
記住我
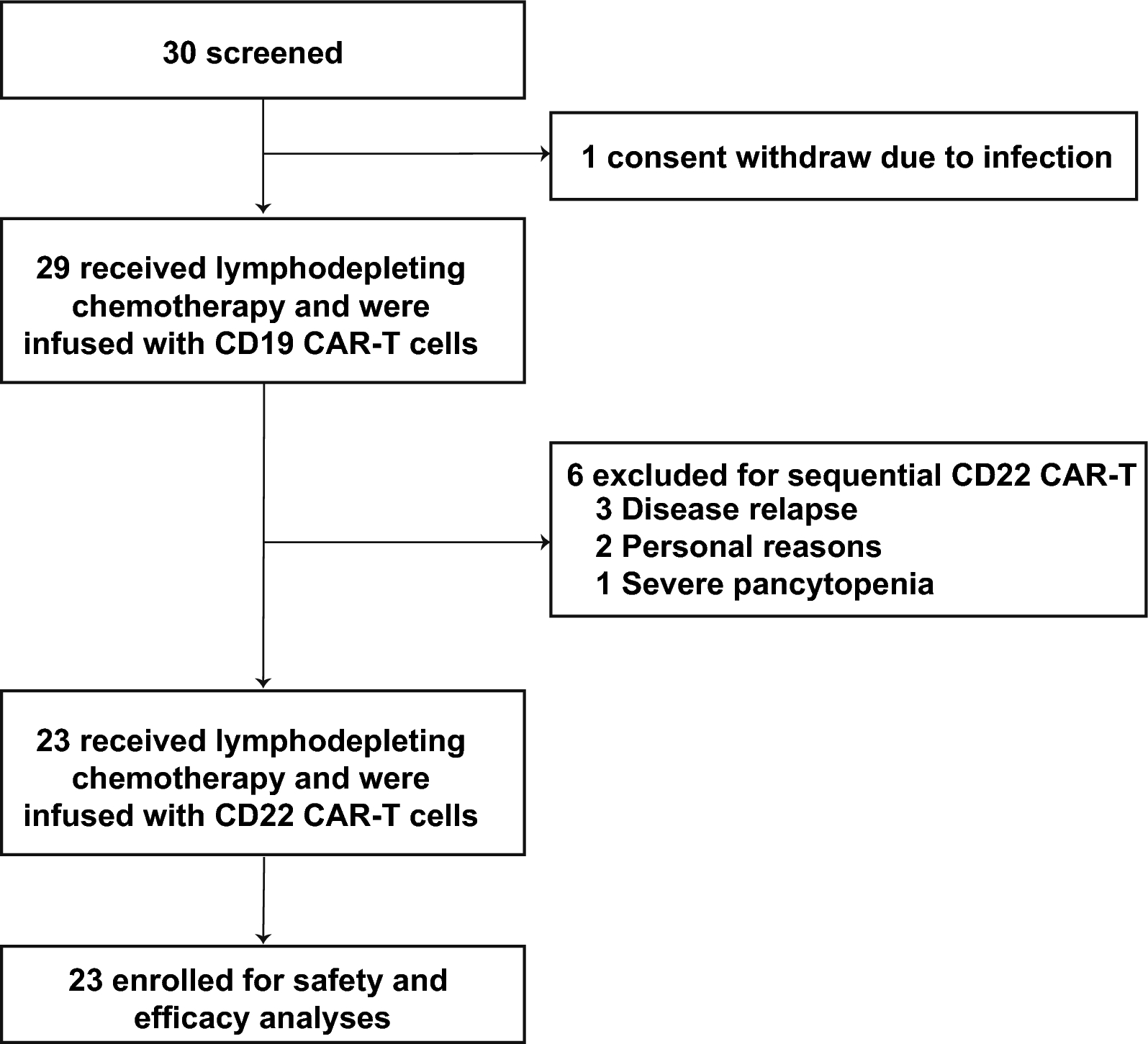


Between November 2020 and November 2023, 30 patients were screened, and 23 were enrolled to receive sequential CD19 and CD22 CAR-T cell therapy (Fig. 1). One patient withdrew due to a severe infection. Six patients discontinued after the CD19 CAR-T cell infusion and did not receive CD22 CAR-T cells due to disease relapse (n = 3), personal reasons (n = 2), or severe AE (n = 1). The baseline characteristics of patients are summarized in Table 1. Of the enrolled patients, 12 (52.2%) were male, and 11 (47.8%) were female, with a median age of 58.1 years (range, 25.9–75.0). High-risk cytogenetic and genomic aberrations were detected in 10 patients (43.5%) (Table S1). BCR-ABL fusion genes were detected in four patients, complex chromosome karyotypes in three patients, IKZF1 alterations in two patients, and TP53 mutation in one patient. Nineteen patients (82.6%) had undergone more than three prior lines of therapy, seven had previously undergone allo-HSCT, and one had previously received dual CD19 and CD22 CAR-T therapy. At enrollment, five patients had EMD: three with isolated diffuse EMD, one with concurrent BM and diffuse EMD involvement, and one with BM and CNS involvement (Table S2). Eight patients received bridging therapy, including bispecific T-cell engager (BITE, n = 6) and chemotherapy (n = 2), to reduce circulating blasts before lymphodepletion (Table S3).
Fig. 1
Diagram of the sequential treatment procedure
Table 1 Baseline characteristics of all enrolled patientsCharacteristics of the infused CAR-T cell productThe median transduction efficiency was 59.7% (range, 10.6–77.9%) for CD19 CAR-T cells and 48.1% (range, 20.7–70.0%) for CD22 CAR-T cells. The median infusion doses were 2.1 × 106 cells/kg (range 0.8–3.6 × 106) for CD19 CAR-T cells and 2.1 × 106 cells/kg (range 1.1–3.0 × 106) for CD22 CAR-T cells. Among the seven patients with a history of allo-HSCT, five received donor-derived CD19 and CD22 CAR-T products (four from haploidentical donors and one from a matched sibling donor), while the remaining two received autologous CAR-T products due to the unavailability of donor T cells (Table S4). A comparison of the two CAR-T cell types revealed that CD19 CAR-T cells had a significantly higher transduction efficiency (P = 0.01), CD4 CAR-T/CAR-T ratio (P < 0.001), and CD4/CD8 CAR-T ratio (P = 0.02), whereas CD22 CAR-T cells showed higher CD8 CAR-T/CAR-T ratios (P < 0.001) than did CD19 CAR-T cells (Table S5). No significant differences in CAR-T product characteristics were observed between patients who achieved ongoing remission and those who experienced relapse (Table S6).
SafetyAll AEs associated with CD19 and CD22 CAR-T cells are presented in Table S7. No treatment-related deaths occurred. Following CD19 CAR-T therapy, hematologic toxicities were the most common grade ≥ 3 AEs, including lymphopenia (100%), neutropenia (91.3%), anemia (52.2%), and thrombocytopenia (52.2%) (Fig. S1A). Among patients with grade 3 or higher cytopenia, 69.6% recovered to grade ≤ 2 lymphopenia, 81.0% to grade ≤ 2 neutropenia, 41.7% to grade 2 anemia, and 50% to grade 2 thrombocytopenia within 1 month after infusion. The median lymphocyte count before the second lymphodepletion was 1.1 × 109/L (range 0.5–5.7 × 109/L), similar to the level before the first lymphodepletion (1.1 × 109/L; range 0.5–4.2 × 109/L) (Fig. S1B). During CD22 CAR-T therapy, grade 3 or 4 lymphocytopenia occurred in all patients, neutropenia in 87.0%, anemia in 21.7%, and thrombocytopenia in 52.2%. One month after CD22 CAR-T infusion, among patients with grade 3 or higher cytopenia, recovery to grade ≤ 2 lymphopenia was observed in 82.6%, neutropenia in 80%, anemia in 40%, and thrombocytopenia in 50%. Red blood cell transfusions were administered to six patients (26.1%) during CD19 CAR-T and three (13.0%) during CD22 CAR-T. Platelet transfusions were administered to five patients (21.7%) following CD19 CAR-T and two (8.7%) following CD22 CAR-T. Infections occurred in seven patients (30.4%) during the first infusion, including pneumonia (n = 4), intestinal infection (n = 1), urinary tract infection (n = 1), and bloodstream infection (n = 1). During the second infusion, six patients (26.1%) developed infections, including pneumonia (n = 3), intestinal infection (n = 2), and bloodstream infection (n = 1). All infections were successfully resolved. After CD19 CAR-T cell infusion, no patient experienced Epstein-Barr virus or cytomegalovirus (CMV) reactivation. After the CD22 CAR-T infusion, only one patient developed CMV reactivation.
CRS occurred in 18 patients (78.3%) during CD19 CAR-T cell therapy, including seven (30.4%) with grade 1, nine (39.1%) with grade 2, and two (8.7%) with grade 3 CRS. The primary manifestation of CRS was fever, with only one patient exhibiting localized facial swelling, which was considered focal CRS. The median onset and duration of CRS were 4 days (range 1–10) and 6 days (range 2–13), respectively. All grade 1 CRS cases and two grade 2 CRS cases were managed with symptomatic treatment; two grade 2 CRS cases received only steroids, while five grade 2 CRS cases and two grade 3 CRS cases were treated with steroids and tocilizumab. After CD22 CAR-T, nine patients (39.1%) experienced CRS (grade 1, n = 3; grade 2, n = 6), with a median onset and duration of 1 day (range 1–5) and 5 days (range 3–14), respectively. No CRS of grade 3 or worse was documented. One patient received steroids and tocilizumab, two received steroids alone, and six received symptomatic treatment. In both infusions, patients with higher-grade CRS (≥ grade 2) had significantly higher peak concentrations of serum interleukin-6 (IL-6), IL-10, interferon-γ, and C-reactive protein than did those with low-grade CRS or without CRS (grade 0–1 CRS) (Fig. S2). The IL-6 levels in patients with CRS ≥ 2 during CD19 CAR-T therapy were significantly higher than those in patients with CRS ≥ 2 during CD22 CAR-T therapy (P = 0.03), while no significant differences were observed for other cytokines (Fig. S3). Baseline BM disease burden was comparable between patients with grade ≥ 2 CRS and those with grade 0–1 CRS during CD19 CAR-T infusion (P = 0.12) (Fig. S4). Two patients developed grade 2 immune effector cell-associated neurotoxicity syndrome (ICANS), mainly manifesting with drowsiness, confusion, sluggish responses, and incoherent answers. One of whom had CNS leukemia (CNSL) and developed ICANS with concomitant grade 2 CRS. The onset of ICANS was observed at 6 days and 16 days post-infusion, with both cases lasting for 2 days each. Symptoms resolved without clinical sequelae. No ICANS was reported during CD22 CAR-T cell therapy.
EfficacyFollowing CD19 CAR-T cell therapy, the overall response rate was 100%, with all patients achieving MRD-negative (MRD−) CR. After sequential infusions, two patients received one course of sintilimab as consolidation therapy, and three BCR-ABL-positive patients continued taking tyrosine kinase inhibitors. With a median follow-up of 19.4 months (range 8.7–45.6), 15 patients (65.2%) were alive, and 14 (60.9%) remained alive in molecular remission without further treatment (Fig. 2A). Eight patients died during follow-up owing to infectious shock (n = 4), disease progression (n = 3), and HSCT-associated complications (n = 1). The median OS was not reached, and the median LFS was 20.8 months. The OS rates were 91.3% (95% confidence interval [CI], 80.5–100%) at 1 year and 58.6% (95% CI 38.7–88.8%) at 2 years (Fig. 2B). The 1-year and 2-year LFS rates were 67.1% (95% CI 49.5–90.9%) and 47.0% (95% CI 28.2–78.4%), respectively (Fig. 2C).
Fig. 2
Clinical outcomes. A Swimmer plot showing the duration of response and survival outcomes post-infusion for all treated patients (n = 23). CR/CRi, complete remission/complete remission with incomplete hematologic recovery; MRD−, minimal residual disease-negative. B, C Kaplan–Meier estimates of overall survival (OS, B) and leukemia-free survival (LFS, C) in all patients. D, E Kaplan–Meier estimates of OS (D) and LFS (E) in patients without extramedullary disease (EMD) (n = 18) versus those with EMD (n = 5). F Cumulative incidence of relapse in all patients. G Cumulative incidence of relapse in patients without EMD versus those with EMD
Eight patients experienced leukemia relapse: six (75.0%) with CD19+CD22+ relapse, one (12.5%) with CD19−CD22+ relapse, and one (12.5%) with CD19−CD22− relapse (Fig. S5A and Table S8). There were six cases of BM relapse, one of isolated extramedullary relapse, and one of coexisting BM and CNSL relapse (Fig. S5B). The median time to relapse following CD19 and CD22 CAR-T cell infusion was 8.5 months (range 5.1–20.8) and 4.2 months (range 2.1–16.7), respectively. CIR at 1 year and 2 years were 28.6% and 42.5%, respectively (Fig. 2F).
Among the five patients with EMD involvement, the extramedullary lesions achieved CR following the initial CD19 CAR-T infusion. After sequential infusions, of the three patients with isolated EMD, one patient succumbed to septic shock 1.3 months after CD22 CAR-T cell infusion. Another patient experienced isolated EMD relapse, with new lesions identified in the kidneys, heart, and tonsils. One patient experienced only BM relapse. In patients with BM and extramedullary involvement, one had BM relapse, while another had both BM and CNS relapse. The median time to relapse was 9.4 months (range 5.1–14.4) following CD19 CAR-T cell infusion and 5.4 months (range 2.6–10) following CD22 CAR-T cell infusion. Patients with EMD had inferior OS (P = 0.032) and LFS (P < 0.001) (Fig. 2D–E). A significantly higher CIR was observed in patients with EMD compared to those without EMD (P = 0.02) (Fig. 2G).
Kinetics of CAR-T cellsThe full kinetic profiles of circulating CAR-T cell levels, measured by flow cytometry in patients over time, are shown in Fig. 3A and B. CAR-T cell expansion was observed in all patients throughout the treatment cycles. During the first infusion, rapid CAR T-cell expansion was observed with a median time to peak of 11 days (range, 7–19) and a median peak level of 353.2 cells/μL (range, 30.6–2902.1) (Fig. 3C). Prior to CD22 CAR-T therapy, the median level of CD19 CAR-T cells was 1.8 cells/μL (range, 0–89.8), and the median percentage of CD19 CAR-T cells in PB lymphocytes was 0.9% (range, 0–17.5%) (Fig. S6A and B). During the second infusion, the median peak CAR T-cell expansion occurred on day 9 (range, 4–21), with a median peak level of 34.5 cells/μL (range, 0.8–6415.4) (Fig. 3C). Despite the comparable infusion doses of CD19 and CD22 CAR-T cells, the peak CAR-T cell levels were significantly higher in the first cycle than in the second cycle, indicating a more robust initial expansion. Peak CD22 CAR-T cell levels were lower in patients who experienced relapse than in those in remission (P = 0.06), and peak CD19 CAR-T cell levels showed no significant difference between the two groups (P = 0.29) (Fig. 3D). No significant differences in both CAR-T cell expansion were observed among the different CAR-T product sources (Fig. 3E). Further investigation of the correlation between EMD and peak CAR T-cell expansion revealed no significant correlation with either CAR-T infusion (Fig. S7). Among the 8 relapsed patients, CAR-T cells were undetectable by flow cytometry.
Fig. 3
Dynamics of CAR-T cell expansion and comparison of peak CAR-T levels. A Expansion of CAR-T cells over time post-infusion in all patients. B CAR-T cell expansion between autologous and donor-derived CAR-T cells. C Peak CAR-T cell levels and the number of days to reach peak expansion. D Peak CD19 CAR-T cell levels (top) and peak CD22 CAR-T cell levels (bottom) between patients with ongoing remission and those who relapsed. E Peak CD19 CAR-T cell levels (top) and peak CD22 CAR-T cell levels (bottom) between autologous and donor-derived CAR-T cells
BCABCA in the PB or BM was observed in all patients 1 month after CD19 CAR-T therapy. Before the second CAR-T cell infusion, the median B-cell percentage in peripheral lymphocytes was 2.1% (range, 0.15–26.1%) (Fig. S6C). Twelve patients had sustained BCA, while eleven had B-cell recovery with a median percentage of 6.5% (range, 3.3–26.1%) of peripheral lymphocytes. Of the 14 patients with durable responses, three (21.4%) maintained BCA for longer than 6 months following CD22 CAR-T cell infusion. The remaining 11 patients experienced B-cell recovery with a median time of 2.8 months (range, 1.2–5.8) after CD22 CAR-T infusion. Among the eight patients with relapse, loss of BCA preceding relapse was observed in three cases (37.5%), concurrent loss of BCA and relapse in four cases (50%), and ongoing BCA in one case (12.5%). For MRD−CR patients with follow-up exceeding 6 months after CD22 infusion, immunoglobulin recovery at the cut-off date was observed in six cases (75.0%) for IgM, five (62.5%) for IgA, and five (62.5%) for IgG.
Multivariate analysesMultivariate analyses for clinical outcomes were conducted (Table 2). A higher leukemia burden at baseline (≥ 64% blast cells in BM) was an independent prognostic factor correlated with shorter OS (hazard ratio [HR], 5.9; 95% CI 1.3–26.7, P = 0.021). Multivariable analysis for LFS revealed that the presence of EMD at baseline contributed significantly to inferior LFS (HR, 8.9; 95% CI 2.1–37.7; P = 0.003). Conversely, patient age, sex, risk stratification, prior lines of therapy, interval between the two CAR-T infusions, and loss of BCA before CD22 CAR-T cell infusion were not predictive of OS or LFS.
Table 2 Univariate and multivariate analysis of factors influencing OS and LFS
留言 (0)