Study design and setting
A facility-based cross-sectional study was conducted among lactating mothers visiting child immunizations and postnatal care units in public health facilities in Girawa District from January 20 to February 20, 2023. The Girawa District is found in the East Hararghe Zone, Oromia Regional State, Eastern Ethiopia, 580 km from Addis Ababa, the capital city of Ethiopia and 75 km from Harar (zonal city). According to the Girawa District Health Office report, there were 14,652 lactating mothers in 2022. The district has one hospital, nine health centers and 45 health posts. The major food products of the district are cereals, including maize, sorghum, teff, wheat, and barley; pulses, such as beans, peas, lentils and other legumes; vegetables, such as potato, sweet potato, spinach, lettuce, cabbage, and pumpkin; and fruits, including mango, avocado, banana and oranges [32].
Population and sampling
Lactating mothers who live in Girawa District, Eastern Ethiopia were source populations whereas among lactating mothers those who visited child immunizations and postnatal care units of public health facilities were the study participants for this study. Lactating mothers who were severely ill were excluded from the study.
The sample size for the magnitude of inadequate consumption of vitamin A-rich foods was estimated by using the single population proportion formula \(\:n=\frac/2)2\text\text}2}\), with the following assumptions: the magnitude of inadequate consumption of vitamin A-rich foods among lactating mothers (p) from previous study conducted in Northwest Ethiopia which is 61.1% [21], the 95% confidence level (Zα/2) was 1.96, and the degree of precision (d) was 0.05 and 10% for nonresponse. Accordingly, the sample size was 402. The sample size for the factors associated with inadequate consumption of vitamin A-rich foods was calculated by using EPI-Info version 7 Statistical Software considering the following assumptions: 95% confidence level, 80% power of the study, and unexposed to exposed ratios of 1:1 and 10% for the nonresponse rate which resulted in a sample size of 422. The sample size calculated for the associated factors yielded a larger sample size. Thus, the final sample size of this study was set at 422.
From the 10 total public health facilities, six health facilities (Garamuleta General Hospital (GMGH), Girawa Health Center (GHC), Dogu Health Center (DHC), Lafto Health Center (LHC), Oromitu Health Center (OHC) and Melba Health Center (MHC)) were selected randomly using the lottery method. The calculated sample size was proportionally allocated to the selected health facilities (202 to GMGH, 115 to LHC, 150 to GHC, 108 to OHC, 166 to DHC and 90 to MHC) based on the average number of clients who flow to the child immunization and postnatal care units during the three months prior to the study. The study participants were then selected by a systematic random sampling method. The calculated sampling interval (k) for each selected health facility was two. The first study participant for each health facility was selected by the lottery method, and then sampling continued every two participants until the required numbers of samples were achieved.
Data collection methods
An interviewer-administered questionnaire was developed for this study (Additional file 1), thereby reviewing different previous literatures [30, 33,34,35]. The questionnaire was, then, structured into the following seven sections: [1] sociodemographic characteristics [2], nutrition knowledge of lactating mothers [3], consumption status of vitamin A-rich foods by lactating mothers [4], dietary diversity status of lactating mothers [5], household food security status [6], health services and health conditions of lactating mothers, and [7] water, hygiene and sanitation. Six data collectors—one diploma nurse, two BSc nurses and three BSc midwives—who fluently speak Afan Oromo (the local language) and who were working outside of the study facility—were involved in the data collection. Two supervisors (one BSc midwife and one public health officer), who were familiar with the study setting, supervised the data collection.
The consumption of vitamin A-rich food was assessed using the Helen Keller International food frequency questionnaire (FFQ) with modifications to the local context. The Helen Keller International food frequency method assesses the extent to which communities and populations are at risk of VAD. If at least 70% of the surveyed people are not above the threshold values (had inadequate consumption of vitamin A-rich foods), VAD is likely to be a public health problem in the entire study area [35]. The FFQ asks respondents how many days in the past week they ate the foods listed on a predesigned FFQ. The tool has twenty-eight different food items. Among the twenty-eight food items, twenty-one are available in the study area and are consumed by society. Only major sources of vitamin A (≥ 100 RE) were taken into consideration. The foods selected for the analysis of the consumption of foods rich in vitamin A included dark green leafy vegetables (DGLVs), carrots, pumpkins, mangos, papayas, sweet potatoes, palm oils, eggs, fishes, livers, and butter.
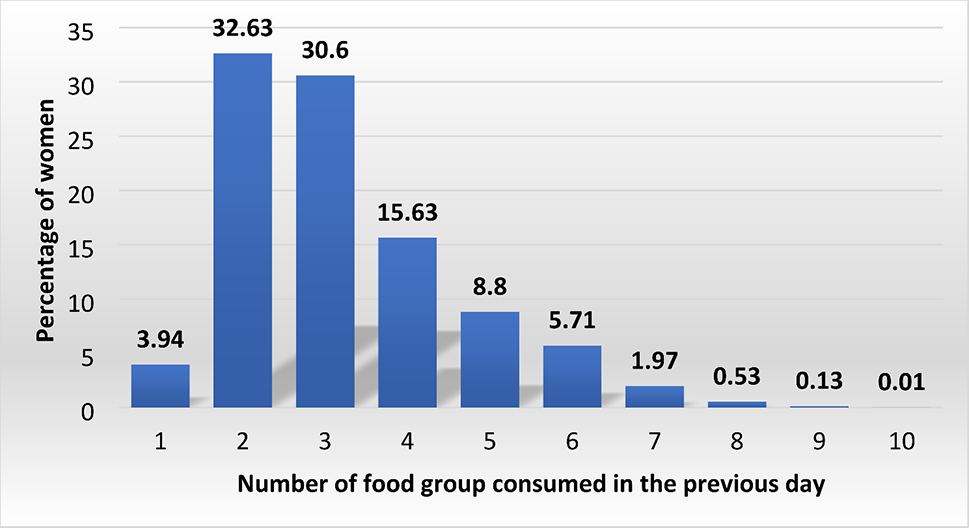
Maternal dietary diversity was measured by the minimum dietary diversity for a woman, which is a dichotomous indicator/tool that was developed by the FAO. The maternal dietary diversity score was calculated as the sum of the number of different food groups consumed by the mother in the 24 h preceding the survey. A total of ten food groups were considered in this study: [1] grains, roots, tubers and plantains; [2] pulses (beans, peas and lentils); [3] nuts and seeds; [4] milk and milk products; [5] meat/poultry and fish; [6] eggs; [7] DGLVs; [8] other vitamin A-rich fruits and vegetables; [9] other vegetables; and [10] other fruits. Mothers who consumed a minimum of five out of the ten food groups within a 24-hour recall period were considered to have adequate dietary diversity [30].
Food insecurity was measured by the Household Food Insecurity Access Scale (HFIAS), which consists of nine occurrence questions that represent a generally increasing level of severity of food insecurity (access) and nine frequency-of-occurrence questions that were asked as a follow-up to each occurrence question to determine how often the condition occurred during the previous 4 weeks [34]. Nutrition knowledge was assessed using a scoring system based on responses to 9 nutrition-related standardized questionnaires with both close and open-ended questions [33].
Operational definitions
Inadequate consumption of vitamin A-rich foods
Intake of animal sources of vitamin A for ≤ 4 days per week or consumption of a weighted source (total intake of animal and plant sources of vitamin A) for ≤ 6 days per week [35].
Minimum dietary diversity for women
Intake of at least five food groups out of 10 food groups [30].
Food insecurity
A situation that occurs when people lack secure access to sufficient amounts of safe and nutritious food for normal growth and development and an active and healthy life [36].
Based on the total HFIAS score, household food insecurity can be categorized into four levels:
food secure—if the household scores 0 or 1, mild food insecure—if the household scores from 2 to 8, moderate food insecure—if the household scores from 9 to 16, severe food insecure—if the household scores from 17 to 27 [34].
Adequate nutritional knowledge
Lactating mothers who score 7–9 on the basis of nine nutrition-related standardized questionnaires with both close- and open-ended questions.
Fair nutritional knowledge
Lactating mothers who score 4–6 on the nine questions.
Poor nutritional knowledge was defined as follows
Lactating mothers who scored between 0 and 3 on one of nine questions [33].
Data quality control
To maintain the accuracy and consistency of our data, the questionnaire was translated to the local language (i.e., Afan Oromo) and was pretested on 5% of the total sample size two weeks before the actual data collection. Modifications were made on the questionnaire based on the findings of the pretest. The data collectors and supervisors were trained for two days on the data collection process. The collected data were checked daily for consistency and completeness. Double data entry was performed, and the data were cross-checked to ensure consistency. The principal investigator and supervisors coordinated the overall data collection process.
Data processing and analysis
The collected data were coded, cleaned, and entered into the EpiData version 3.1 software package and exported into STATA version 17 for analysis. Data cleaning was performed to identify outliers/inconsistencies, errors and missing values. Both descriptive and analytical statistics were done. Descriptive statistics such as the mean (with standard deviation) and median (with interquartile range) for continuous data as well as frequency and percentage for categorical data were used to describe the characteristics of participants using tables, figures and text.
To determine the association between the independent variables and the outcome variables, both bivariable and multivariable logistic regression analysis was performed to determine the factors associated with inadequate consumption of vitamin A-rich food sources. Variables with a P value < 0.25 in a bivariable logistic regression analysis were retained and entered into a multivariable logistic regression to control for the potential confounding variable that affects the measurable outcome variable. The model goodness-of-fit test was checked by using the Hosmer and Lemeshow test (p value = 0.11). Finally, a P value < 0.05 and an AOR calculated with 95% CI were used to determine the presence of statistical significance.





留言 (0)