In this comprehensive analysis of MM disparities across different continents, we sourced global MM patient report data from the openFDA Human Drug Adverse Events endpoint, a dataset encompassing diverse patient-related information. Similar to a study that observed declines in early mortality in all MM patients including those younger than 65 years and older than 65 years [20], our findings revealed distinct characteristics in mortality but ultimately demonstrated a decreasing trend across continents. Differences in various reported outcomes could be due to various factors related to disparities including utilization and availability of different drug regimens in different regions. In terms of age and gender distribution, the male-to-female ratios were consistent across regions, with slight regional variations.
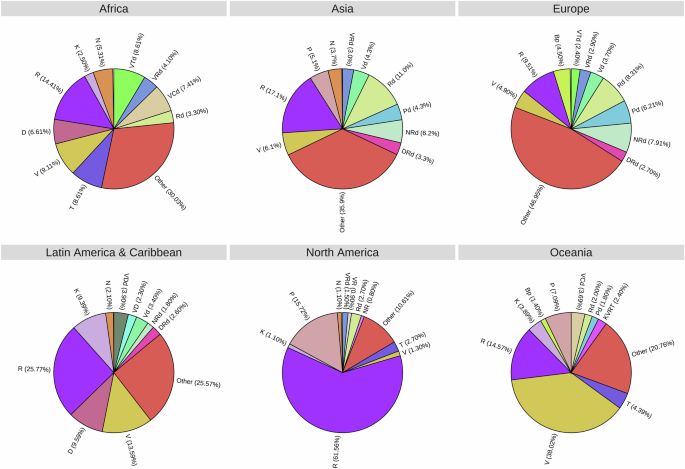
In the MM Research Foundation (MMRF) CoMMpass study via NCI’s Genomic Data Commons Data Portal, the largest MM dataset in the public domain, d, R, and V are the top three drug components in combination therapy [21]. However, in our dataset, R emerged as the most frequently reported drug, followed by glucocorticoids, V, and P among all regions. Notably, T, D, K, and cyclophosphamide-based regimens were also used frequently. To account for multiple drugs within a single report, we grouped drugs into regimens across six different regions. Single use of R was highly prevalent in NA, whereas in the EU, drug regimens were more diverse, NRd, Pd, Rd, and R consist of AEs in the United Kingdom and France as the top two countries of report AEs in the EU. Nevertheless, R or R-related regimens remained dominant in the EU, while in other regions, single use of R was consistently the most widely used drug.
According to the FDA, death, and hospitalization are two serious outcomes in patient reports, however, the occurrence of one or more deaths and hospitalization in a report does not necessarily mean that drug was the cause of these two serious outcomes [22]. Our findings revealed intriguing trends in death rates and hospitalization rates of MM patients over time, as depicted in Fig. 3. The descending bubbles in Fig. 3 symbolize a marked improvement in survival rates, particularly in AS, EU, and NA. The introduction of novel therapies significantly improved survival rates for MM patients in the US, evident in data from both the Mayo Clinic and the Surveillance, Epidemiology, and End Results (SEER) program over a 14-year period [23]. A study also showed that survival rates for MM patients in Germany have improved remarkedly since 2000 due to the novel therapeutic [24]. Based on our findings, death rates (mean value of 27%) exhibited fluctuations with no drug regimen usage exceeding 10% of total reports in the EU. It is important to highlight the variability in drug availability or use across the EU. AS experienced an initial decrease in death rates until 2012, followed by an ascending trend until 2016. However, it witnessed a substantial drop to the lowest value of 27.1% in 2022. Significant variations in death and HR were also observed in AF, LA, and OC, primarily attributed to the limited number of cases reported from these regions. In AS and EU, hospitalization rates displayed comparatively less variation over time, whereas NA saw a decline in HR. These intriguing trends in death and hospitalization rates underscore the multifaceted nature of MM disparities across different continents and emphasize the importance of further research in this domain, leveraging advanced technologies like artificial intelligence (AI) and machine learning, as demonstrated in different studies [16, 17, 25, 26].
A previous analysis focusing on MM outcomes across different races and ethnicities in the US aligns with the disparities observed in our mortality and hospitalization data across continents [8]. This study revealed significant variations in MM diagnosis and outcomes, highlighting that Hispanics were diagnosed at the youngest median age, while Whites were at the oldest median age. Age at diagnosis emerged as an independent predictor of OS and MM-specific survival, suggesting that demographic and possibly genetic factors may influence MM outcomes and would have implications on access and utilization of healthcare. Similarly, in our analysis, we observed variations in mortality and HR across different continents, which are likely due to differences in healthcare delivery, drug access, supportive care strategies, and patient demographics. The observation that Asians exhibited the most favorable median survival in the prior study aligns with the trends seen in our data, where some regions, like AS and EU, showed lower mortality and HR compared to others, while Hispanics faced the least favorable outcomes.
Our study has also shown a higher prevalence of AE reports in males versus females. These differences could be due to multiple factors, such as subjective differences in reporting including gender-related differences in symptom perception, reporting and interpretation of AEs, body composition variations, differences in sex hormones, and changes in pharmacokinetics, pharmacodynamics, and pharmacogenomics. To ensure that clinically relevant differences are not overlooked, the relationship between dose, efficacy, and toxicity should be evaluated separately in men and women, using data from large clinical studies and pooled analyses. Zavala et al. highlighted health disparities in various racial and ethnic minority populations in the US and underscored the ongoing persistence of inequities despite concerted efforts to understand their root causes [27]. This notion reverberates with our findings, which show disparities in MM mortality and HR across continents, which are likely significantly due to variability in care, but also likely indicate inequities in healthcare access and outcomes, which persist on a global scale. In a study led by Baughn et al., the role of cytogenetic abnormalities in driving racial disparities in MM was explored [28]. Their findings suggested that a significant proportion of the racial disparity in MM outcomes could be attributed to variations in the occurrence of specific cytogenetic abnormalities, such as t(11;14), t(14;16), and t(14;20) types of MM. While our data did not directly assess genetic factors, the geographic disparities in MM outcomes observed in our analysis might reflect a combination of genetic, demographic, and healthcare-related factors that warrant further investigation [29].
Atkins et al. conducted a retrospective cohort study involving over 340,000 patients diagnosed with lung cancer between 2000 and 2006 [30]. They gathered data from various geographical areas in the US, including metropolitan, urban, suburban, and rural areas, utilizing the SEER Program database and found that the increase of lung cancer mortality correlated with dosage and rurality across rural-urban regions. Xu et al. employed the SEER database to identify patients with hepatocellular carcinoma (HCC) in the US between 1998 and 2012 [31]. Their research highlighted significant racial differences in presentation, treatment, and survival among HCC patients. Further research is essential to gain a better understanding of the socio-demographic and biological factors contributing to racial disparities in care.
Recently, chimeric antigen receptor T Cells (CAR-T) have emerged as a promising treatment for managing relapsed-refractory MM (RRMM) [32]. This therapy involves a complex process and treatment is usually given in large academic institutions after a robust selection process. All CAR-T centers use tools for selection criteria, selection timelines, and priority scores. Kourelis et al. explored the issue’s scope and examined how major medical centers were tackling the challenges associated with the allocation of manufacturing slots for CAR-T therapy [33]. This approach would not only streamline access to CAR-T therapy but also safeguard the needs of both current and future patients and physicians for utilization of such resource-intensive therapeutic options. Recently, Peres et al. collected data from several institutions across the US that provided CAR T-cell therapy for MM patients and found non-Hispanic Black (NHB) patients are likely to develop any grade Cytokine release syndrome compared Hispanic and NHW patients [34]. Possible reason attributed to high CRS is due to an elevated proinflammatory state among NHB patients before CAR-T cell therapy. Three T cell redirecting bispecific antibodies (Teclistamab, Elranatamab, Talquetamab) are now approved for the management of RRMM [32], however, these drugs are mostly available in academic centers in developed countries. Outside of the USA, there is variability in access and scarcity of newer drugs and cellular therapies in many regions.
In conclusion, the pronounced disparities in health outcomes among different populations present significant moral and public health concerns. While our research sheds light on the multifaceted nature of these disparities and advocates the pivotal role of social and economic factors, it is evident that new technologies like AI and machine learning will be instrumental in shaping our future understanding of these complex issues. Studies such as Gao & Cui et al. or Meng et al. have demonstrated the potential of AI and machine learning to uncover critical insights into population-level disparities [16, 17]. Striking data highlights the fundamental influence of social factors on health outcomes, exemplified by studies that examined the impact of socioeconomic and race on MM survival in the US [35]. The understanding of MM disparities will undoubtedly require an interdisciplinary approach that considers the interplay of genetics, socioeconomic factors, and advanced technologies, ultimately guiding us toward more equitable and effective healthcare solutions.
Limitations
One limitation inherent in our present study is its retrospective nature, as it relies on the analysis of curated ADE databases from reporting systems [36,37,38,39]. The natural confounding of age and medical comorbidities on MM-related outcomes is frequently encountered in attempts to discern the impact of medications on clinical outcomes. This challenge is exacerbated by the fact that older adults are more likely to be affected by MM and age-related comorbidity. The OpenFDA datasets have many limitations for pharmacovigilance research. These include underreporting of AEs which can result in incomplete information on the true occurrence of AEs, particularly in regions with fewer reported cases or where there is a higher incidence of severe AEs. Severe or unusual AEs are more likely to be reported than common, mild ones, which are more prevalent in openFDA, contributing to a skewed safety profile. Confounding factors are also difficult to disclose within the openFDA. Further limitations include a lack of comprehensive clinical data, which can impede the assessment of trends, the accurate estimation of true AE occurrences, and the availability of clinical context. Additionally, there may be selection biases arising from the non-random selection of patients exposed to the drug or the inaccurate selection of contributors from distorted spontaneous reports. These biases may be driven by covariates other than the drug under investigation, such as a patient’s disease stage, delay in diagnosis, or disease duration. To address these bias-related challenges, we implemented comprehensive data validation procedures and statistical methods to enhance the accuracy and completeness of the reported AEs. We also standardized the reporting framework to minimize inconsistencies and biases within the dataset. Complementing these efforts, a longitudinal review of available data enables us to track temporal trends over time, allowing for a more nuanced understanding of AEs.
Moreover, several other confounding variables prevalent in cancer studies involving spontaneous reporting systems can introduce potentially detrimental bias or variation. Due to the limited information available, a comprehensive meta-analysis of the observational evidence concerning the source, magnitude, and impact of these factors remains inconclusive [36,37,38,39,40,41,42].
Future directions
Our findings have shown that global disparities in myeloma care result in poorer outcomes in low- and middle-income countries due to limited access to novel drugs, and specialized healthcare professionals, highlighting the need for better resources and access to new therapies.
We recommend advocating for policies that promote equitable access to resources and care for underserved populations. Most importantly, global and governmental measures to address fundamental issues such as poverty, increased government spending on health care (including cancer care), and provision of universal basic health care are critical to cancer care globally. Global and governmental efforts are crucial for improving health care funding for cancer care, as well as providing universal health care to ensure access to high-quality cancer care treatment worldwide. For clinical practice, health practitioners could enhance awareness and improve patient outcomes by understanding different AE patterns across the globe. For future research, we suggest conducting longitudinal studies to assess the long-term impacts of myeloma drug therapies, understanding race, social and biological factors of drug disparity from the pooled analysis, and conducting more clinical trials in low-income countries.




留言 (0)