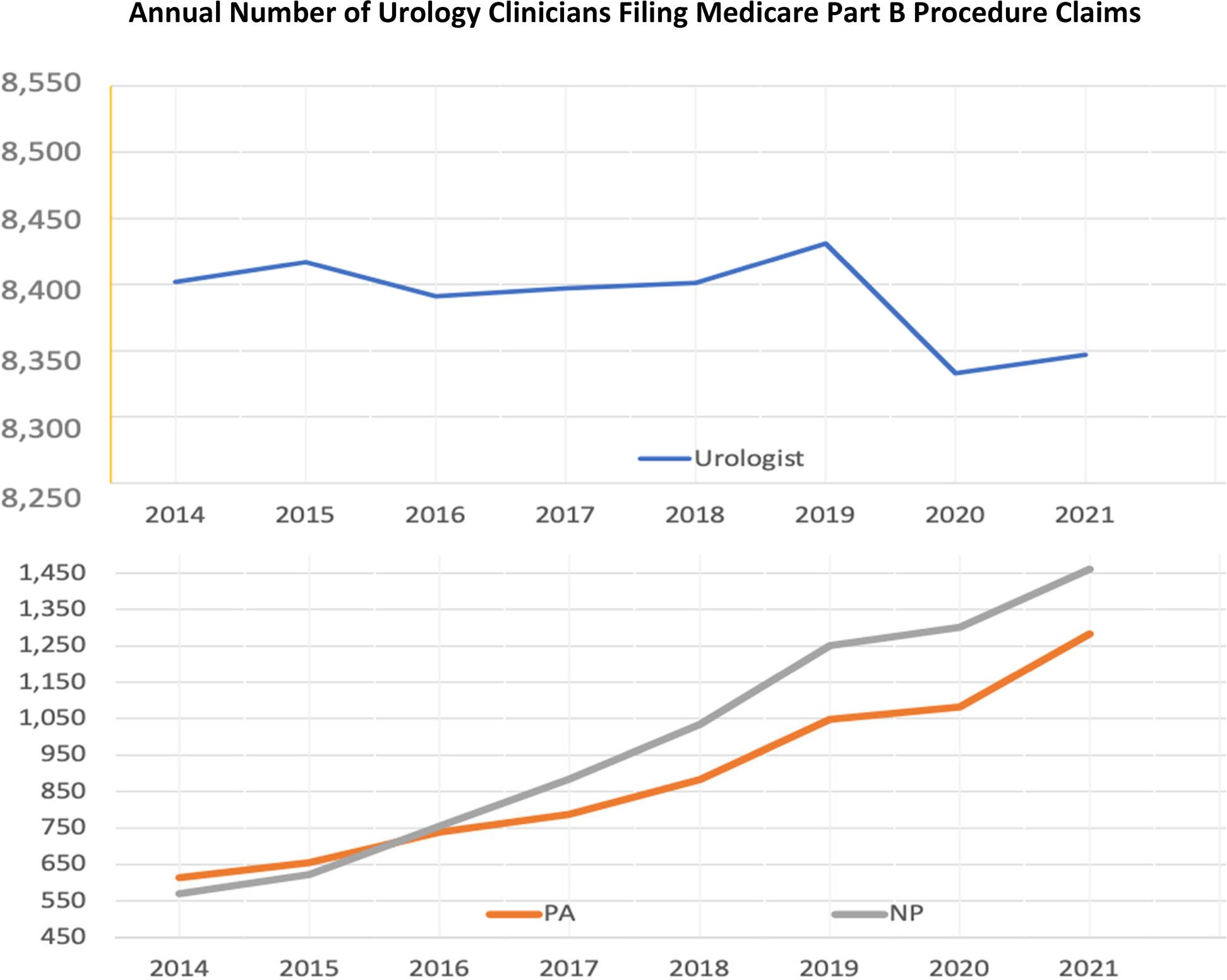
Several important trends in urological medicine in older adults are observed, and prominent in this analysis is the redistribution of the tasks of outpatient procedures to PAs and NPs. Another observation was that the number of urologists filing outpatient Medicare Part B claims in this specialty declined. National health labor trend analyses find that the physician and surgeon ratio per population is becoming leaner [9]. Third, the demographics of the US population compounded this demand. As the number and proportion of older people has grown, there has been an increase in the incidence and prevalence of urological diseases [10]. Lower urinary tract symptoms are more prevalent among the elderly, and clinical urodynamic studies have demonstrated that advancing age is associated with reduced bladder capacity, increased uninhibited contractions, decreased urinary flow rate, and diminished urethral pressure profile [10].
Urology is a growing specialty among PAs and NPs, mirroring the spectrum of American medicine, which employs significantly more to fill labor voids in highly specialized medical professions [11]. As of 2022, 1,199 PAs reported they were employed in urology, representing approximately 1% of all clinically active PAs (N = 116,549) [12]. Absent a similar registry for NPs, the AUA identified 209 urological NPs in 2022 [13]. Most PAs work in general urology, while NPs are reported to be more likely than PAs to work in oncology and pediatrics [13].
Most urological practices (87%) are in urban areas [14]. The 2022 AUA census reported 13,976 “practicing urologists” in the US. However, without structural changes in the contemporary workforce, the availability of board-certified/eligible urologists is forecasted to worsen without significant adjustments to the number of residents trained in this specialty [14]. To offset this trend, the AUA includes PAs, NPs, and physician members in surveys [14].
This study reinforces that within one specialty, the medical labor trend of task-shifting and team-based care has been underway for two decades. Task shifting and team-based care are two service delivery areas that interest labor economists as they are a strategy to maximize healthcare delivery [15]. When detailing urology services, the AUA (2023a) reports that PAs and NPs perform various office-based delegated tasks. Some of these procedures include circumcision, cystoscopy, hydrocele aspiration, intravesical Botox, prostate biopsy, and testopel injection [15].
The roles of PAs and NPs in urology appear significant when viewed by the span of procedures and productivity. The AUA (2023a) reports PAs and NPs provide care to a median number of 60 patients per week, work 40 h on clinical duties, and three-quarters are salaried. The difference was that PAs were more likely to assist in significant inpatient operative procedures than their NP counterparts (45.3% vs. 12.4%, respectively). While a similar proportion of PAs and NPs see in-office patients as part of their clinical responsibilities (91.9% vs. 89.5%), proportionately more PAs provide postoperative care than NPs (94.4% vs. 87.6%, respectively). Stefos and colleagues assessed urology activity in an aggregate study of all Veterans Health Administration (VHA) medical centers. They found that the average annual productivity of urology PAs was 2,129 Relative Value Units (RVUs) and NPs 2,055 (RVUs [16]. This assessment of urology PA and NP urology outpatient care was the second highest of the ten most active surgical clinic specialties. The VHA has a long history of using PAs and NPs in outpatient service delivery [17].
Data from the AUA notes that most (88%) of urology NPs and PAs report broad patient access [13]. Concurrently, a satisfaction survey of patients visiting an academic urology clinic staffed with all three clinicians in 2018 produced results that varied depending on the patient’s age, race, sex, and type of visit. Most patients desired to be seen initially by a physician-urologist but were satisfied with the management of their condition by the urology PA or NP afterward [18].
Limitations
All public data in Medicare Part B are based on claims filed by care providers and provide no information about whether the procedure was appropriate or adhered to protocol. For an individual provider to be counted in the public database, at least 11 claims must be filed by that provider that year, which means low-volume procedures per annum were not included. Furthermore, these data only include outpatient claims submitted (i.e., independently billed) by each provider type. While this caveat on federal Medicare data truncates the full extent of publicly available data for a complete analysis, the trend revealed by this investigation is significant as it reflects the growing number of PAs and NPs providing outpatient urological services.
Medicare filings primarily involve older Americans (87%), mainly omitting procedures involving younger adults and children. Medicare is an essential public health insurance scheme for U.S. adults 65 years and over, and at least 96% of all older citizens are enrolled in Medicare. At the same time, urology conditions are more prevalent in older adults than in any other age group. The need for more public data to compare the division of labor in specialized medical and surgical settings that employ all three types of clinicians grows. The absence of such data hampers more refined analyses.
Another nuance of federal data is that urologists are listed explicitly in Medicare B, as are 20 select physician and surgeon specialties. However, PAs and NPs are not listed by specialty but instead generically. The need for a national specialty file for PAs and NPs would improve understanding of how this cadre cares for and shares the roles and duties of disease management across all specialties. The generic assignment of PAs and NPs without delineating their specialized role occurs throughout the federal system, including the National Center for Health Statistics, Centers for Medicare and Medicaid, and Federal Bureau of Workforce Analysis (https://bhw.hrsa.gov). The Bureau of Labor Statistics also generically lists PAs or NPs [9]. At the same time, the NPI distinguishes the physician’s specialty in these federal databases, not the PA or NP. This omission of specialty is considered a significant oversight and inhibits a more robust accounting of medical and surgical care nationwide.









留言 (0)