Resection of the tumor is the only potentially curative treatment of pancreatic cancer. In the context of left or total pancreatectomy removal of the spleen is often performed due to the anatomical proximity of the spleen to the pancreatic tail and affection of the splenic vessels by the tumor. Spleen preservation can either be performed through sparing of the splenic artery and vein or by vessel resection. The preservation of the splenic vessels can be surgically challenging, especially in malignant pancreatic disease, where tumor free resection margins are a pivotal factor for patient outcome. In 1988 Warshaw originally described a pancreatic resection technique with preservation of the spleen but resection of the splenic vessels, based on the preservation of the short gastric- and the left gastroepiploic vessels taking advantage of splenic collateral blood flow [5]. Today, multiple studies have proven the safety and effectiveness of this procedure in open and laparoscopic surgery with no differences in early postoperative outcome [6, 13,14,15,16]. Our findings align with this conclusion, as we could not identify any disparities in postoperative morbidity and mortality (see supplementary Fig. 2). Additionally, no significant differences were observed in terms of operative time or perioperative blood loss in the patient cohort under investigation. In total pancreatectomy, where spleen preservation is most challenging, we observed a shorter operation time compared to simultaneous splenectomy, although this difference did not reach statistical significance. This is probably due to the fact that the Warshaw technique was performed in all cases, eliminating the need for time-consuming exposure of the splenic vessels.
Besides technical reasons, a radical lymph node dissection, including the lymph nodes in the hilus of the spleen, is a reason for splenectomy in pancreatic cancer surgery, especially because nodal involvement is directly correlated with patient outcome. In our study we did not observe any difference between in the number of examined and affected lymph nodes between the splenectomy and no splenectomy group. This is in line with a retrospective analysis of lymph node involvement in patients who underwent total splenopancreatectomy by Collard et al., who found a low median number of only two lymph nodes in the splenic hilus, with 40% of the patients with no lymph nodes detectable at all. None of the hilus lymph nodes were positive for metastasis in this study [8]. Navez et al. described only one case of positive lymph node metastasis in a group of 85 patients with pancreatic adenocarcinoma of the body or the tail, and Kim et al. reported four positive hilar lymph nodes in a cohort of 97 cases of pancreatic cancer [9, 10].
Further, direct infiltration of the spleen by pancreatic tumors of the tail presents a reason for splenic removal. It has been shown that this can be reliably predicted in the preoperative CT [8]. Therefore, cases for potential spleen preservation should be preoperatively assessed for direct splenic infiltration. In our patient cohort, we did not observe any difference in the residual tumor/margin status between the splenectomy and no splenectomy group.
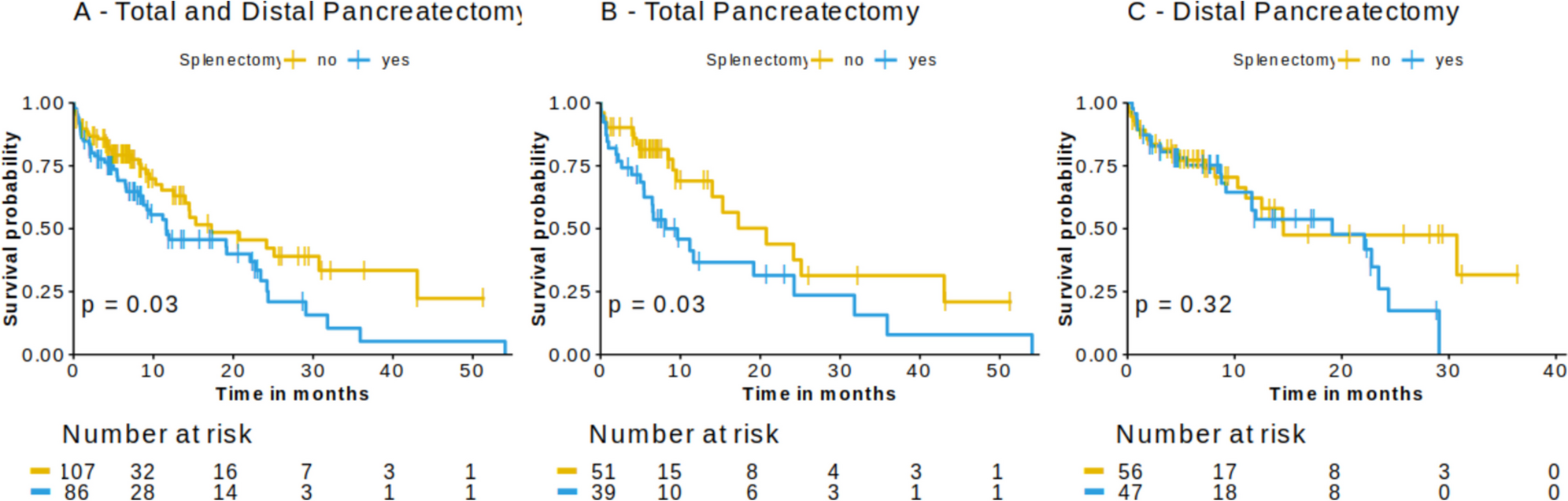
In a large cohort study of cancer-free veterans by Kristinson et al., splenectomy was associated with an increase in cancer incidence and risk of cancer death [17]. This observation was confirmed by Sun et al. in their population-based cohort study of patients undergoing splenectomy for traumatic and nontraumatic indications [18]. In both groups, splenectomy was associated with a higher risk for overall cancer development [18]. When splenectomy was a part of tumor resection of patients with colorectal or esophageal cancer, it was associated with poorer patient prognosis [1, 2]. In pancreatic cancer, Schwarz et al. reported a significantly prolonged survival of patients who underwent a spleen-preserving operation for pancreatic cancer with curative intention. These results are in line with our data; however, Schwarz et al. included distal and total pancreatectomies, and additionally pancreatic head resections (pancreatoduodenectomy). They reported a median survival of 12.2 versus 17.8 months in the splenectomy (n = 37) vs. the spleen-preserving group (n = 289), respectively [3]. In their multivariate analysis, splenectomy was found to be an independent factor for a shorter survival. Interestingly, the survival benefit was independent of the performed operation [3]. In our data, the survival benefit of patients without splenectomy was prominent in the total pancreatectomy group, while we did observe little to no effect in the distal pancreatectomy group. The same observation was reported in a Dutch outcome analysis of patients with pancreatic cancer who underwent distal pancreatectomy. In line with our data, splenectomy did not show a significant association with patient survival in this subgroup [19]. However, the proportion of spleen-preserving compared to spleen-resecting surgery in this study was rather small (17 vs. 124) and the study may therefore lack the statistical power to detect survival differences [19]. In contrast to our data, the retrospective analysis of Yang et al. did not detect a difference in long-term survival of pancreatic cancer patients undergoing total pancreatectomy between the spleen preservation (Warshaw technique) and splenectomy group (n = 38 vs. 21, p = 0.905) [4]. We analyzed the above-mentioned studies from Schwarz et al. [3] and Yang et al. [4] in a meta-analysis (Rooij et al. [19] did not include p values). Here, splenectomy was identified as an independent risk factor for an inferior long-term survival. However, our study is certainly limited by its retrospective nature. It is crucial to acknowledge that a significant constraint of this study is the use of overall patient survival data. While overall survival and progression-free survival are closely correlated for pancreatic cancer patients, given the unfavorable prognosis and high recurrence rate, this introduces another potential source of bias that limits the generalisability of our conclusions. Additionally, information on tumor location and indication for total pancreatectomy (tumor location, size, high-risk pancreaticojejunostomy, or no residual functioning pancreas), indication for the chosen technique (spleen preservation/resection), and perioperative treatment regime (neoadjuvant/adjuvant treatment) was not included in the StuDoQ|Pancreas registry. Another data that was not sufficiently reported in the database was the information on pre- and postoperative oncologic treatment. This remains a major limitation of the study, as this is of crucial importance to the tumor recurrence and with that to overall survival. Due to the limitations mentioned above, we cannot make a general recommendation for spleen preservation in ductal pancreatic cancer. Prospective, randomized trials with recurrence-free survival data are needed to provide clear guidelines.
Our systematic review shows that the impact of spleen removal on pancreatic cancer outcomes is poorly studied and the underlying mechanisms remain unknown. In the human organism, hematologic changes can be observed after splenectomy [20]. However, it is not known how this affects the course of malignant disease, such as pancreatic cancer. One pioneering study by Hwang et al. observed a significant increase in tumor growth after removal of the spleen in their murine pancreatic cancer model [11]. In the splenectomy group, they additionally observed a lower ratio of effector T cells (CD8 + /CD4 +) to immunosuppressive regulatory T cells (FOXP3 +), suggesting an impaired anti-tumor immune response [11]. It may be that this impaired immune system leads to a less effective anti-tumor immune response, especially when severe diabetes co-exists e.g. after total pancreatectomy [21]. However, further evidence is needed to understand and potentially circumvent these changes induced by splenectomy.








留言 (0)