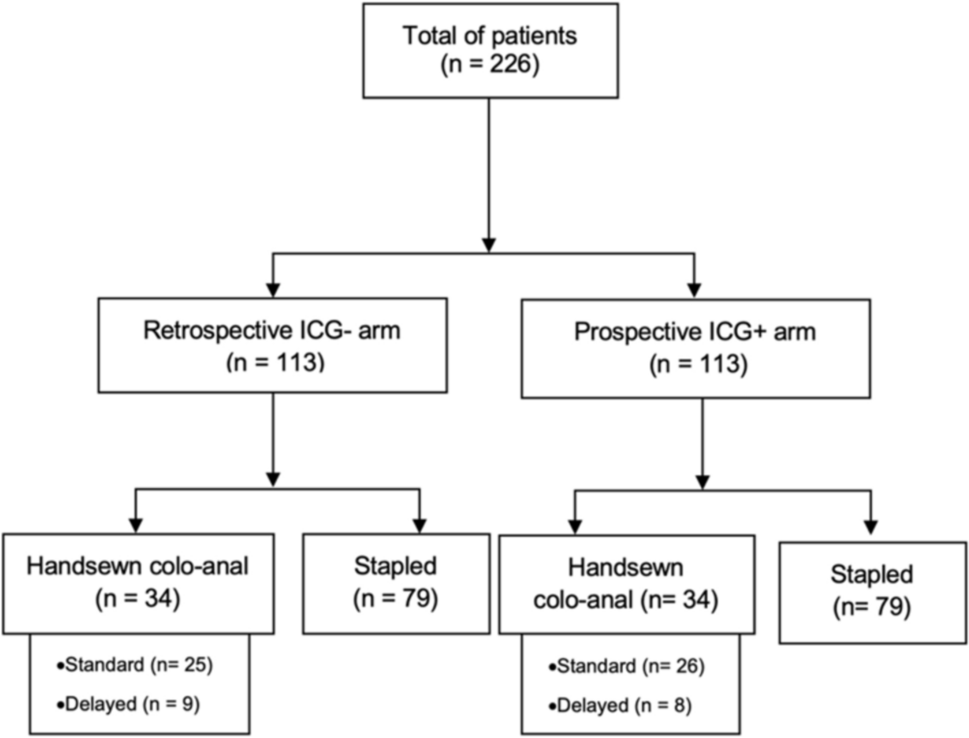
From June 2011 to March 2016, all patients who required TME and manual CAA were considered to have undergone TaTME/CAA and were included in this open, single-arm prospective study. These patients were the first to undergo this new approach for low-lying rectal cancer treatment. This study was approved by the local institutional review board. All patients received information on the expected benefits and potential risks of the procedure before providing their consent. The study was conducted in accordance with the 1989 World Medical Association Declaration of Helsinki.
Two colorectal surgeons (B.L. and C.D.C.) with extensive laparoscopic colorectal experience (> 200 LTMEs each) performed all study procedures. The procedures were performed by one or both the surgeons, depending on their experience and operational conditions. The distribution of procedures between the two operators was balanced in terms of volume and time. Therefore, we consider this experience comparable to a single-surgeon learning study.
Oncological management
Pretherapeutic evaluations included a digital rectal examination, pelvic magnetic resonance imaging (MRI), endoscopic ultrasound and thoraco-abdominal and pelvic computed tomography (CT) scans. In our department, preoperative chemoradiation (CRT) is indicated for T3 and/or N+ mid and low rectal adenocarcinoma and for T2 low-lying tumours close to the sphincter. Long-course CRT consisted of a total dose of 50 Gy, with a daily dose of 2 Gy combined with capecitabine. Induction chemotherapy (FolFirinOx, 4–6 cycles) before CRT is offered to patients with a threatened circumferential resection margin (CRM) on MRI. Surgery was usually performed 8–12 weeks after the completion of CRT.
Patient selection for TaTME/CAA
All patients with low rectal adenocarcinoma who required conservative TME and CAA were included in the study. The exclusion criteria were T4 fixed tumours requiring multivisceral resection and/or abdominoperineal excision, possible mechanical trans-sutural anastomosis, unresectable metastatic disease, and/or peritoneal carcinomatosis.
Technical considerations and operative strategy
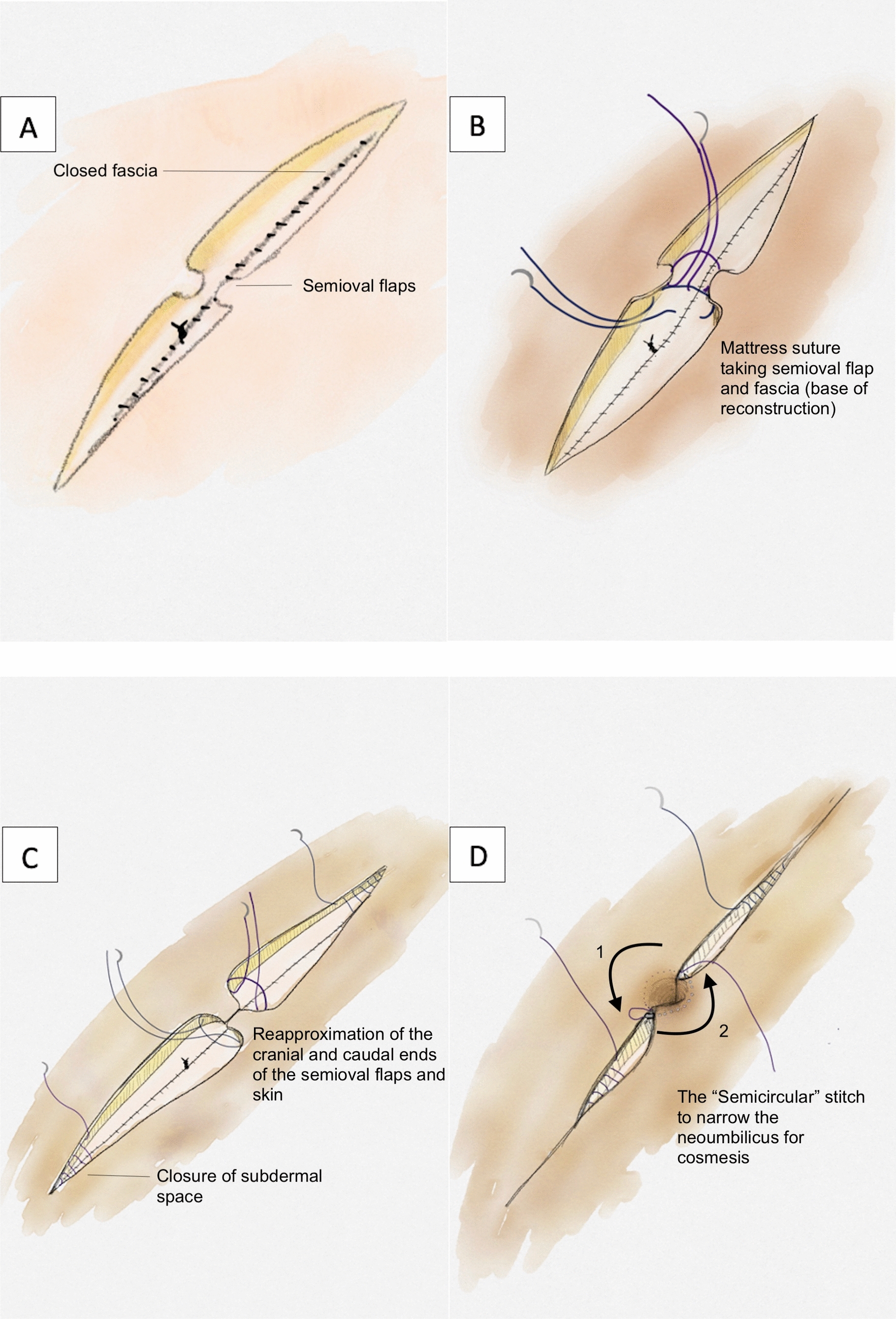
The operative technique was standardised for all patients, as previously described [28]. A primary conventional transanal approach was performed with standardised steps for dissection including a mucosal incision and internal sphincter dissection, based on tumour extension [29]. After circumferential exposure of the fascia recti, the distal rectal lumen was closed using a 3/0 manual purse-string suture. The surgical field was systematically rinsed with isotonic saline solution. The transanal endoscopic device (Gelpoint Path by Applied Medical, Rancho Santa Margarita, CA, USA, or SILS port by Covidien, Norwalk, CT, USA) was then positioned to perform the entire mesorectal excision. TaTME was considered complete if the posterior dissection led to the vertical part of the rectum, the Douglas pouch was opened, and the lateral nervous plexuses were identified. Laparoscopic abdominal approach was secondary performed for colonic mobilisation with systematic splenic flexure mobilisation and inferior mesenteric vessel ligation. No simultaneous double-team approach was used in this study. The specimens were extracted transanally or abdominally. Manual CAA was then performed. Loop ileostomy was systematically performed, and most patients received a pelvic drainage tube.
For high-risk patients and fragile patients, the ‘ultralow Hartmann procedure’ was performed as a planned procedure. The same dissection steps were followed with comparable oncological principles, although anastomosis was not performed, and a permanent terminal left colostomy was established.
Study settings and data collection
The patients’ demographics, perioperative details, histological parameters, and follow-up data were collected prospectively. The duration of the transanal approach was defined as the time interval from the mucosal incision until the completion of TaTME. The total operation time (TOT) was defined as the interval between mucosal incision, wound closure, and stoma completion. We prospectively evaluated the 30- and 90-day postoperative morbidity according to the Clavien–Dindo classification [30]. Conversion was defined as any incision for any reason other than specimen extraction.
Objectives of the study
We hypothesised that the most relevant variables related to the learning process would be operative time, procedure completion rate, conversion rate, postoperative morbidity, macroscopic mesorectal assessment, and microscopic margins. We aimed to provide an all-encompassing view of the learning process for TaTME by combining the expected parameters of the learning process into a composite success criterion and generating a curve that outlines the changes in the success rate. Success was recorded if the following five items were present: TaTME procedure completed (as previously defined), no conversion to an open procedure, no severe (i.e. Clavien–Dindo III–IV) postoperative morbidity, grade III complete mesorectal excision, and R0 resection (CRM > 1 mm and a safe distal margin). The second important goal was to identify the key parameters that have a significant impact on the learning process and to determine where the focus should be placed in the future for effective training.
Statistical analyses
All statistical analyses were performed with the significance level set at α = 0.05, using SAS 9.3 (SAS Institute Inc., Cary, NC, USA).
For the operative time, we used the 30-patient simple moving average method. If x denotes the operation, the 30-patient simple moving average (SMA30) is defined as the mean of the previous 30 points as follows:
$$}_\left(n\right)=\frac_+_+\dots +_}.$$
For the binary variables (i.e. procedure completion rate, conversion rate, postoperative morbidity, macroscopic mesorectal assessment, and microscopic margins), we used the risk-adjusted cumulative sum (CUSUM) plot:
$$\text\left(n\right) = \sum_^ = \left(_-\tau \right)+^_}_$$
where xi = 1 indicates success, xi = 0 indicates otherwise, \(\tau\) represents the observed event rate, and pi is the expected rate of success in each case, which was calculated from a logistic regression model that included success as an event of interest, and sex, pretherapeutic T stage (0–2, versus 3), and the N stage as the independent variables [31, 32]. Every included case was plotted from left to right on the horizontal axis. As described by Tekkis et al. [33], this plot considers an individual’s expected probability of success and does not affect the surgeon’s performance in the case of success for a high-risk patient. We defined the end of the learning process as the point at which the curve reached a steady state (cut-off point).
The ‘learning’ and ‘experience’ periods were, therefore, defined by the periods before and after the cut-off point respectively. Comparisons between the two periods were made using the chi2 or Fisher’s exact test for qualitative variables and the Wilcoxon–Mann–Whitney U test for quantitative variables. Follow-up data from the date of surgery in the learning and experience periods were estimated using the inverse Kaplan–Meier method and compared using the bilateral log-rank test.






留言 (0)