
記住我
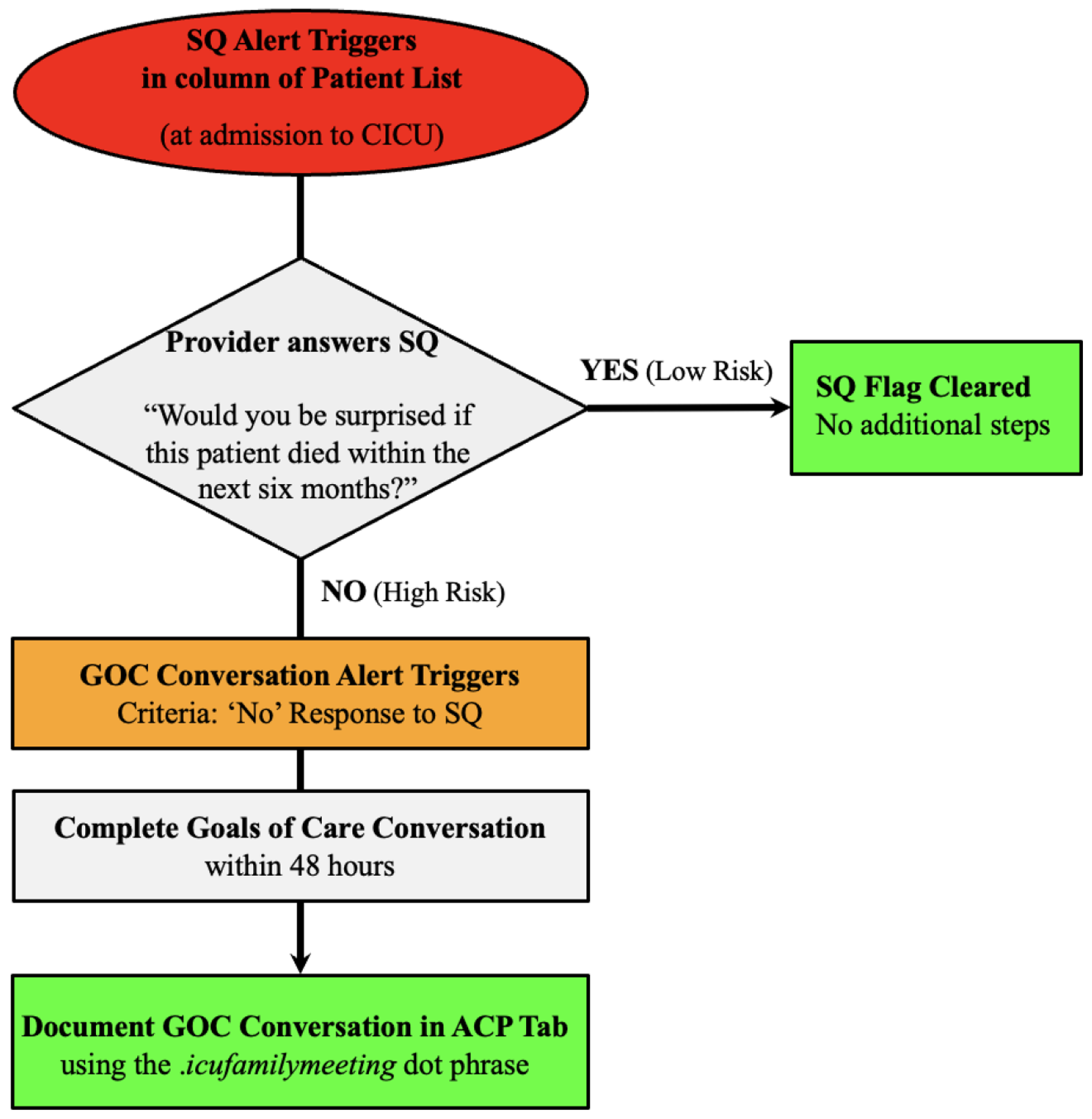




Participants in most cases often emphasised that decision-making regarding palliative sedation did not occur as a single event, but was a dynamic and iterative process occurring over time. In most cases, once the idea of palliative sedation had been introduced, there was an ongoing process of information-sharing, observation, and deliberation between patients, relatives, and healthcare providers until a decision was made. This process generally followed a sequence of starting the conversation, a conditional decision (where prior decisions were made to be enacted in specific circumstances), followed by a final decision to proceed with palliative sedation (see Fig. 3).
Fig. 3
Iterative process of decision-making in palliative sedation
How the conversation startedSeveral bereaved relatives reported that the idea of palliative sedation was initiated a while before the phase of dying (in one case a year before death). The concept of sedation was often introduced in a broader conversation about end-of-life care triggered by previous experiences or during a hospital admission during the illness trajectory. In these cases, patients and families had detailed knowledge of their condition and prognosis and a clear view of how they would like to proceed including prior consideration of palliative sedation.
“I think two years ago, mum and dad went together to the palliative physician. Mum had
everything written on paper, her Do-Not-Resuscitate -code ... she had everything on paper and afterwards she also let us know …”(Belgium, case 2, relative)
According to the bereaved relatives, while some patients and families had an understanding of their health condition and prognosis, they were unaware of what could be offered as palliative care options. In a few cases, it appeared that patients and families came to palliative care services without adequate awareness of their prognosis, with some even hoping for further cancer treatment and cure.
“There are people who say: "well, this is it, this is the end, this is the end here and now", but he was always thinking that he was going to get better, and it was Easter, and he was Catholic, and then he would look at me and say: "I'm waiting for my miracle", and the next day he would say to me: "I'm still waiting for my miracle": "I'm still waiting for my miracle". (Spain, case 30, relative)
Between the settings, there were different approaches to providing information to the patient. So, while in the Netherlands settings, palliative sedation was addressed proactively, in other settings, palliative sedation was mostly discussed reactively after it was initiated by the patient (eg. Site 1). Some healthcare professionals explicitly avoided reference to “palliative sedation”, but used terms such as ‘comfort’ or ‘relief’ (eg. Site 7), while in the Netherlands, Belgium and Germany palliative sedation is explicitly named in conversations with patients and families.
“There were conversations about there being no more treatments, and indeed, we talked to him about there being nothing more to do, that we needed to focus on comfort” (Spain, case 31, health care professional)
Both bereaved relatives and healthcare professionals reported that in end-of-life conversations, pros and cons of palliative sedation, and the concerns of patient and relatives were discussed. Several healthcare professionals suggested that information frequently needed to be repeated in subsequent meetings since not all information was understood initially, because of the emotional distress of patients and families.
"The options have been repeatedly explained, not once but a whole number of times. I thought at least twice by myself and questioned again to the patient. It has been proven that in emotional conversations, we only remember a small percentage of the information. So, the repetitiveness is very important for clarity." (Belgium, case 1, healthcare professional)
Conditional decisionAccording to bereaved relatives, a few patients were initially reluctant to discuss end-of-life care, although most patients and families were open to address this topic. Bereaved relatives and healthcare professionals reported that the expected worsening of the patient’s medical condition with more suffering was often a concern. Anticipating this, many patients formulated a conditional decision, that if the situation worsened, then they wanted to be sedated. This ‘conditional decision’ was in many cases a strong directive on how to proceed. In most of these cases, relatives supported patients’ decisions about palliative sedation.
“It was discussed in advance that she would like this [palliative sedation] in case her suffering would become intolerable, and she was probably very, very restless throughout the weekend, always trying to get up and then it was discussed with her that palliative sedation could be started now and she agreed to this.” (Germany, case 11, healthcare professional)
Decision to start sedationData suggests that following initial conversations and conditional decision-making, the final decision to proceed with palliative sedation can be complex, and emotionally difficult for patients and families. This final decision was often precipitated by a deterioration in the patient’s condition, and the presence of refractory suffering, prompting further discussions about commencing palliative sedation. In some cases, this was initiated by the healthcare team, after a period of observing the patient’s symptoms and team discussions. In other cases, it was initiated by a verbal request or non-verbal communication from the patient. Our findings suggest that whilst families tended to be influenced mainly by observing patients’ physical symptoms, healthcare professionals were more likely to also consider psychological and existential suffering as indications for palliative sedation.
“When she started to have these fears for her end of life, we started talking about sedation, how to modulate sedation, so we shared the process with her. At a certain point, when she couldn't take it anymore, we started discussing it during the visit and said to each other: let's start the sedation because perhaps the time has come to control things better.” (Italy, case 13, healthcare professional)
A final decision about palliative sedation usually involved further discussions between all parties, often referring to previous conversations. When the patient was no longer able to communicate, any earlier conditional decision was a valuable directive, along with consultation with the relatives. However, making the final decision to start palliative sedation was often very difficult and emotionally distressing for patients and families, even when patients were initially committed to it. In a few cases, ambivalence was reported when patients and families struggled between reducing suffering and saying their final goodbyes. When tensions increased during this period, the healthcare professionals reported that they mediated to reach a consensus.
“He was suffering from these five things, and he indicated that it was enough, and he pointed to his mouth again, meaning I want a sip, I’m thirsty. At that time, I started the conversation with his daughters like, I think we need to start palliative sedation now because this is unbearable for him. And his daughters really struggled with that. We had this conversation on Monday, and they had to sleep on it for a night, so Tuesday we had the conversation again, now with all daughters present. A long conversation, even though you would think, this is clear as day, that man is suffering terribly, and he doesn’t have much longer to live. Then we talked for about an hour and at some point one of the daughters said: maybe giving him palliative sedation is the merciful thing to do. Yes, I confirmed that obviously, and then they were all aboard like, okay this is our decision. That evening, half past seven we started sedating.” (Netherlands, case 20, healthcare professional)
When light or intermittent sedation was insufficient, additional decision-making was precipitated. Patients who were still conscious were involved, otherwise, physicians took the lead after informing or consulting with relatives.
留言 (0)