We found robotic dual-docking surgery performed with the ports placed laterally aligned at the level of the umbilicus to be applicable to endometrial cancer. Using our standard protocol, we achieved almost complete surgical staging without the need for additional port placement. The number of lymph nodes, including para-aortic lymphadenectomy up to the left renal vein level removed by our system, was the 2nd highest among other studies [6, 7, 11,12,13,14,15,16, 19,20,21], ranging between 19 and 52, and only one patient experienced a recurrence of the disease, with no deaths being reported during the long-term follow-up periods. The relatively long console time in our cohort may be attributed to extensive lymph node dissection.
Initial reports regarding robotic surgery for para-aortic lymphadenectomy in endometrial cancer were published in 2008 [5,6,7]. A literature review, including a feasibility assessment via the intraperitoneal approach is shown in Table 4. Evidence from Asia, especially Japan, has not yet been reported; however, our analysis, following an adequate period of observation, suggests that that this procedure be adopted as a surgical standard.
Table 4 The literatures of the transperitoneal para-aortic lymphadenectomy mainly involving intermediate to high-risk endometrial cancerPara-aortic lymphadenectomy as a dual-docking surgery was conducted by Magrina et al. [12] in 2010, but these procedures were not completely dual-docked robotic systems because of the need to turn the patient’s bed and the requirement for additional port placement. Meanwhile, Zanagnolo et al. [13] report a small alteration to their robotic surgery using the Da Vinci S or Si system, while Pakish et al. [22] describe the utility of a retroperitoneal approach, in which more para-aortic lymph nodes could be resected than during a transperitoneal approach (the median number of lymph nodes: 10 in retroperitoneal approach vs. 4 in transperitoneal approach). However, the range of arm motion of transperitoneal approach is limited, and unlike laparoscopic surgery, robotic surgery requires repositioning or changing the patient’s cart position. Therefore, we consider that dual-docking surgery is more realistic. The usefulness of double-docking compared with single-docking is described by Franke et al. [14]. In double docking for para-aortic resection, one endoscope port and three other ports are located in the lower abdomen under the Da Vinci Si system docked on the patient’s head. In pelvic lymphadenectomy following para-aortic lymphadenectomy, the system was undocked, the patient’s cart was moved between the two legs, and the endoscope port was placed on the umbilicus. Although the double-docking technique leads to approximately twice the number of resected lymph nodes compared to single-docking, the surgical time is quite long, and docking is complex.
We introduced the lateral alignment of the ports, and a similar retrospective study of port placement was conducted by Ekdahl et al. [16]. The endoscope port in double-docking surgery using the Da Vinci Si system was introduced laterally at the level of the iliac spine, which was almost 3 cm caudal to the umbilicus. After the upper abdominal procedures on the patient’s right side above the robotic column, the column was rotated, and the patient’s bed was moved appropriately for the lower abdominal procedures. Similarly, Loaec et al. [15] report the use of an endoscope port placed at the median suprapubic and umbilicus for para-aortic lymphadenectomy in pelvic lymphadenectomy.
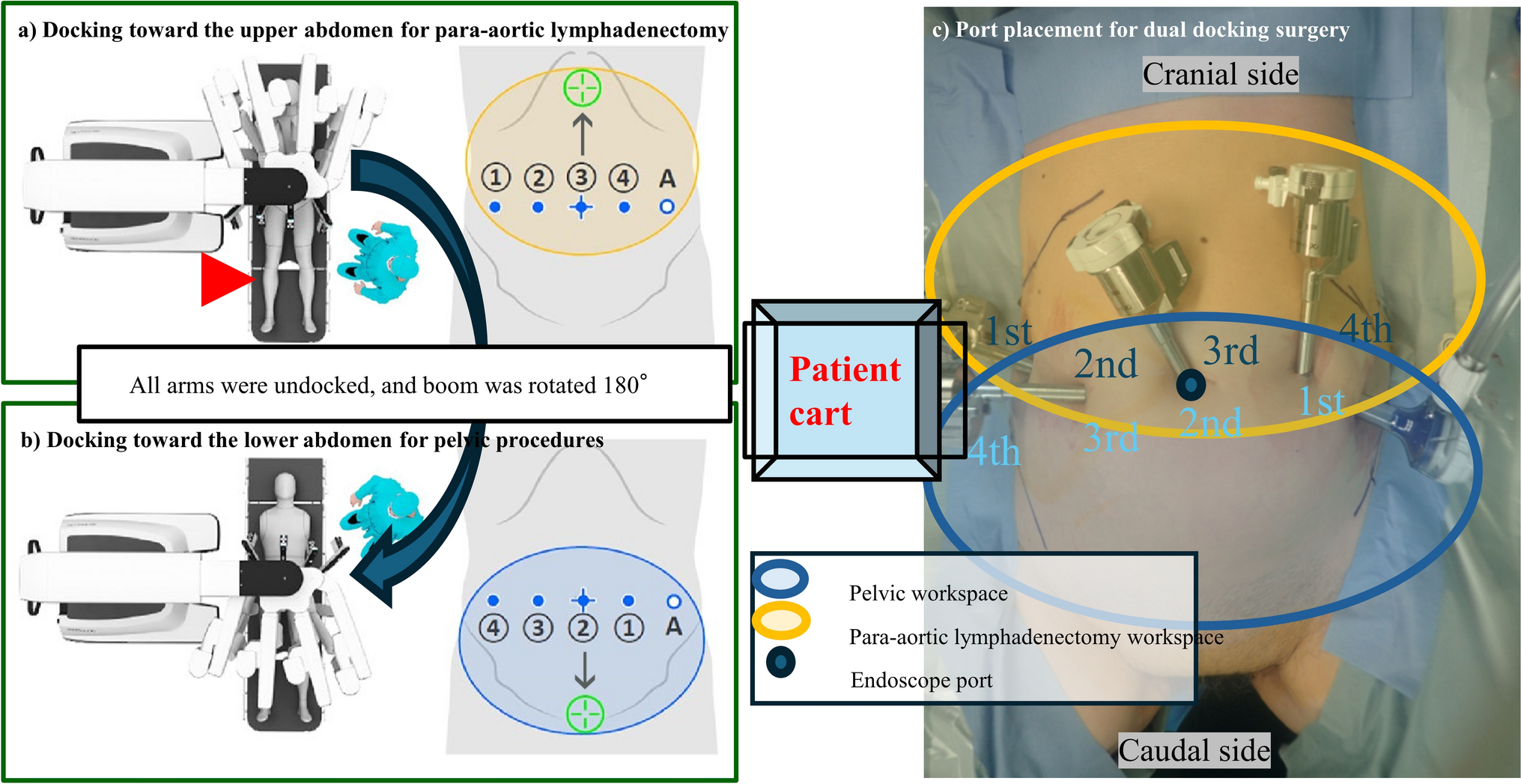
Using the latest Da Vinci Xi system, we have developed some newer improvements including: (1) docking from any direction by turning the boom, (2) the endoscope port can be attached to any arm since it has been miniaturized to 8 mm in diameter, and (3) the patient clearance function and enlargement of the range of motion and distance by the end-list forceps which are 4.5 cm longer than Si, made it possible to laterally align four Da Vinci 8 mm ports during dual-docking surgery. These improvements have led to the ease of dual-docking, and in most situations when using the Da Vinci Xi system, the patient cart or bed does not need to be moved.
A recent retrospective report by Lee et al. [20] compares the Da Vinci S system and laparoscopic surgery with a robotic endoscope port fixed at the umbilicus regardless of the patient’s habitus, with the other ports aligned at the level of the umbilicus. Previous studies have been conducted based on earlier robotic systems, and there is a lack of evidence including prognostic outcomes for prospectively evaluating dual-docking surgeries using the Da Vinci Xi system.
The advantages of robotic surgery for laparotomy or laparoscopy in obese patients with endometrial cancer have been described [7, 11, 23, 24]. Laparoscopic surgery in obese patients results in fewer postoperative complications, shorter hospitalization, and lower levels of postoperative pain than laparotomy [7, 23]. Compared to less invasive surgical approaches, a robotic surgery patient group that had a significantly higher BMI showed superior surgical outcomes over a laparoscopy group who underwent comprehensive surgical staging [11]. Regarding the degree of obesity in patients undergoing robotic surgery, BMI classification did not correlate with conversion to laparotomy or complication rate, and node dissections were equivalent in the three categories [24].
The novelty of our dual-docking surgery is that it provides a suitable port placement arrangement. Changing the surgical range from the upper abdomen to the lower abdomen can be simply performed by rotating the boom without moving the patient cart and by directly docking the ports in the Da Vinci Xi system. No complications due to the most frequently used Endowrist® Vessel Sealer were found in retroperitoneal lymphadenectomy or in the difficulty of robotic operation. However, 4 out of 15 patients (26.7%) experienced major complications. The injury to the right common iliac vein in Case 11 was not attributable to a technical error but rather occurred during rapid forceps manipulation. No further injuries were observed after this case because the standard technique for para-aortic lymph node dissection described in “Materials and methods” was fully established and carefully performed. The reason for the right renal artery injury in Case 14 may have been that the camera could easily reach the deep field under the renal vein and provide a view different from that of laparotomy. Although these complications are specific to endoscopic surgery, they are not technical problems that occurred in only a single case; therefore, they do not account for the complexity of this technique.
Robotic endometrial cancer surgery in lean Asian patients has not yet been described, and our cohort is the leanest recorded in the literature (Table 4) [5,6,7, 12,13,14,15,16, 19,20,21]. We verified that for certain body habitus types, the positioning of ports allowed for successful surgery without interfering with the movement of intraoperative forceps. Three patients with a BMI greater than 30 underwent surgery successfully without experiencing serious perioperative complications. In addition, a BMI of less than 20 allowed for the placement of a laterally aligned port that accommodated robotic forceps. The analyzed surgical outcomes of the literatures and our study are shown in S3. The number of lymph nodes for para-aortic lymph node dissection was positively correlated with operative time and conversion rates, with a higher number of lymph nodes removed in our facility and longer operative time. Contrary to expectations, the number of para-aortic lymph node dissection decreased as BMI increased, with our cohort being the leanest and most adequately dissected. In the learning curve of our facility, as the number of experienced cases increased, operating time tended to decrease. Our study was limited by the small number of patients and the inclusion of a large range of body types. Although the surgeon performing all procedures was experienced, the median surgical time, especially for para-aortic lymphadenectomy, was longer than that reported elsewhere. Approximately 20 procedures are needed for a surgeon to become proficient in performing retroperitoneal lymphadenectomy for endometrial cancer [5]. Most of our cases were successful, but we also experienced three cases with serious complications in dual-docking surgery, indicating that the results of our study require further research.
In conclusion, this technique allowed enough lymph nodes to be dissected in patients of various types of habitus including lean common among the Japanese, and the prognosis was excellent. This study demonstrated that dual-docking surgery, facilitated by the introduction of the Da Vinci Xi system, has the potential to become a standard procedure for robotic endometrial cancer surgery. Further extensive clinical trials on the feasibility of dual-docking surgery are needed.







留言 (0)