We evaluated the frequency of PCS-related symptoms in children and adolescents after SARS-CoV-2 infection in the Omicron era compared with SARS-CoV-2-seronegative controls. Despite the increase in SARS-CoV-2 infections during the Omicron wave, the number of children with ≥ 1 typical PCS symptom(s) was similar in both groups, as was the frequency of the symptoms reported individually. However, impaired concentration and reduced physical performance were significantly more common among children with Omicron infection. Children in the COVID-19 group rated their fitness as worse, with otherwise equal ratingsSSS of QoL regarding general and mental health.
According to a recently published study comparing typical PCS symptoms in children across different pandemic waves [17], the relative number of children and adolescents with PCS-like symptoms (64.9%) in our COVID-19-cohort was of the same magnitude as in COVID-negative controls (62.1%) during the Omicron wave. In contrast, in our cohort, the proportion of children reporting typical PCS symptoms following SARS-CoV-2 infection was similar to that reported during the SARS-CoV-2 Alpha wave. Conducted in the UK, the Children and Young People with Long COVID (CLoCk) study reported 66.5% of 3065 adolescents with persistent symptoms 3 months after SARS-CoV-2 infection compared with 53.3% of healthy controls [2]. In a large Danish cohort study, Borch et al. [28] reported a prevalence of up to 51% in children and adolescents versus up to 38% in controls > 4 weeks after SARS-CoV-2 infection.
Consistent with other studies, we found a high burden of symptoms in both patients and controls, pointing toward factors other than infection contributing to PCS-like symptoms. Therefore, we suspect that pandemic-related interventions will have a major impact on children’s physical and mental health. This assumption is supported by the measurable decline in the physical and mental health and QoL of children and adolescents [29,30,31,32]. Contributing factors may include school closures and related restrictions on the lives of children and young individuals. Despite a slight improvement, the rate of reported health problems remained above pre-pandemic levels [29, 33, 34].
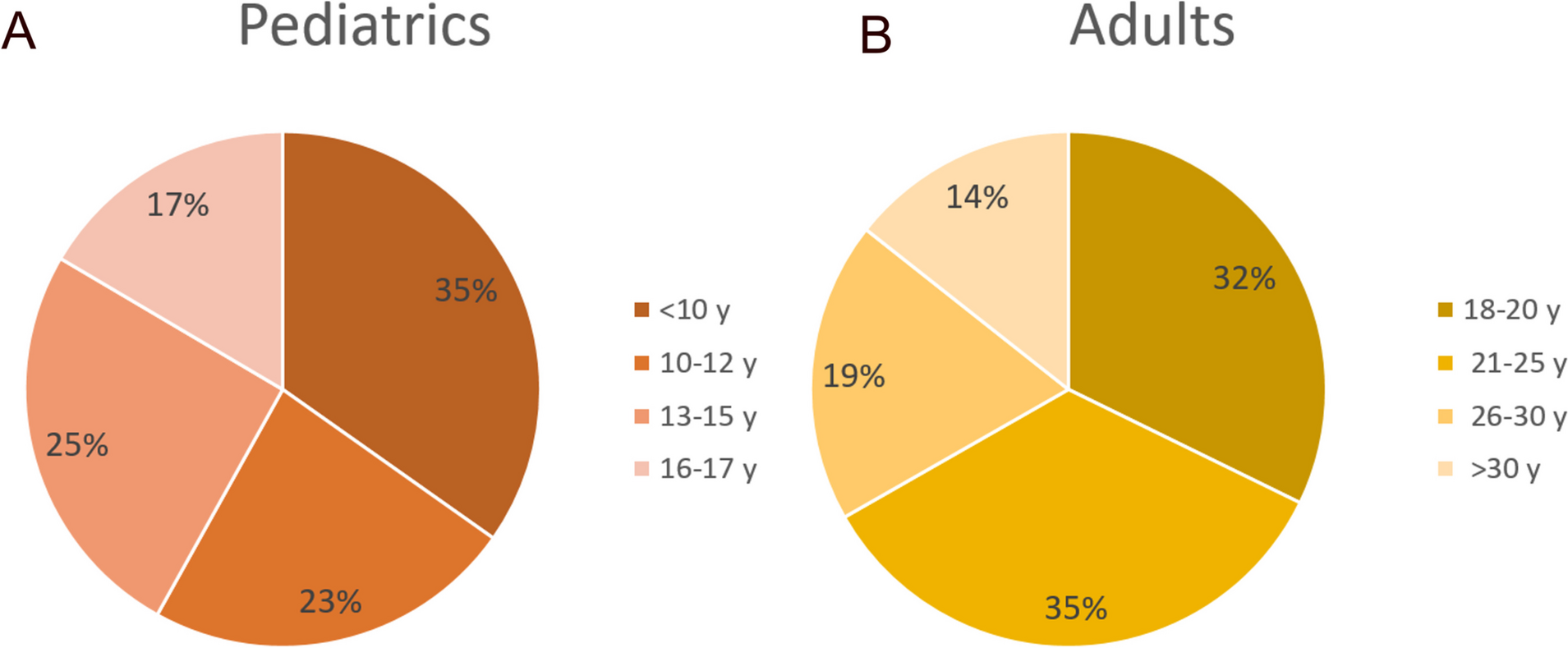
Another explanation for the higher burden of complaints in the control group may be the slightly higher proportion of adolescents in our control group compared with the COVID-19 group (66.7% vs. 49.1%, respectively). Data regarding high prevalence of symptoms, which were also grouped as “PCS-like”, already existed in this age group before the pandemic. For example, > 20–30% of adolescents experience fatigue [35, 36]. In a representative German study (KIGGS cohort) in 2019, 45.2% of 11–17-year-old girls reported recurrent headaches, recurrent abdominal pain (34.5%), and recurrent back pain (28.3%) [37]. This high burden of symptoms among adolescents independent of COVID-19 was also observed in our study cohort. For example, two-thirds of the participants in the control group who reported reduced physical performance were > 12 years of age (Fig. 3). Regarding the sex association, our study revealed a trend, rather than a confirmed higher symptom burden after COVID-19, among girls and adolescents [2, 5]. Unfortunately, the literature lacks pre-pandemic prevalence data for all PCS symptoms with which to compare our cohort. Our findings highlight the need for more robust longitudinal research to track symptom prevalence in the future.
Despite the high frequency and burden of reported typical PCS symptoms in the COVID-19 and control groups, children and adolescents rated their QoL and general and mental health mostly as excellent or very good. We found no significant differences between the two groups, which is consistent with findings from other larger cohorts [2, 7]. Thus, the decline in QoL observed in children and adolescents during the pandemic [29, 30] appears to be independent of SARS-CoV-2 infection. However, children and adolescents rated their fitness as worse if they experienced SARS-CoV-2 infection than the control group.
Compared with the initial years of the pandemic, the incidence of PCS decreased significantly in the Omicron era [14, 15, 17]. However, following infection with the Omicron variant, PCS-associated symptoms, such as fatigue and dermatological, gastrointestinal, sleep, and sensory manifestations, have also been described in children and adolescents [15,16,17]. However, in accordance with the study by Pazukhina et al. [17], our analysis of a non-selected cohort compared with a control group did not confirm that many of these symptoms were purely SARS-CoV-2 related, although we also observed significantly impaired physical performance in the COVID-19 group. Of note, olfactory and gustatory disturbances were rarely reported in our cohort, which is still one of the most common symptoms reported in the Alpha wave [28] and is listed as a major symptom according to the WHO definition [3].
Limitations and strengths
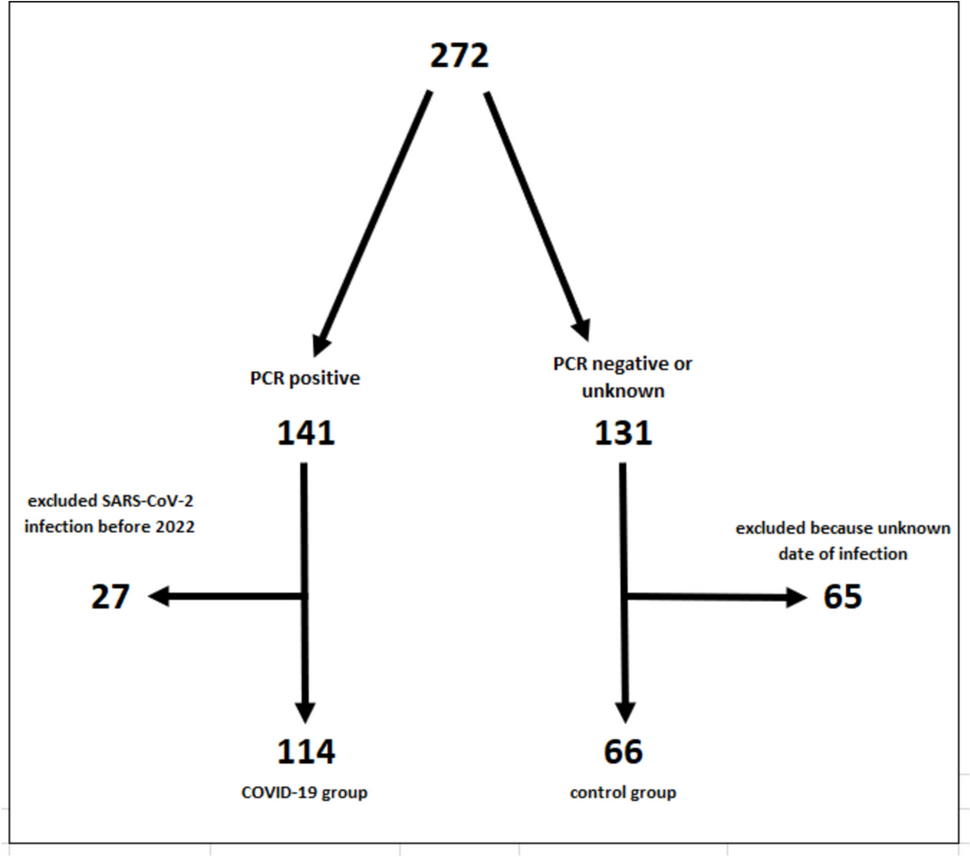
Limitations of our study include its retrospective design and relatively small sample size. Unfortunately, the time interval between infection and study enrolment was not recorded for all participants. In the majority of the children in Bochum, the infection had occurred more than 6 months previously. Because of the uncertainty in the other participants, we avoided using the term confirmed PCS and only analysed the frequency of PCS-associated symptoms. The study relied on self- or parent-reported symptoms in the absence of clinical assessment. Parents answering questions on behalf of their children can lead to higher or lower levels of complaints, and knowledge of Sars-CoV-2 infection could have led to false-positive results. Although we recruited from a non-selective cohort, we cannot exclude the possibility that families who were very sensitive to PCS-associated symptoms enrolled in the study. This could be another explanation for the high symptom rates in the COVID-19 and control groups.
Strengths of our study included the analysis of a non-selective cohort of children and adolescents after SARS-CoV-2 infection compared with a control group, and the strict inclusion criteria of PCR-confirmed SARS-CoV-2 infection and antibody analysis, which are among the main points of criticism in other PCS studies [18].

留言 (0)