
記住我

Although small-cell lung carcinoma (SCLC) molecular subtype classification was observed in human tumours and preclinical models, it requires further validation in a large cohort of SCLC patients at various disease stages and variable specimens to highlight its clinical significance.
WHAT THIS STUDY ADDSOur results validated the feasibility of lung biopsy samples for identifying SCLC molecular subtypes, and revealed that combined SCLCs were significantly enriched in the subtype of POU2F3-dominant SCLC (SCLC-P) and for the non-SCLC components of combined SCLCs, adenocarcinoma was more prevalent in ASCL1-dominant SCLC, while large-cell neuroendocrine carcinoma was more commonly seen in SCLC-P.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICYThis study describes the diagnosis, prognosis and predictive significance of SCLC molecular subtype classifications, which would aid in the development of personalised treatments and subtype-specific treatment of SCLC.
IntroductionSmall-cell lung carcinoma (SCLC) accounts for approximately 15% of newly diagnosed lung cancers.1 Current therapeutic approaches for SCLC are generally based on disease stage, with no consideration of distinct biomarkers that might have predictive or prognostic significance. Recently, SCLC profiling studies have suggested molecular subtypes defined by the relative expression profiles of four key transcriptional regulators: achaete-scute family Basic Helix-Loop-Helix (BHLH) transcription factor 1 (ASCL1; SCLC-A), neuronal differentiation 1 (NEUROD; SCLC-N), POU class 2 homeobox 3 (POU2F3; SCLC-P) and Yes1-associated transcriptional regulator (YAP; SCLC-Y).2 These four subtypes are associated with neuroendocrine (NE) differentiation, showing that the first two groups have significant NE differentiation, namely, the NE phenotype, and the latter are non-NE phenotypes.2 This molecular subtyping concept has inspired many researchers to stratify patients into subsets with distinct therapeutic vulnerabilities.3–5 Notably, delta-like ligand 3 (DLL3), an inhibitory NOTCH ligand upregulated in ASCL1-dominant SCLC, is overexpressed in 80% of SCLC tumours but is not expressed in normal tissues.6 7 It is currently under investigation as a potential therapeutic target.8 The NEUROD1 and POU2F3 subtypes are characterised by MYC gene overexpression,4 which is also a novel therapeutic target under clinical trial.8
Despite a substantial volume of data on SCLC molecular subtypes in preclinical models, there is currently minimal information on the expression of a full panel of these markers in SCLC clinical samples.9–18 Some of these studies lack information on previous treatments and outcomes.9–11 17 Additionally, most specimens were biopsies/tumour microarrays (TMAs) or surgically resected SCLC samples from limited stage patients.9–18 However, emerging evidence suggests that different subtypes are dynamically changing, emphasising the intratumoral heterogeneity and strong plasticity of SCLC.19 20 Thus, biopsies/TMAs may not represent the molecular subtype of the whole tumour, and surgically resected tumours might not completely mirror the clinicopathological characteristics of the entire disease spectrum.
Therefore, we collected specimens from SCLC patient with various stages and investigated the expression of molecular subtypes and predictive markers by immunohistochemistry (IHC) in whole SCLC tissue/cell blocks of formalin-fixed paraffin-embedded (FFPE), to explore the clinicopathological features and prognostic implications of SCLC molecular subtype. To the best of our knowledge, this is the first study to investigate the expression of subtype markers in paired resected-biopsy SCLC specimens.
Materials and methodsPatient selection and data collectionThis retrospective study was performed using archived samples from the Peking University Cancer Hospital database between January 2010 and April 2023. We collected surgically resected SCLC primary tumours, resected biopsy of SCLC metastases and pleural effusions diagnosed as SCLC by cytology. In addition, treatment-naive patients with paired lung core-needle biopsies of surgically resected SCLC were included. Patients with unavailable FFPE and poor specimen quality from IHC analysis were excluded. The approval of the Ethics Committee of Beijing Cancer Hospital (2023KT23) was obtained and waived the need for individual informed consent for this study.
All archival slides stained with H&E and conventional NE diagnostic markers, CD56, chromogranin A (CgA), and synaptophysin (Syn) were retrieved and re-evaluated by two senior pathologists (YZ and HW) independently to confirm the diagnosis of SCLC. tumor-node-metastasis (TNM) stage was determined according to the eighth edition of the TNM classification system proposed by the American Joint Committee on Cancer. Detailed patient demographic and clinical information were collected from the electronic medical records. Follow-up data were obtained from the clinical records and telephone interviews. Overall survival (OS) was calculated as the date from pathological diagnosis to the time of death from any cause. Progression-free survival (PFS) was calculated from the date of pathological diagnosis to the time of the last clinical evidence of recurrence, progression, or death.
IHC staining and scoring criteriaFFPE specimens were prepared, and consecutive 4 µm-thick tissue sections were cut from the specimens for IHC analysis. All samples were stained for the six markers (ASCL1, NEUROD1, POU2F3, YAP1, DLL3 and MYC). Detailed IHC protocols are summarised in online supplemental table S1.
We evaluated the entire tumour area for all specimens, and the expression of markers was recorded by a histoscore (H-score), which was derived by multiplying the percentage positivity by the intensity score (1, 2 and 3), yielding a range of possible H-scores of 0–300.21 The WHO classification of lung tumours defines combined SCLC as tumours containing both SCLC components plus any type of non-SCLC (NSCLC) component, including adenocarcinoma (ADC), squamous cell carcinoma (SCC), large-cell neuroendocrine carcinoma (LCNEC), large-cell carcinoma or rarely other,22 and in combined SCLCs, we selected FFPE blocks in which at least half of the tumours were SCLC component, and IHC scores reflect expression exclusively in the SCLC component. For descriptive purposes, H scores ≤50 were regarded as negative, and those >50 were regarded as positive. To classify SCLC molecular subtypes, an unsupervised hierarchal clustering based on expression of the four subtype-defining transcription factors (ASCL1, NEUROD1, POU2F3, YAP1) was performed.
Statistical analysisSPSS software (V.21.0; SPSS) and Prism V.8.0 (GraphPad Software, San Diego, California) were used for data visualisation and statistical analysis. The correlation between continuous variables was calculated using the Spearman’s rank correlation. Correlations of subtype-defining markers’ expression between the resected specimens and paired biopsy specimens were examined using the Spearman’s rank correlation and Wilcoxon matched-pairs signed-rank test. Hierarchical clustering of samples based on the measured expression levels was performed with the Complex Heatmap R package (R V.3.6.3). Clinicopathological characteristics of each molecular subtype were analysed by the χ2 test, χ2 test of independence with Yate’s continuity correction or Fisher’s exact test. A Cox proportional hazards regression model was used to evaluate factors independently associated with OS and PFS. Variables with p<0.20 in the univariate analyses were considered in the multivariate Cox proportional hazards regression model. Survival curves were delineated using the Kaplan-Meier method, and differences between curves were estimated using the log-rank test. Statistical significance was set at p<0.05.
ResultsPatient and sample characteristicsA total of 195 SCLC patients were included in this study. The mean patient age was 61.5 years (range, 33–87 years), 106 (54.4%) patients were older than 60 years, 145 (74.4%) were men and 43 (22.1%) were never-smokers with de novo SCLC; none was histologic transformation of tyrosine kinase inhibitors-treated patients. The number of patients with pure SCLC and combined SCLC was 146 (74.9%) and 49 (25.1%), respectively. The NSCLC component for combined SCLCs was lung ADC (n=23), lung SCC (n=8) and LCNEC (n=18). 78 (40.0%), 38 (19.5%), 42 (21.5%) and 37 (19.0%) patients had stage I, II, III and stage IV disease, respectively. Most patients were treatment-naive before surgery or biopsy, with only 34 (17.4%) patients undergoing neoadjuvant chemotherapy (ChT). Beside surgical resection, SCLC patients also received adjuvant ChT with or without adjuvant thoracic radiotherapy according to the lung cancer treatment guidelines of our hospital; thus, one hundred and thirty-one (67.2%) patients received ChT, 60 (30.8%) patients received radiotherapy, and 81 (41.5%) patients received prophylactic cranial irradiation (PCI) treatment.
We collected 216 specimens from 195 patients with SCLC, including 150 surgically resected primary tumours, 17 metastatic samples by biopsy, 28 pleural effusions and 21 lung biopsies paired with surgically resected SCLC.
Expression of molecular subtypes and predictive markers and their correlationsWe examined the expression of molecular subtypes and predictive markers for the samples (n=195) besides the paired biopsies (n=21). When dichotomised into positive versus negative using an H-score threshold of >50, the ASCL1, NEUROD1, POU2F3, YAP1, DLL3 and MYC-positive expression rates were 70.3%, 56.9%, 14.9%, 19.0%, 75.4% and 22.6%, respectively. The expression distribution of these markers is listed in table 1.
Table 1Expression of these subtyping and predictive markers of SCLC
A significant positive association was observed between ASCL1 and DLL3 (Ρ=0.7256, p<0.0001), whereas a significant negative association was observed between POU2F3/YAP1 and DLL3 (Ρ=−0.2618, p<0.0001 and Ρ=−0.1967, p<0.0001). In contrast to DLL3, expression levels of MYC had a strong positive association with those of POU2F3/YAP (Ρ=0.6053, p<0.0001 and Ρ=0.2152, p<0.0001) and a negative association with those of ASCL1 (Ρ=−0.2481, p<0.0001) (figure 1A). Additionally, we observed no significant correlation between NEUROD1 and DLL3/MYC (figure 1A). Representative histopathological images revealing the relationship between subtype-specific protein expression and DLL3/MYC expression are shown in figure 1B.
 Figure 1
Figure 1 Molecular subtypes and predictive markers’ expression correlations. (A) DLL3 positively correlated with ASCL1, whereas negatively correlated with POU2F3/YAP1. MYC positively correlated with POU2F3/YAP1, whereas negatively correlated with ASCL1. (B) Representative histopathological images revealing the relationship between subtype-specific protein expression and DLL3/MYC expression. ASCL1, achaete-scute family BHLH transcription factor 1; DLL3, delta-like ligand 3; POU2F3, POU class 2 homeobox 3; YAP1, Yes1-associated transcriptional regulator.
Subtype-specific protein expressions in SCLC-paired resected tumours and biopsiesThe expression of subtype-defining markers in resected tumours and paired biopsies is shown in figure 2A. To determine the relationship between subtype-defining markers’ expressions in resected tumours and biopsies, we examined the correlation between these markers’ expressions in the matched specimens using Spearman’s rank correlation test. Strong associations of ASCL1 (Ρ=0.8603, p<0.0001), NEUROD1 (Ρ=0.8326, p<0.0001), POU2F3 (Ρ=0.6950, p<0.0001) and YAP1 (Ρ=0.7466, p<0.0001) expressions were detected in the paired two groups (figure 2B). Next, to investigate subtype-specific markers heterogeneity, we assessed the differences in these marker expressions between the resected and biopsy tissues using the Wilcoxon matched-pairs signed-rank test. The heterogeneity of NEUROD1 expression significantly differed between the resected and biopsy specimens (p=0.048), and these data suggested that NEUROD1 expression in resected tumours was stronger than in biopsies (figure 2C).
 Figure 2
Figure 2 Comparative analysis of paired resected-biopsy tumours. (A) The expression of subtype-defining markers in resected tumours and paired biopsies. (B) Spearman’s rank correlation tests were used to investigate the expression correlation between resected tumours and paired biopsies, and showed strong associations of ASCL1, NEUROD1, POU2F3 and YAP1 expressions in the paired two groups. (C) By Wilcoxon matched-pairs signed-rank tests, we found that the heterogeneity of NEUROD1 expression significantly differed between the resected and biopsy specimens (p=0.048), revealing that NEUROD1 expression in resected tumours was stronger than in biopsies. ASCL1, achaete-scute family BHLH transcription factor 1; NEUROD1, neuronal differentiation 1; POU2F3, POU class 2 homeobox 3; YAP1, Yes1-associated transcriptional regulator.
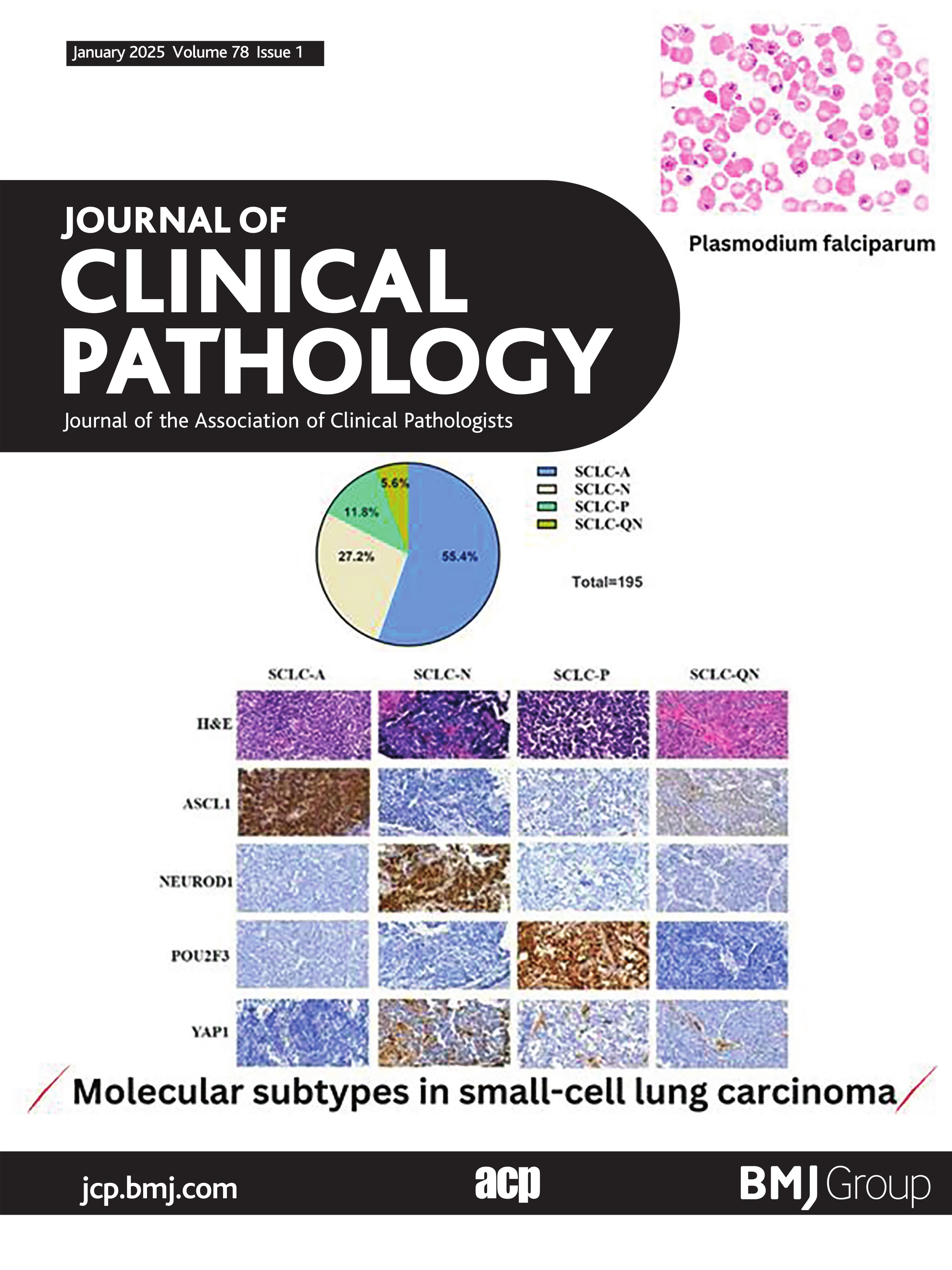
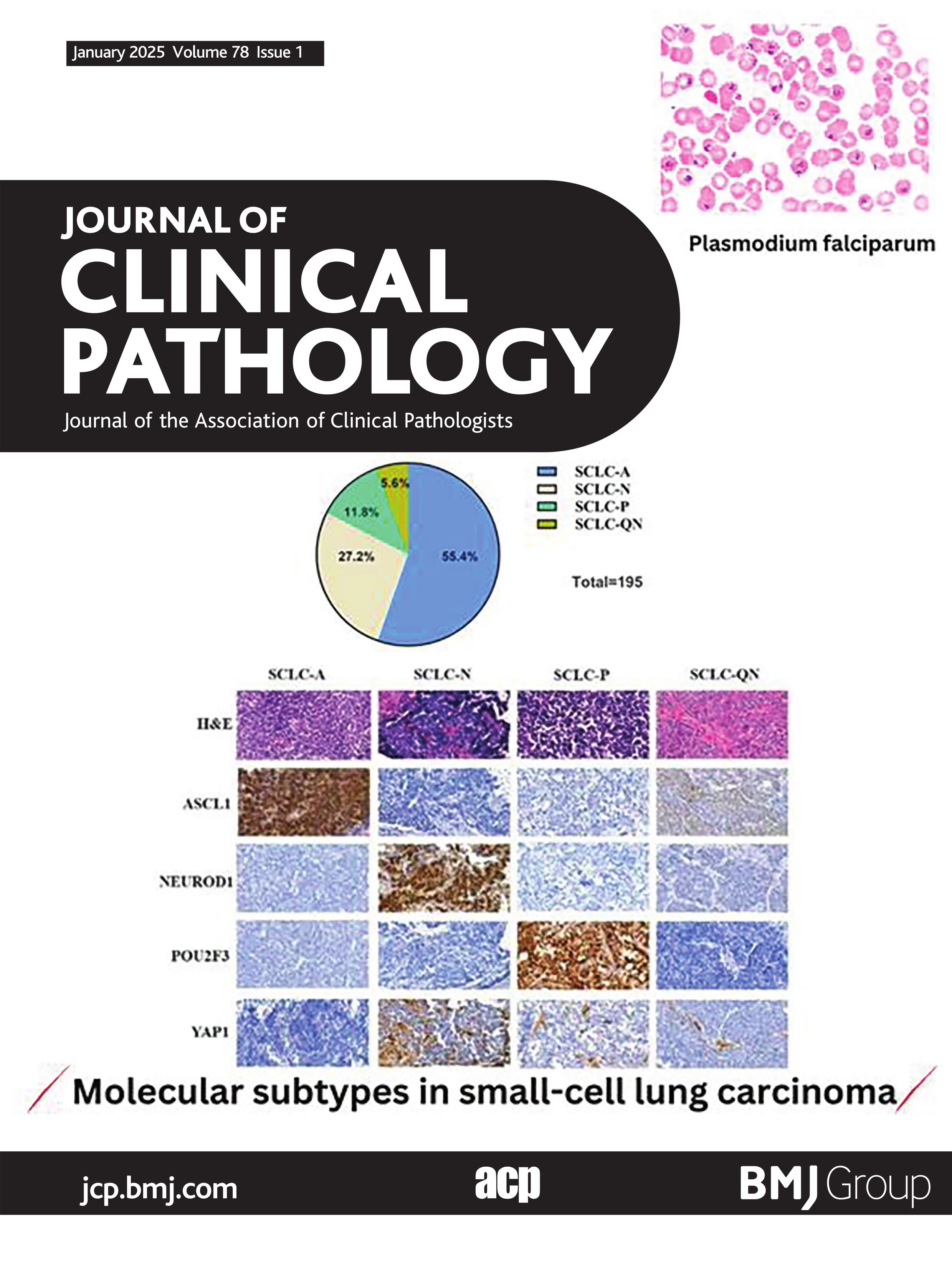
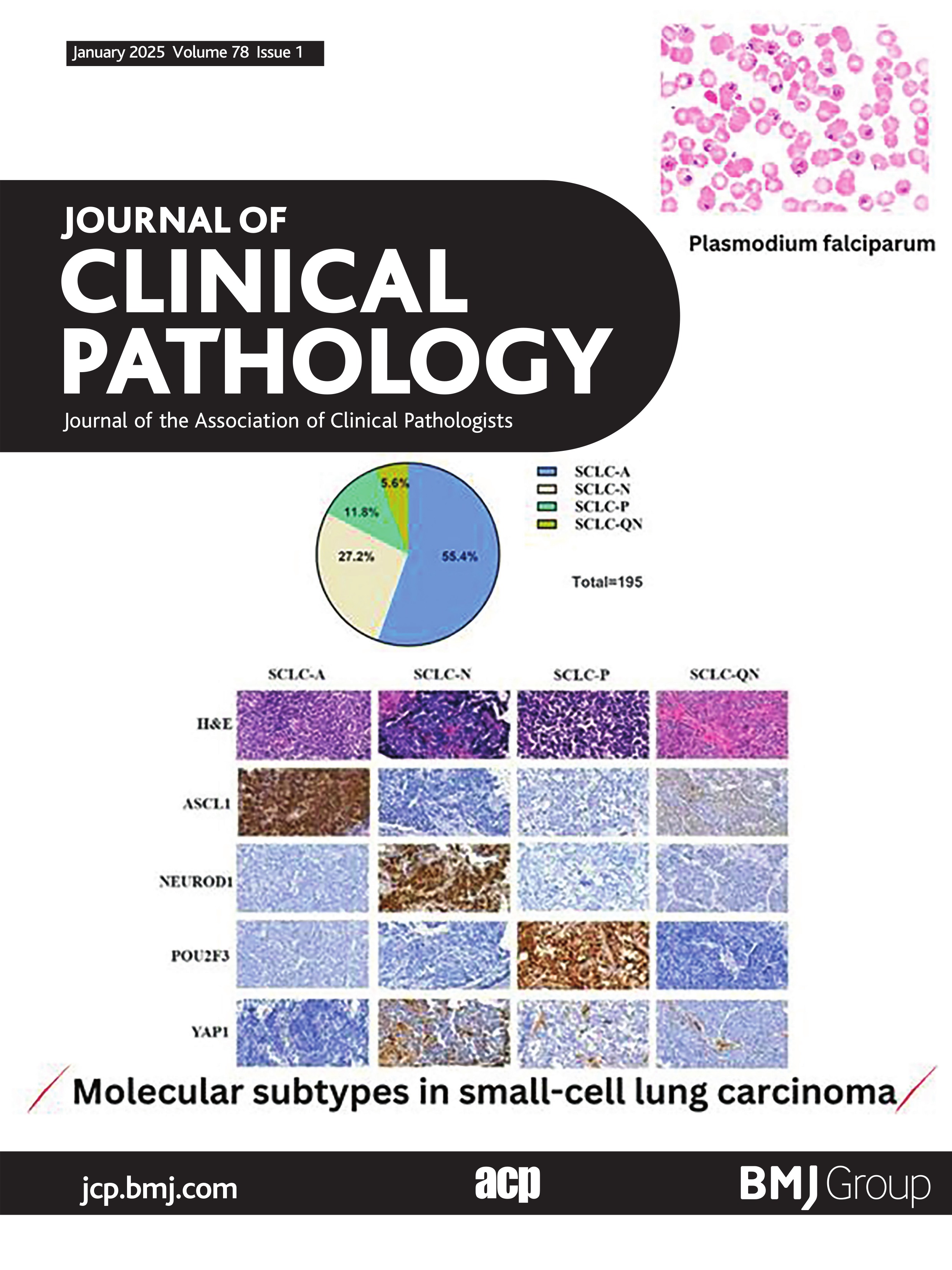
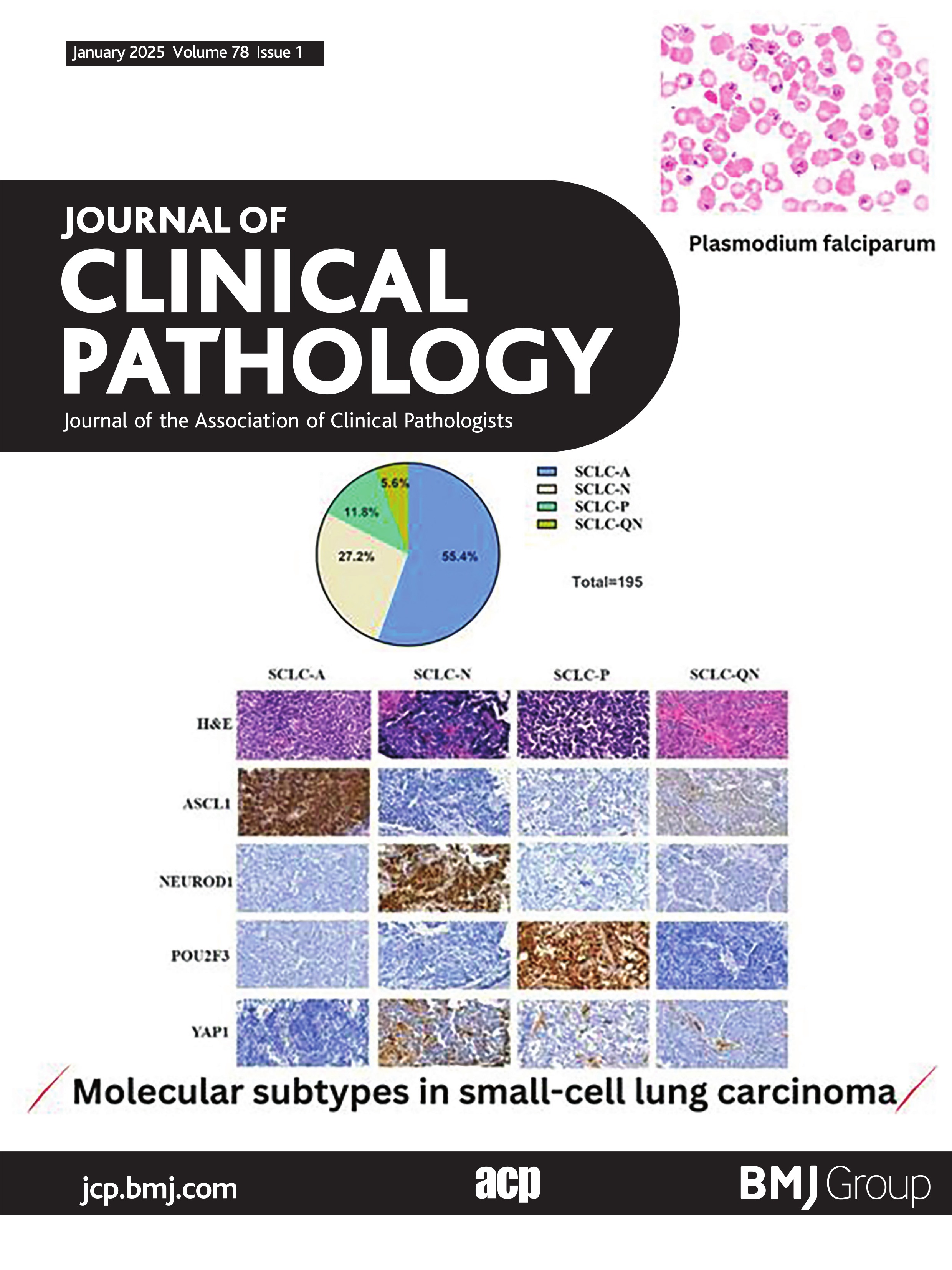
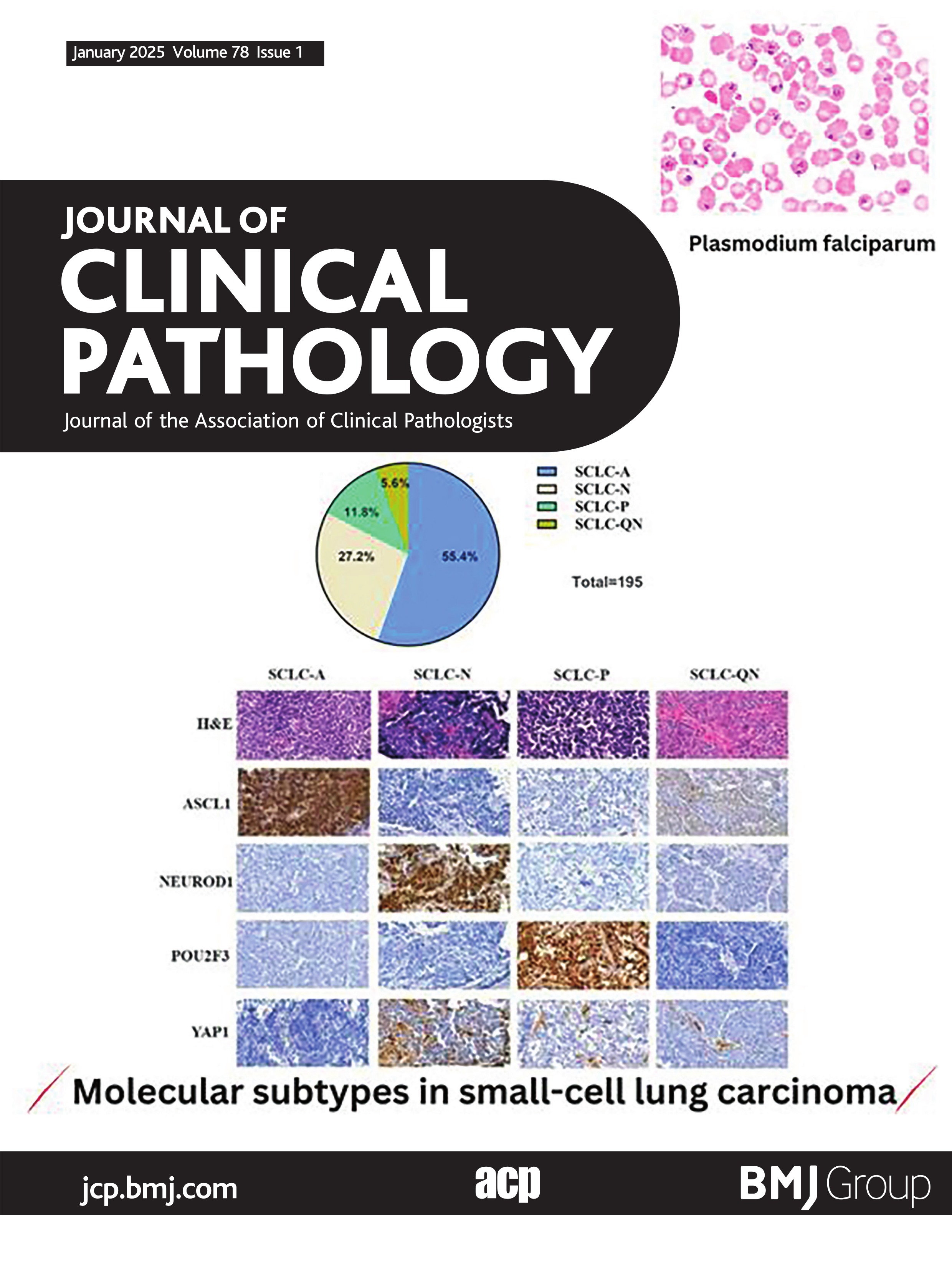
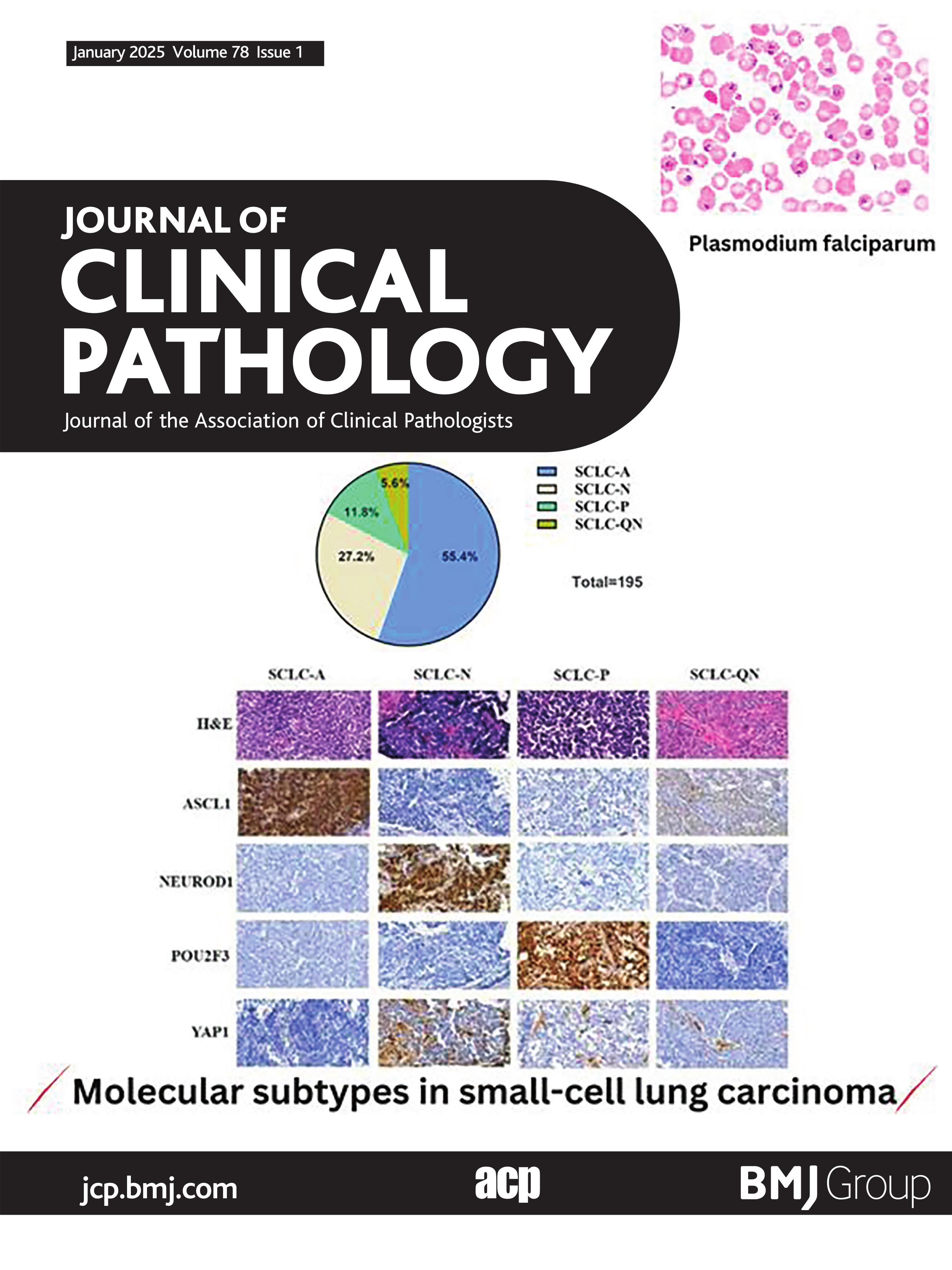
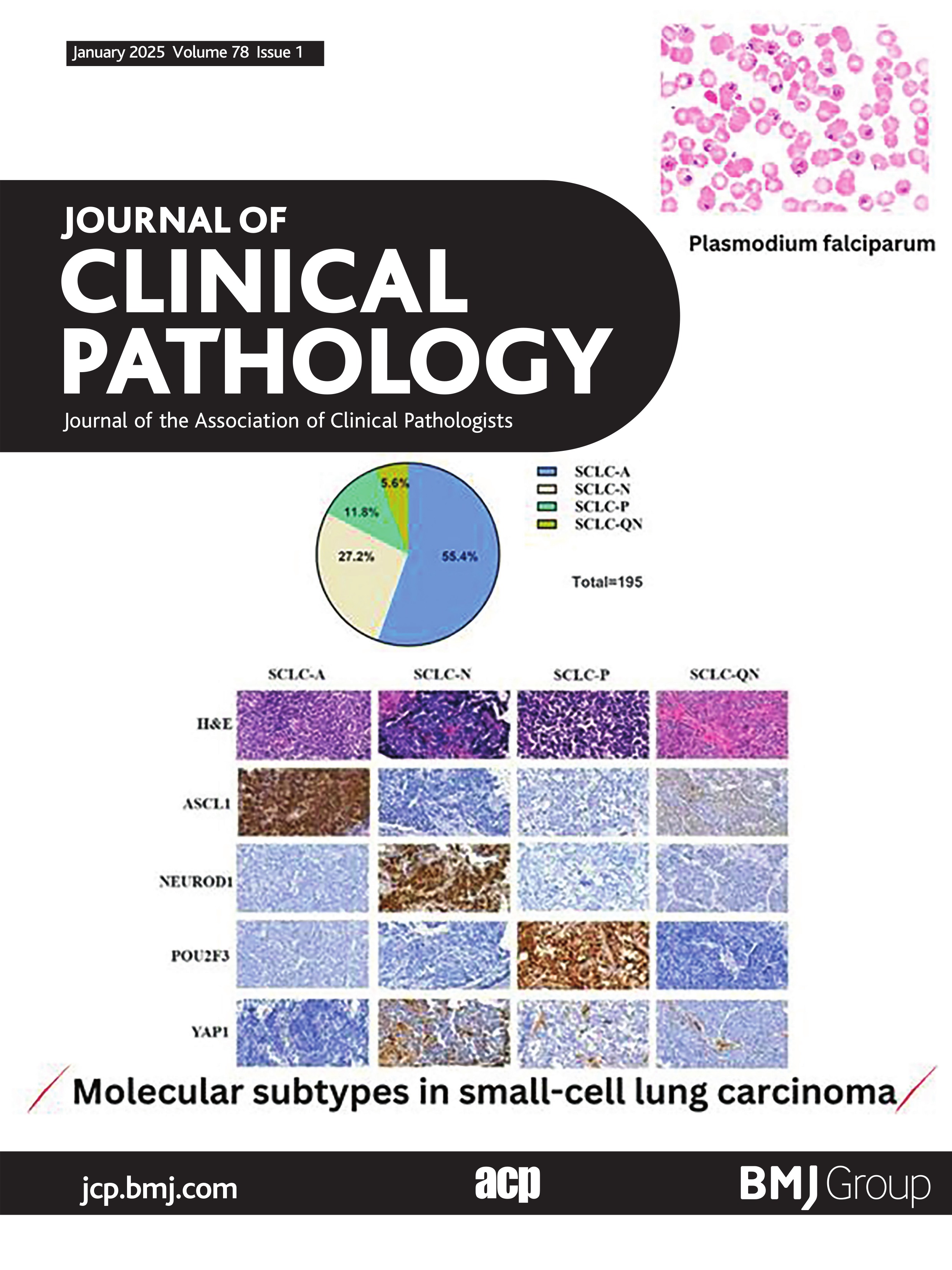
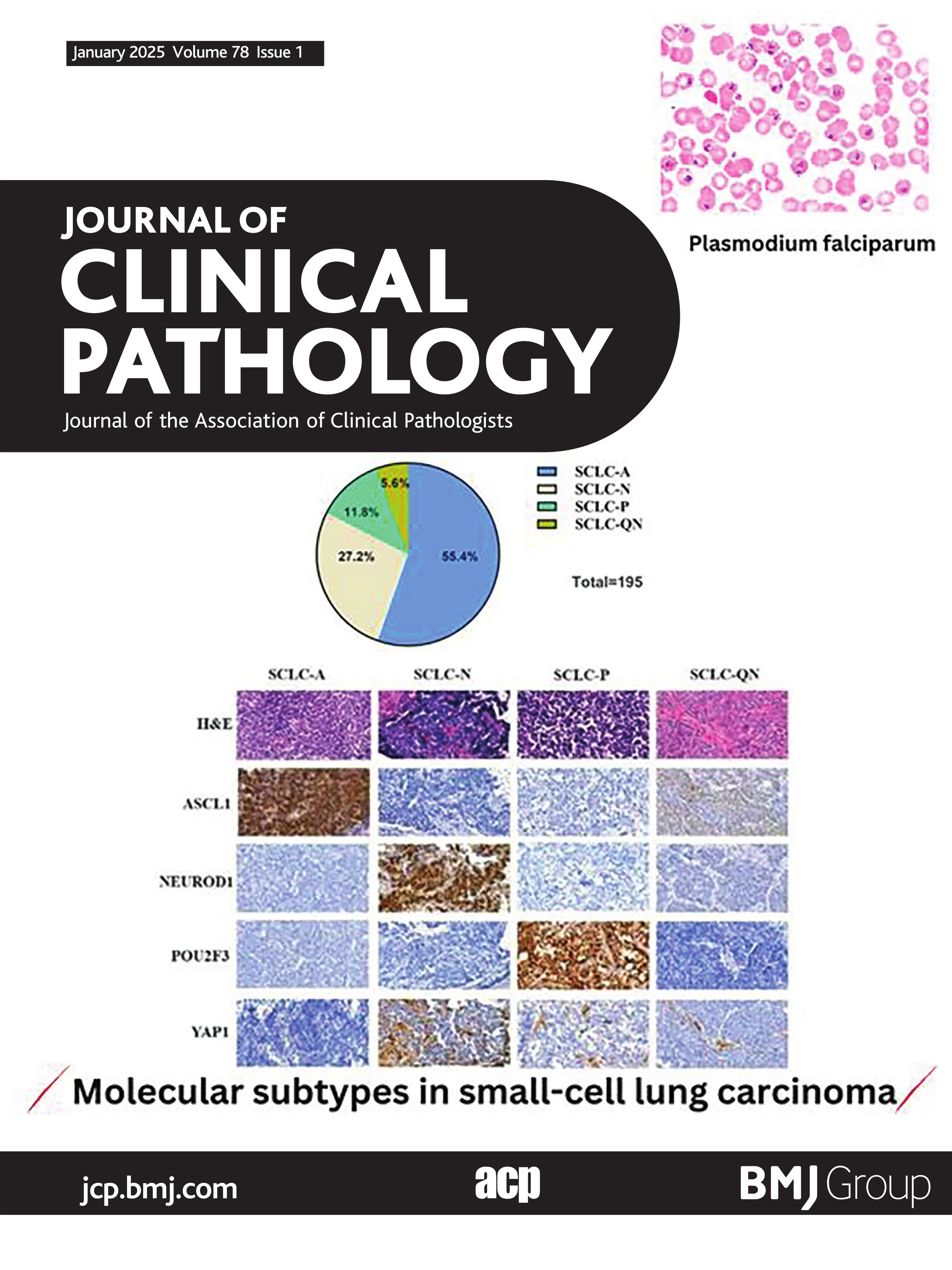
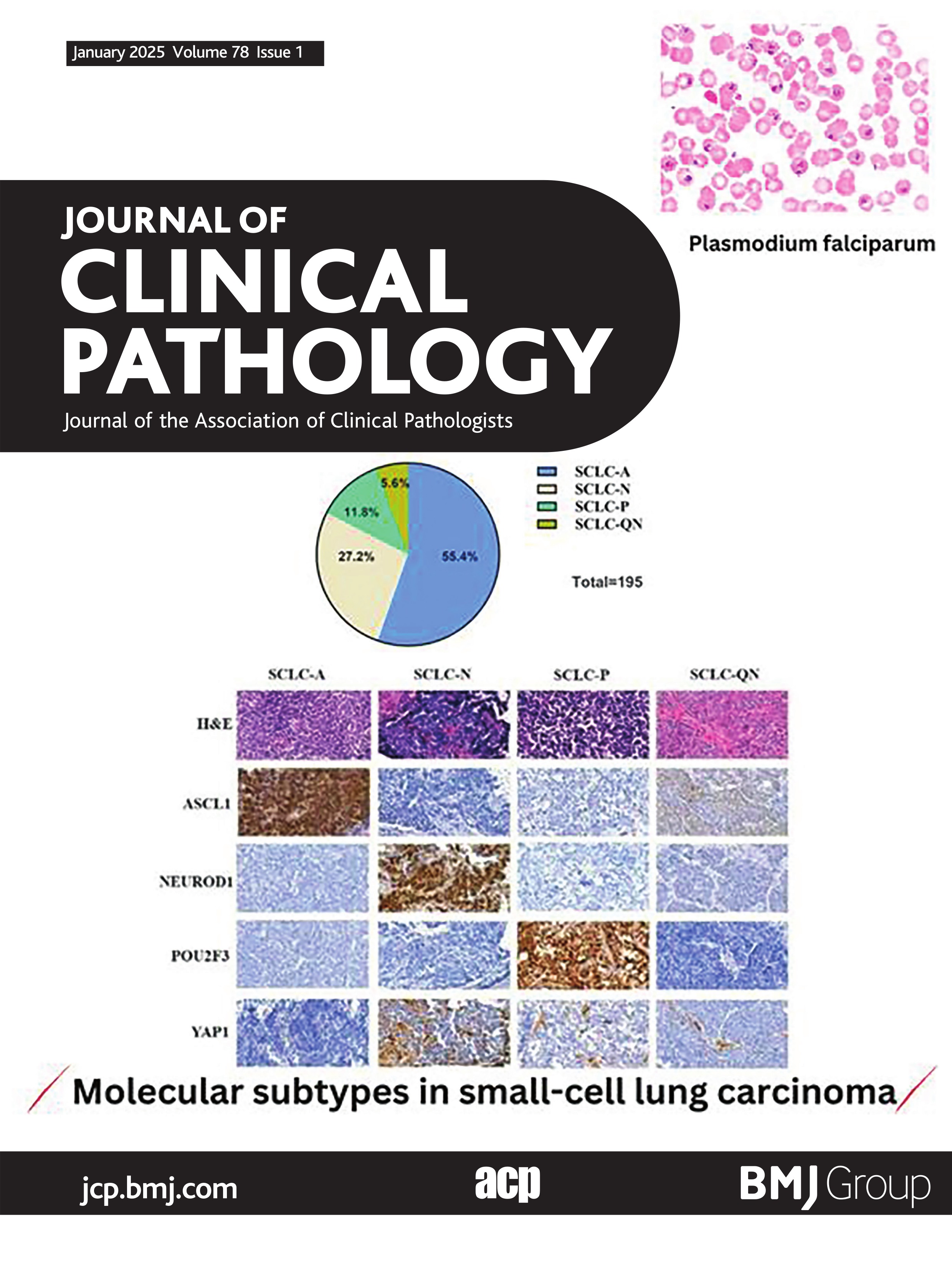
Molecular subtypes and clinicopathologic correlationUnsupervised hierarchical cluster analyses were performed to identify the dominant marker in 195 samples besides the paired biopsies (n=21) based on the IHC expressional levels of the four molecular subtype markers (ASCL1, NEUROD1, POU2F3 and YAP1). Differential expression of the four markers clearly distinguished four major SCLC subtypes. In addition to SCLC-A (ASCL1-dominant), SCLC-N (NEUROD1-dominant) and SCLC-P (POU2F3-dominant), cluster analyses identified a fourth, quadruple-negative SCLC subtype (SCLC-QN) characterised by the low expression of all four subtype-specific proteins (figure 3A). As shown in figure 3B, 55.4% (n=108), 27.2% (n=53), 11.8% (n=23) and 5.6% (n=11) were categorised as SCLC-A, SCLC-N, SCLC-P and SCLC-QN, respectively. Representative histopathological images of the marker-defined SCLC molecular subtypes are shown in figure 3C.
 Figure 3
Figure 3 Molecular subtypes distribution. (A) Unsupervised hierarchical clustering analyses of ASCL1, NEUROD1, POU2F3 and YAP1 immunohistochemistry expression were performed in 195 samples besides the paired biopsies. Differential expression of the four markers clearly distinguished four major SCLC subtypes. In addition to SCLC-A (ASCL1-dominant), SCLC-N (NEUROD1-dominant) and SCLC-P (POU2F3-dominant), cluster analyses identified a fourth, quadruple-negative SCLC subtype (SCLC-QN) characterised by the low expression of all four subtype-specific proteins. (B) The pie chart illustrating the percentage of each dominant molecular subtype tumour in specimens besides the paired biopsy (n=195). (C) Representative histopathological images of SCLC by molecular subtypes. ASCL1, achaete-scute family BHLH transcription factor 1; NEUROD1, neuronal differentiation 1; POU2F3, POU class 2 homeobox 3; SCLC, small-cell lung carcinoma; YAP1, Yes1-associated transcriptional regulator.
We then analysed the relationship between molecular subtypes and clinicopathologic parameters. Notably, combined SCLCs were significantly enriched in the subtype of SCLC-P, and patients with the tumour of SCLC-P tended to have a history of smoking. For the NSCLC components of combined SCLCs, ADC was more prevalent in SCLC-A, while LCNEC was more commonly seen in SCLC-P. All SCLC-A cases showed DLL3 expression, similarly, we observed MYC expression in all SCLC-P cases (table 2).
Table 2Clinicopathological characteristics of each molecular subtype in small cell lung carcinoma
Survival analysis in relation to clinicopathologic parameters and molecular subtypesAll patients were followed-up routinely. By the follow-up deadline of 30 April 2023, 123 cases (63.1%) had tumour recurrence or metastasis, 50 (25.6%) were disease-free, 108 (55.4%) died, 65 (33.3%) were alive and 22 (11.3%) were lost during follow-up. The median OS and PFS were 40 and 28 months, respectively. One-year, 3-year and 5-year OS and PFS rates were 87.3% and 60.1%, 47.4% and 29.5%, and 23.7% and 15.6%, respectively.
To assess the prognostic value of ASCL1, NEUROD1, POU2F3, YAP1, DLL3 and MYC expression and other clinicopathologic variables, we performed univariate Cox’s regression analyses, and the results are summarised in online supplemental table S2. Next, clinicopathologic parameters with p value less than 0.2 in univariate analyses were included in a multivariate Cox proportional hazards regression model (figure 4). Furthermore, Kaplan-Meier analysis was used to compare the risk stratification of subgroups according to these prognostic factors, which were included in multivariate analysis (figure 5 and online supplemental figure S1). Together, these results revealed median and advanced TNM stage (II–IV) was associated with short OS and PFS compared with early TNM stage (I), and TNM stage was an independent prognostic factor in the cohort (figure 5A). Additionally, an older age (HR=1.530, 95% CI 1.023 to 2.288; p=0.038) was independently correlated with worse clinical survival outcomes, while performing PCI was an independent predictive factor (HR=0.547, 95% CI 0.365 to 0.819; p=0.003) (figure 4A and figure 5A).
 Figure 4
Figure 4 Multivariate analyses for prognostic significance of clinicopathologic parameters in the cohort. Clinicopathologic parameters with p value <0.2 in univariate analyses were included in a multivariate Cox proportional-hazards regression model. (A) An older age and median and advanced TNM stage (II and IV) were independently correlated with worse clinical survival outcomes, while performing PCI was associated with favourable OS. (B) Advanced TNM stage (II and IV) was independently correlated with short PFS, conversely, performing PCI was associated with prolong PFS. ASCL1, achaete-scute family BHLH transcription factor 1; DLL3, delta-like ligand 3; OS, overall survival; PCI, prophylactic cranial irradiation; PFS, progression-free survival; POU2F3, POU class 2 homeobox 3; YAP1, Yes1-associated transcriptional regulator; TNM, tumor-node-metastasis.
 Figure 5
Figure 5 Kaplan-Meier estimates for OS and PFS. (A) Kaplan-Meier analysis was used to compare the risk stratification of subgroups according to the prognostic factors in multivariate analysis. (B) The Kaplan-Meier curves for OS and PFS according to molecular subtypes and NE-phenotype or non-NE-phenotype, showing that there was no survival difference among molecular subtypes (SCLC-A, SCLC-N, SCLC-P and SCLC-QN) and there were no significant differences in OS and PFS between NE-phenotype and non-NE-phenotype cohorts. However, SCLC patients with a non-NE phenotype tended to have a better outcome. OS, overall survival; PFS, progression-free survival; SCLC, small-cell lung carcinoma; SCLC-A, SCLC-ASCL1-dominant; SCLC-N, SCLC-NEUROD1-dominant; SCLC-P, SCLC-POU2F3-dominant; SCLC-QN, SCLC characterised by the low expression of all four investigated transcription factors.
We then conducted a subgroup analysis according to molecular subtypes. The median OS and PFS values in patients with the SCLC-A, SCLC-N, SCLC-P and SCLC-QN subtypes were 38.7 and 27.1 months, 39.7 and 28.1 months, 40.1 and 32.9 months and 55.3 and 28.6 months, respectively. The Kaplan-Meier curves for OS and PFS according to molecular subtypes were examined, and no difference was found among molecular subtypes (SCLC-A, SCLC-N, SCLC-P and SCLC-QN) (figure 5B). In addition, based on the NE differentiation of their tumours, patients were further dichotomised into the two groups of NE phenotype (SCLC-A and SCLC-N) and non-NE phenotype (SCLC-P and SCLC-QN); there were no significant differences in OS and PFS between the two groups (p=0.1551 and p=0.9141) (figure 5B). However, a consistent trend was noted towards a better SCLC outcome for patients in the non-NE-phenotype group.
DiscussionThe positive rate of ASCL1 (70.3%) in this study was consistent with previously reported 59.5%–79.2%,9 11 13 16 17 23 24 whereas that of NEUROD1 (56.9%) was higher.9 11 13 16 17 However, SCLC-A was the predominant subtype, which was also in line with prior studies.9 10 13 14 16–18 The high NEUROD1-positive rate might be attributed to antibodies used and the different clinical stages of patients included. Notably, we observed a significant coexpression of ASCL1 and NEUROD1, which is consistent with those of other reports in the literature.9 12 17 18 In support of this, other recent RNA-based investigations have also suggested that the SCLC-N subtype has greater transcriptional overlap with SCLC-A tumours,2 25 and recent genetically engineered mouse SCLC models have demonstrated temporal evolution from one molecular subtype to another (such as the transition from SCLC-A to SCLC-N). These findings indicate transcriptional plasticity in SCLC, which may explain the discordant expression of ASCL1 and NEUROD1 in various studies. However, consistent with prior studies,9–11 16–18 most SCLCs (82.6%) were characterised by dominant expression of ASCL1 and/or NEUROD1 (SCLC-A and SCLC-N) in our study population, and the ASCL1/NEUROD1 double-negative subtype (SCLC-P and SCLC-QN) comprised only a minor subset of SCLC (17.4%).
No YAP subtype was found in our study, which is in line with other tissue-based studies that failed to identify a distinct subtype with high YAP1 expression.4 9 12 18 Conversely, a small subset of SCLC with dominant YAP1 expression was reported in primary SCLC tumours,10 14 26 and it also has been pointed out that some samples may be sourced from YAP1-expressing subclones of SCLC in cell line and circulating tumour cell-derived explant data.27 28 Collectively, the role of YAP1 as a subtype-defining marker in SCLC warrants further investigation for clarification. Notably, given the previously reported association of YAP1-abundance and ChT-resistance in preclinical studies,29 30 the YAP1 lineage might indeed be more prominent in patients already treated with ChT and could emerge during disease evolution.31 In addition, caution should be taken with the results concerning YAP1 expression by using bulk RNA sequencing as YAP1 could be positive in stromal cells and the NSCLC component of combined SCLC.9 10
Consistent with the previous studies,9 11 23 32 33 a positive correlation was observed between ASCL1 and DLL3 expression. Furthermore, we detected significantly negative associations between POU2F3/YAP1 and DLL3, indicating that POU2F3/YAP1-dominant SCLCs might be unsuitable for targeted therapy for DLL3. Unlike the in vitro findings that MYC is often overexpressed in the NEUROD1-subtype SCLC lines,27 we found no significant correlation between NEUROD1 and MYC expression, and expression levels of MYC had a strongly positive association with those of POU2F3/YAP and a negative association with those of ASCL1. These findings are in agreement with those of a recent study by Qu et al.10 Collectively, our results show the significance of guiding targeted therapy for patients with SCLC and the need to be validated in prospective clinical trials.
In the present study, 49 cases of combined SCLC were enrolled, and this is the largest cohort of combined SCLC samples to investigate the molecular subtype distribution in terms of histological subtypes (pure and combined SCLC).9 16–18 In the first comprehensive IHC-based study on SCLC molecular subtypes in patient samples,9 combined SCLCs were significantly enriched in the non-NE phenotype, and in line with this, we observed significant enrichment of SCLC-P in the combined SCLC cohort. Conversely, Hwang et al found that SCLC-N was more commonly seen in the combined SCLCs.18 SCLC molecular subtypes were not associated with histology in the other two studies,16 17 while the number of combined SCLC cases included was relatively small. In addition, we collected information on the NSCLC components of combined SCLCs to explore whether they differed according to the molecular subtype, and the results revealed that ADC was more prevalent in SCLC-A, while LCNEC was more commonly seen in SCLC-P, which requires further prospective validation.
Although no difference was found among molecular subtypes, we noted that SCLC with a non-NE phenotype tended to have a better outcome, and this finding is generally consistent with other reports in the literature.12 13 Conversely, SCLC-P (p=0.023) was an independent poor prognostic factor for resected SCLC in the Cox multivariate analysis by Ding et al,16 and in the most recent study, it was pointed out that YAP1 expression was a poor prognostic factor for patients undergoing surgical resection.18 The difference in prognosis prediction is probably due to the constitution of different TNM stages and therapeutic regimens, relatively small cohort size or different antibodies used, and studies in larger cohorts will be needed to further evaluate the prognostic and treatment implications of different SCLC molecular subtypes.
There were some limitations in our study. First, it was a retrospective and single-centre study, which inevitably caused selection bias. Second, due to the limited number of paired lung biopsies of surgically resected SCLC primary tumours, the number of studied populations was limited reducing the statistical power. Third, targeted therapy of DLL3 and MYC is not yet applied in the clinic, together with the nature of the retrospective study, we could not identify the exact correlation of molecular subtypes and predictive markers’ expression with treatment response.
ConclusionsIn summary, our study validated the proposed molecular subtype classification of SCLC in a large cohort of various patient samples using whole-section FFPE-based IHC. No YAP1 subtype was found. The expression of DLL3 was positively associated with that of ASCL1 and negatively associated with that of POU2F3/YAP1, whereas MYC had the opposite effect. Strong associations of subtype-defining markers in the paired resected-biopsy specimens were detected, proving the feasibility of biopsy samples for identifying SCLC molecular subtypes. We observed significant enrichment of SCLC-P in the combined SCLC cohort, and ADC was more prevalent in SCLC-A, while LCNEC was more commonly seen in SCLC-P. No survival difference was found among molecular subtypes, while SCLC with a non-NE phenotype tended to have a better outcome. Collectively, our results provide clinical insights into the diagnostic and prognostic significance of SCLC subtype classification and contribute to the selection of individualised treatments and subtype-specific management.
Data availability statementData are available upon reasonable request. All data needed to evaluate the conclusions in the paper are present in the paper and/or the Supplementary Materials.
Ethics statementsPatient consent for publicationEthics approvalThe study protocol was approved by the Ethics Committee of Peking University Cancer Hospital and the local review board (2023KT23).
留言 (0)