Study design
This was a descriptive study of a secondary analysis of data from the large, multicenter, observational study conducted across nine hospitals in Japan between January 1, 2015, and December 31, 2019.
Setting
Data were obtained for patients who were evaluated for LGP at nine hospitals in Japan. For hospitals in which electronic medical records were introduced during the study period, only patients evaluated after the introduction of electronic medical records were included.
Selection of participants
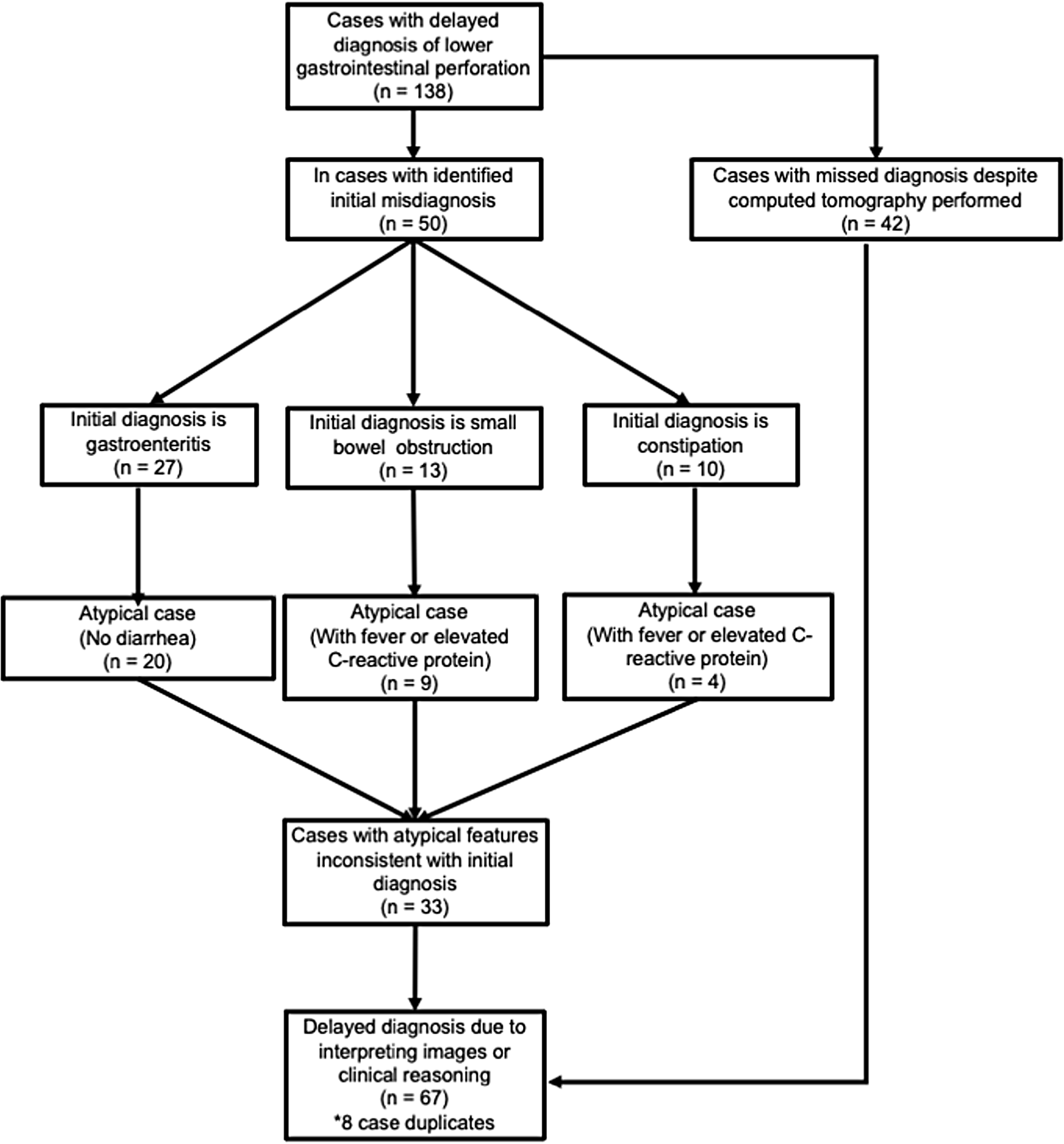
Overall, 138 cases of delayed diagnosis were identified out of the 439 cases with LGP in the previous study. The original study included patients manifesting symptoms indicative of LGP, with confirmation obtained via diagnostic imaging or surgical intervention. Patients under 15 years old, those with perforations caused by trauma, medical interventions, or conditions like mesenteric ischemia, appendicitis, or diverticulitis, and those with upper gastrointestinal perforations were excluded. Secondary lower gastrointestinal perforations were excluded due to their dependence on underlying diseases, complicating diagnostic assessment.
Variables
The following variables were quantified for analysis: timely diagnosis, delayed diagnosis, and diagnostic error. Timely diagnosis was defined based on the following two criteria [7]. The first was a diagnosis of a LGP at the time of the initial visit to a facility with CT imaging capacity. The second was a diagnosis of probable LGP during the initial visit at a facility without CT imaging capacity, with the patient immediately referred to an appropriate medical facility for investigation of the acute abdominal pain. A “near miss” was defined as an incorrect diagnosis during the initial visit at a non-CT facility, with immediate transfer of the patient to a hospital with CT imaging capacity for appropriate diagnosis. “No-fault” cases were defined as an absence of perforation findings on initial CT imaging, with an ultimate diagnosis of LGP after additional testing, as previously defined [7]. Cases that did not meet the classification for “near miss,” “no-fault,” or “timely diagnosis” were classified as “delayed diagnosis.” After a review of the 439 cases with a resultant diagnosis of LGP, a delayed diagnosis was identified in 138 cases.
The clinical reasoning scenarios that could prevent a delay in the diagnosis of LGP were examined. The three most common initial diagnoses associated with a delayed diagnosis were gastroenteritis, constipation, and small bowel obstruction. The typical clinical course of these diseases, which differentiates them from a LGP, is as follows. Acute gastroenteritis is typically associated with diarrhea [13, 14], with gastroenteritis without diarrhea being atypical. Constipation is not likely to cause fever or an elevation in acute-phase inflammatory markers, such as C-reactive protein (CRP) [15]. Lastly, small bowel obstruction is less likely to cause fever or a CRP elevation; in fact, CRP elevation is atypical for small bowel obstruction without complication [16]. Furthermore, a previous study identified an elevation in CRP ≥ 10 mg/L in 77% of patients with LGP and fever in 51% of cases [7]. These two findings are sufficiently consistent to differentiate between LGP and gastroenteritis, constipation, or small bowel obstruction. Based on this evidence, we hypothesized that the following three clinical reasoning scenarios resulted in a delayed diagnosis of LGP. First, CT images were obtained; however, the LGP was missed due to the absence of a radiology report for the emergency physician. Second, an initial diagnosis of gastroenteritis was made despite the absence of diarrhea. Third, an initial diagnosis of constipation or bowel obstruction was made despite the presence of fever and elevated inflammatory markers. To verify the face validity of the hypothesized scenarios, we examined the CT imaging history for all 138 cases in the delayed diagnosis group. Additionally, details on the presence/absence of fever, diarrhea, and elevated CRP were further extracted from the medical reports for the 27 cases of gastroenteritis, 13 cases of constipation, and 10 cases of small bowel obstruction as the initial analysis.
Study size
No statistical sample size calculations were conducted because this study is a secondary descriptive analysis and is exploratory in nature.
Quantitative variables
The primary outcome measure was the frequency with which the delay in diagnosing LGP could be prevented by revising the clinical reasoning process in 50 cases initially diagnosed with gastroenteritis, constipation, or small bowel obstruction. The secondary outcome measure was the frequency with which the diagnosis of LGP was missed despite CT imaging in a group of 138 cases where the diagnosis was delayed.
Statistical methods
Outcome variables were described as a count (percentage) or median (interquartile range) as appropriate for the data type. All descriptive data were calculated using the EZR (Easy R) software Stata statistical software (Saitama Medical Center, Jichi Medical University, Saitama, Japan).
Ethical approval
This study was approved by the ethical review board of Showa University Koto Toyosu Hospital (No. 20T7044) and conducted in accordance with the Declaration of Helsinki.



留言 (0)