Study design
This is a registry-based observational study using the Pan-Asian Trauma Outcome Study (PATOS) database. The manuscript adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines [7].
Study setting
PATOS is a large multinational emergency medical services (EMS)-based trauma registry network across the Asia-Pacific region, initiating data collection in 2015 [8]. The main purposes of PATOS were to benchmark emergency trauma care and improve survival outcomes in the Asia-Pacific region. The registry collected standardized data from 10 countries: India, Japan, Malaysia, Philippines, South Korea, Singapore, Taiwan, Thailand, United Arab Emirates, and Vietnam [9]. Trauma care systems, especially EMS systems, in Asia-Pacific countries were relatively new and underdeveloped compared to the systems in European countries and the United States.
The EMS systems varied among countries. Most of the countries had both Advanced Life Support (ALS) and Basic Life Support (BLS) teams [10]. Fire departments typically provided prehospital trauma care in countries like Korea, Japan, and Singapore, while hospital-based or community-based teams were common in Thailand, Malaysia, and the Philippines [11, 12]. The EMS team leaders were physicians in more than half of the participating sites. Nurses, emergency medical technicians (EMT), and paramedics were team leaders in Korea, Malaysia, Philippines, Singapore, and Taiwan [12].
Most participating sites were urban academic tertiary care hospitals, with a quarter designated as trauma centers [9]. Trauma teams were available in half of the participating sites. Licensed trauma surgeons were available in two-thirds of the participating sites [9].
On the national level, trauma care systems varied due to differences in health care infrastructure, resources, and policy priorities. National trauma triage protocols and patient transfer protocols existed in Korea and Japan [13]. Most participating sites generally followed Advanced Trauma Life Support (ATLS), with exceptions in Korea, Singapore, and Japan where national trauma guidelines existed [13].
Study data source
The PATOS registry gathered data from 36 participating hospitals (27 tertiary, 8 secondary, and 1 primary hospital) across the Asia-Pacific region [9]. The registry collected trauma patients data of any severity who were transported by EMS ambulances in developed communities or non-EMS (non-professional) vehicles in developing communities to the emergency department of the participating hospitals [8].
To ensure data consistency and quality across participating sites, each site designated a research coordinator or principal investigator responsible for data collection, extraction, and input. The PATOS Data Quality Management Committee oversaw the central data cleaning process, conducted routine audits, and provided feedback to research teams to maintain high data quality standards. Additionally, regular meetings were held between the committee and site investigators to address inconsistencies and ensure adherence to standardized protocols [8].
Population
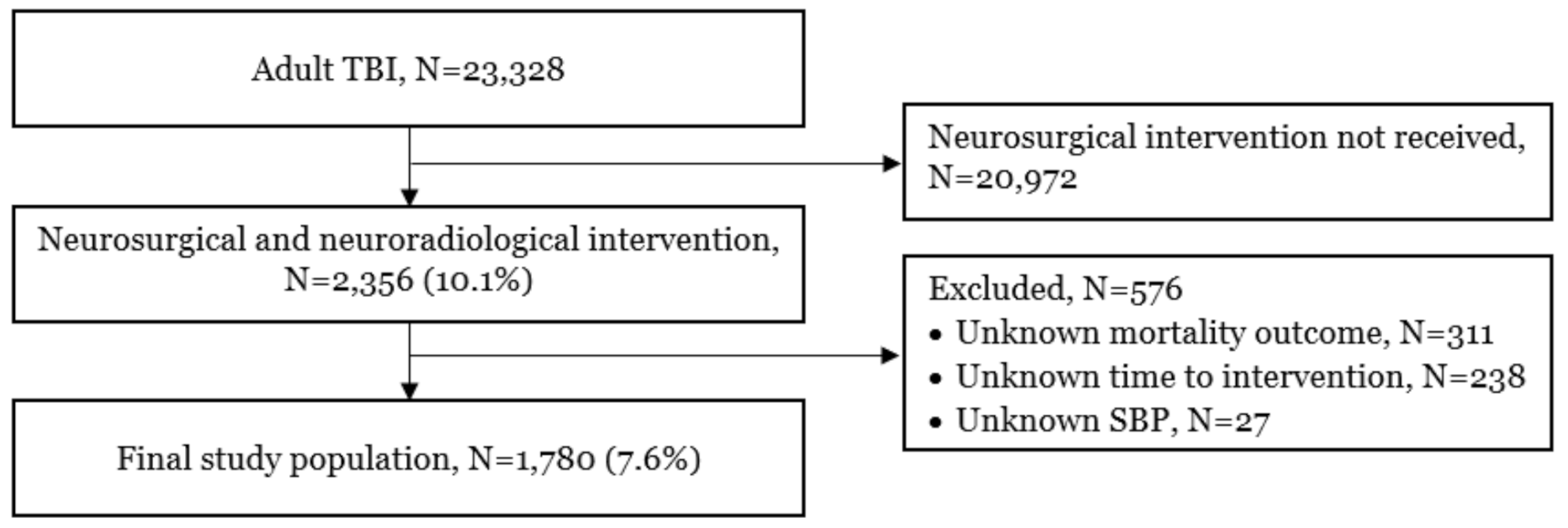
This study included all adult (≥ 18 years) TBI patients who received any neurosurgical or neuroradiological interventions from every participating site during January 2015 to December 2022. The International Classification of Diseases 10th Edition (ICD-10) code S06 (intracranial injury) was used as an index for TBI patients. Neurosurgical and neuroradiological interventions were defined as the first recorded neurological operative procedures performed on the patients in the PATOS database, including both neurosurgical operations (such as craniectomy, craniotomy, and hematoma evacuation) and neuroradiological intervention (such as angioembolization) in the head region.
Patients were excluded if the primary outcome was missing. We also excluded patients whose time to intervention could not be measured. We also excluded patients with unknown systolic blood pressure.
Variables and measurementsExposure definition and measurement
The primary exposure, time to intervention, was defined as the interval between ED arrival and the initiation of the neurosurgical or neuroradiological intervention. In the latest guideline, the time of injury was used as a reference starting time [14]. However, in this study, we used ED arrival time instead for the following reasons: (1) the exact time of injury was likely inaccurate and missing in some cases, and (2) using ED arrival time as a starting point until the time of the surgery would directly reflect the effectiveness of in-hospital management.
The second exposure is the mode of transport. Prehospital transport was defined as the direct transportation of trauma patients from the scene to the ED. Interhospital transport was defined as the secondary transfer of trauma patients from another hospital.
Confounder definition and measurement
Confounder variables were categorized into 5 groups: general factors, injury factors, prehospital care, ED and hospital care, and injury severity. General factors included age, sex, and Charlson’s comorbidity index [15]. The injury factors included the intent of the injury (accidental, intentional), mechanisms of injury, place of injury, alcohol intake, and day of injury (weekday vs. weekend), and time of the injury. Prehospital care data included the top-level personnel, airway management, breathing & ventilation management, and fluid management. ED and hospital care data included vital signs, Glasgow Coma Scale (GCS), and types of intervention (neurosurgical versus neuroradiological intervention). For injury severity, we used the excess mortality ratio-based injury severity scale (EMR-ISS) which was a diagnosis-based injury severity scale for large data sets derived from the ICD-10 codes to depict injury severity [16].
Outcome measures
The primary outcome was death, defined as in-hospital mortality. The secondary outcome was unfavorable neurological outcomes at discharge, defined as Glasgow Outcome Scale (GOS) 1–3 [17]. GOS is a 5-point scale score, categorized as (1) dead, (2) vegetative state, (3) severe disability, (4) moderate disability, and (5) good recovery [18]. This scale was chosen for its wide acceptance and standardized evaluation of functional recovery in TBI research.
Statistical analyses
Confounding and outcomes variables were compared between exposure groups using median and interquartile range (IQR) for continuous variables, and numbers and percentages for categorical variables. Statistical significances were considered when the p-values were less than 0.05 using Wilcoxon sum rank test for continuous variables, and Chi-square test for categorical variables.
The categorization of time to intervention was determined using the Restricted Cubic Spline (RCS) analysis with four knots to model the non-linear relationship between time to intervention and mortality. Two key time points (1.9 and 4.1 h) were identified as knots where the relationship between time to intervention and mortality exhibited noticeable shifts, based on statistical analysis and visual inspection of the spline curve. The remaining two knots were placed at the extremes of the distribution to ensure adequate flexibility in fitting the model. Based on this analysis, patients were stratified into three groups according to time to intervention: early (< 1.9 h), intermediate (1.9–4.1 h), and delayed (> 4.1 h). These intervals not only reflect statistically significant inflection points but also aligned with practical clinical workflows in TBI management. The early group included cases requiring immediate intervention. In contrast, the delayed group represented interventions that occurred after stabilization, allowing for more comprehensive resuscitation, evaluation, or transfer. The intermediate group aligned with the critical therapeutic window frequently emphasized in TBI care, balancing timely intervention with adequate preparation.
For the main analysis, W score was also used to compare the difference in survival outcomes among three groups of patients: early, intermediate, and delayed interventions. W score is the difference between observed survivors and expected survivors per 100 patients [19]. The formula of the W score is (A-B)/(C/100). A is the actual number of survivors. B is the expected number of survivors based on the probability of survival (PS) from the Trauma and Injury Severity Score (TRISS) model which was derived from the Major Trauma Outcome Study (MTOS) in 1995 to predict survival and disabilities with coefficient revision in 2009 [20]. C is the total numbers of patients used for calculation of the PS. For example, a positive W score of + 2 indicates that there are 2 more survivors than predicted per 100 patients. Thus, W score represents the quality of the TBI care system within each group of patients. A positive W score indicates more survivors than predicted, reflecting superior care quality. A negative W score suggests fewer survivors than expected, potentially highlighting areas for improvement.
An additional analysis was performed using the multivariable logistic regression model. Potential confounding factors were tested and selected as confounders for the model when the p-value was less than 0.2 in univariate analysis between the exposures and factors. The association between exposure groups and outcomes was tested using multivariable logistic regression analysis and adjusted odds ratios (AOR) and 95% confidence interval (95% CI) were calculated from the model. We also compared the effect size of the time to intervention on the outcomes across the mode of transport in the final model as interaction terms.
Handling of missing data
Monotone logistic regression imputation was used to address missing data for key covariates, ensuring that the analysis included as many cases as possible while maintaining data integrity. The imputation model included patient demographics, injury severities and injury mechanisms as predictors to account for relationships among variables.
Critical variables such as primary outcomes and time-to-intervention were not imputed. Cases with missing values for these variables were excluded from the analysis to preserve the reliability and robustness of the results.



留言 (0)