Despite advancements in dosimetry development, MTPD is currently hindered by complex logistics, additional patient burden, and resource constraints in clinical application. Furthermore, there is still limited evidence regarding dosimetry in predicting therapeutic responses and identifying potential toxicities [18, 19]. In this retrospective study, we investigated the influence of errors in a simplified dosimetry method from a clinical perspective. Here, we focused on the treatment of 177Lu-PSMA-617 RPT and correlated the dosimetry with follow-up data on serum PSA decline rate, toxicity over cycles, and overall survival [17].
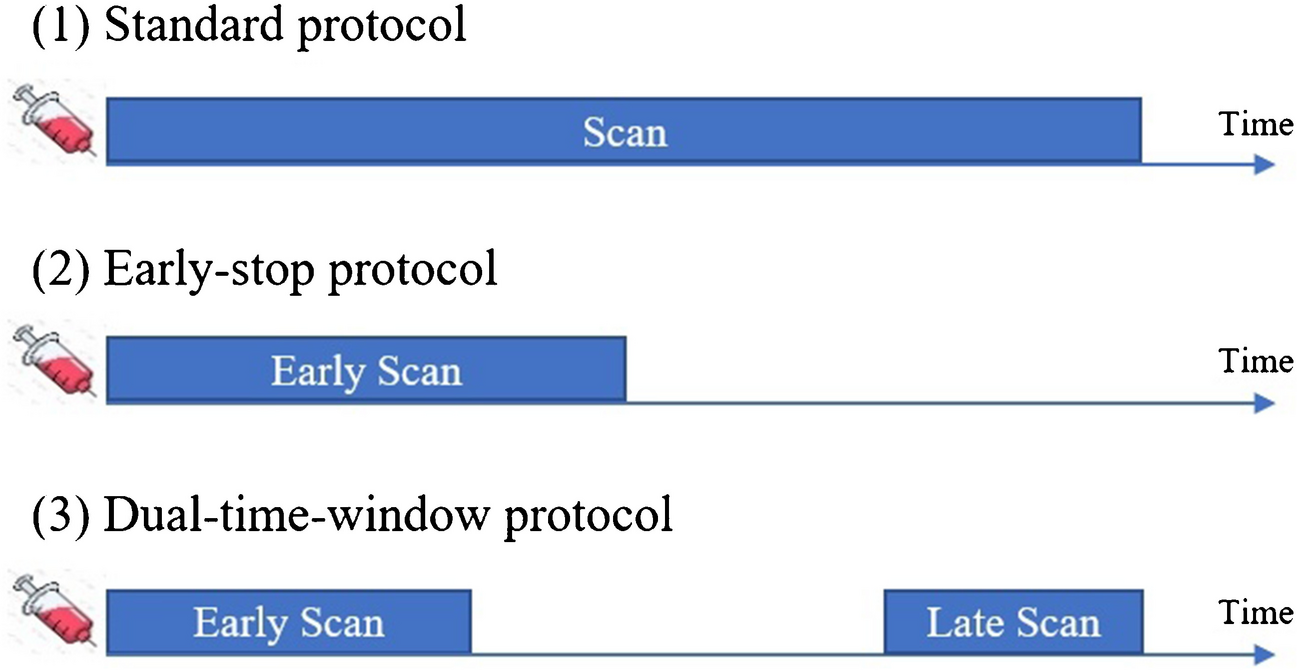
In this study, we selected the Hänscheid STPD method as the simplified dosimetry method, which has already been applied in 177Lu-PSMA-617 dosimetry calculations [21, 33]. With the retrospective data, we could only select the time-points from 1–3 days post-injection for the application of the Hänscheid method, which aligns well with the Hänscheid method's recommended time window [26, 30]. For quality control, we checked the eligible time window using the population effective half-life estimated from our data to confirm the suitability of our dosimetry time-points. Nevertheless, these time-points may not represent the best performance of the Hänscheid method [21, 26, 30, 33], which could have even lower errors.
Our MTPD findings of OARs were similar to previous dosimetry studies [23, 34]. For example, in the first cycle, the kidneys’ MTPD per unit of administered activity was 0.36 ± 0.13 Gy/GBq, which is within the reference range from the VISION trial (mean: 0.43 Gy/GBq, range: 0.22–0.83 Gy/GBq) [34], and also similar to the kidneys’ dose (0.39 Gy/GBq) reported in a voxelized dosimetry study [23]. For dosimetry over 6 cycles, our results demonstrated that the kidneys’ MTPD was 17.20 ± 6.58 Gy when the mean cumulative injection activity was 39.91 ± 1.42 GBq, also within the range from the VISION trial, which is 9.1- 29 Gy when 44.4 GBq injection activity was given [34]. However, our MTPD results for bone marrow from the first cycle (0.45 ± 0.53 Gy/GBq) showed a higher dose compared to the blood sample-based dose (mean: 0.035 Gy/GBq, range: 0.02–0.13 Gy/GBq) from the VISION trial [34], and also higher than the voxelized image-based dose found in Violet’s study (mean: 0.11 Gy/GBq, range: 0.01–0.34 Gy/GBq) [23]. The gap may be related to the challenges in accurately segmenting non-tumor-infiltrated bone marrow. We utilized an automatic whole-body bone mask and subtracted the higher PSMA-PET SUV (> 50% SUVmax) region, which is easy to perform but does not accurately delineate the marrow. The observed correlation between bone marrow dose and toxicity grading hints that both MTPD and STPD measurements could provide meaningful and relevant data for assessing the impact of radiopharmaceuticals, despite the limitations of our segmentation method. Nevertheless, our results showed a similar tumor dose (2.02 ± 1.68 Gy/GBq) compared to Steffie’s finding (all lesion median: 1.69 Gy/GBq, range: 0.41–10.34 Gy/GBq) [35].
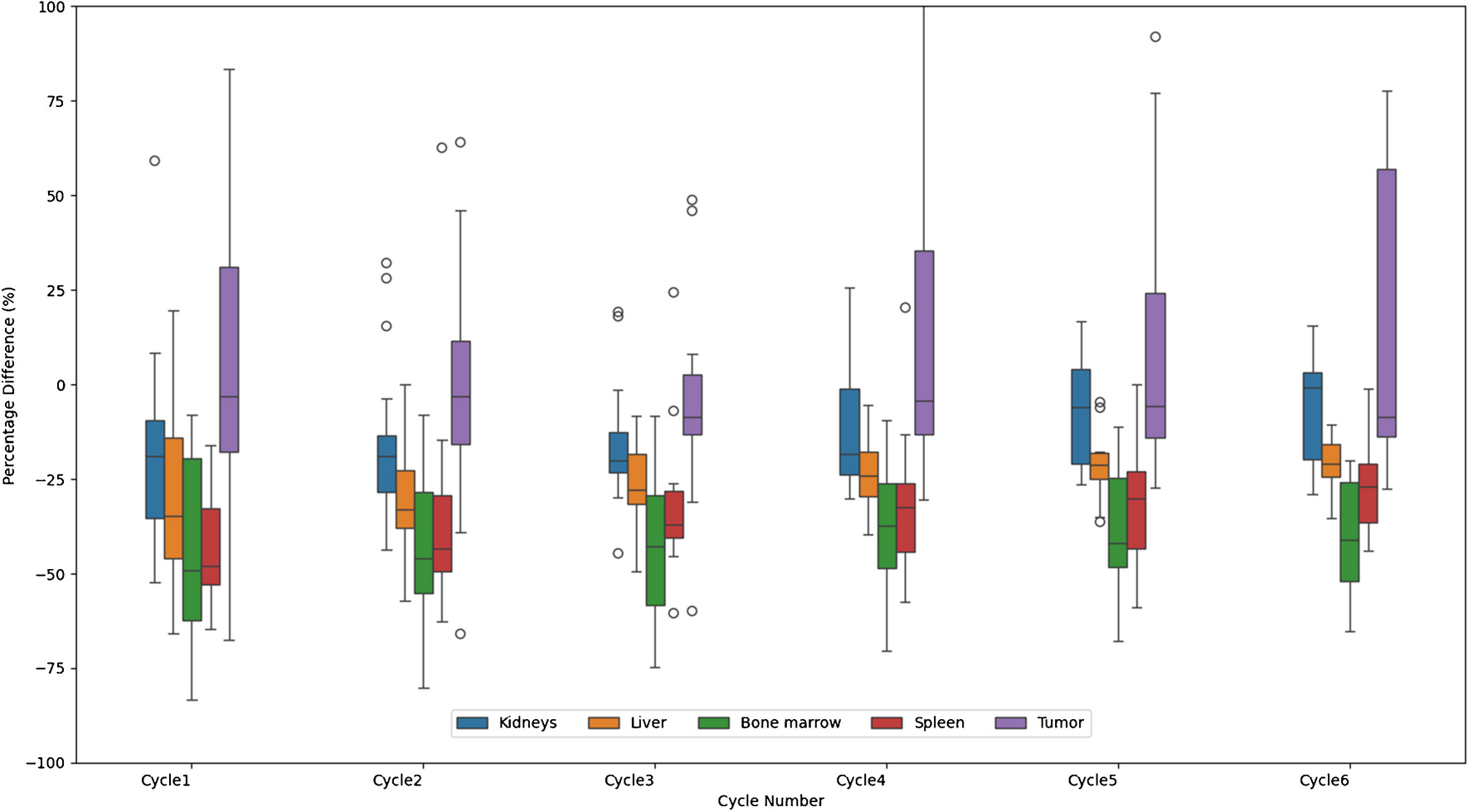
Our results confirmed a strong agreement between STPD and the referenced MTPD for tumors and all the tested OARs (Spearman correlation’s p < 0.001 for all). When assessing the error of STPD relative to MTPD in our cohort, we observed an increase in RMSE across therapy cycles. This can be attributed to a combination of variances in the optimal condition of Hänscheid’s approximation [20, 21], and possible changes in metastasis composition, or treatment-induced radiobiological impacts [36, 37]. We did not find a comparison between STPD and MTPD for 177Lu-PSMA-617 RPT schemes over 6 cycles from previous studies. However, our results showed a larger range of error compared to previous report from the first 2 cycles, with percentage differences of the Hänscheid method compared with MTP being less than ± 20% [21]. Specifically, our results showed the largest error in bone marrow STPD, with its MPE up to 40.26% compared to MTPD. This significant error could be attributed to the spatial mismatch in the SPECT-SPECT image registration [25] and the heterogeneous red bone marrow distribution in different bone sites [38], which poses segmentation challenges in segmentation, particularly for patients with extensive bone metastases.
From a clinical perspective, the safety evaluation in our study found that renal doses from both STPD and MTPD approaches were below the established limits and consistent with clinical trials [31, 34, 39]. Furthermore, despite the great deviation between MTPD and STPD, in bone marrow we found the increasing MTPD and STPD were significantly correlated with anaemia grade (both p < 0.01), and no significant difference between the two corrections was found (Z = −0.39, p = 0.70). Additionally, the therapy response evaluation showed that both MTPD and STPD of tumor were significantly correlated with positive therapeutic outcomes (both p < 0.001), and there was no significant difference between the two correlations (Z = 0.56, p = 0.56). Note that the relationship between dose and PSA decline is observed to be nonlinear. Although we employed the Spearman’s correlation to take this nonlinearity into account, the correlation cannot fully reflect the radiobiological principles [8]. Ideally radiobiological modeling could provide more quantitative insight for the comparison, which could be future work if such kind of model can be developed [39]. Nevertheless, correlation is still the most practical and popular way in clinical assessment of the influencing factors of RPT radiobiological effects [22, 23].
This study is limited by its retrospective nature and small patient cohort. Potential biases from prior therapies, continued treatment-induced radiobiological shifts, and changes in metastasis composition during therapy cycles could impact the performance of both dosimetry methods in their associations with therapy outcomes [28, 29, 40,41,42]. In addition to the studied Hänscheid method, our findings need cross verification for other simplified dosimetry methods [20, 21, 26, 43,44,45].
Existing evidence demonstrates the potential of dosimetry in determining the treatment outcome of RPT including 177Lu-PSMA-617 RPT [22,23,24]. However, the demanding or acceptable accuracy of dosimetry measurements in clinical practice has not been well investigated, especially in practical dilemmas facing compromises with accuracy using simplified protocols. This study presents the first investigation of the influence of dosimetry errors on clinical predictive value. Despite the limitations, the preliminary findings of this study may trigger further investigation of the acceptable accuracy level of dosimetry measurements and in-depth discussion of their impact in clinical practice.








留言 (0)