Data source and sample
The Behavioral Risk Factor Surveillance System (BRFSS) survey is administered by the Centers for Disease Control and Prevention (CDC) and is the largest individual health behavior surveillance system in the United States. It is a cross-sectional annual telephone survey conducted in all 50 states, the District of Columbia, and three US territories (CDC 2023). The BRFSS consists of both core and optional modules to cover many topics regarding health-related risk behaviors and events, chronic health conditions, and use of preventive services. The core modules are asked by every state each year, and the optional modules used are selected by states and differ each year. Questions about cannabis use are in an optional “Marijuana Use” module that was used in Kentucky in 2020 and 2021. BRFSS data are publicly available without the geographic variable for county, but for this study we obtained the data set with county of residence under agreement with the KY Department for Public Health.
Measures
The BRFSS includes this preamble for the marijuana use module: The following questions are about marijuana or cannabis. Do not include hemp-based or CBD-only products in your responses. Participants were asked: During the past 30 days, on how many days did you use marijuana or cannabis? Possible answers ranged from 0 to 30 days. Respondents who reported at least one day of cannabis use were classified as people who currently use cannabis, with those who reported at least 20 days of use classified as heavy users. Those who did not report a number of cannabis use days, coded as either “don’t know/not sure” or “refused,” were excluded from analysis.
Participants who reported any cannabis use were then asked: What was the reason you used marijuana? Possible answers were 1) for medical reasons (like to treat or decrease symptoms of a health condition), 2) for non-medical reasons (like to have fun or fit in), or 3) for both medical and non-medical reasons. Participants who reported using cannabis were also asked: During the past 30 days, which of the following ways did you use marijuana the most often? Did you usually… Possible answers were 1) smoke it (for example, in a joint, bong, pipe, or blunt), 2) eat it (for example, in brownies, cakes, cookies, or candy), 3) drink it (for example in tea, cola, alcohol), 4) vaporize it (for example, in an e-cigarette-like vaporizer or other vaporizing device), 5) dab it (for example, using waxes or concentrates), or 6) use it some other way. For this study, we collapsed these modes into four categories. Eating and drinking were combined into group “Eat/drink,” dabbing and vaping were combined into group “Concentrate,” and both “Smoke” and “Other” remained on their own.
We used responses to other questions routinely included in the BRFSS survey to determine participant demographics. These characteristics included: six-level imputed age category, imputed race/ethnicity, computed income categories, computed level of education completed, health plan coverage, marital status, calculated sex variable, and county code. We collapsed the response categories for some questions for these analyses due to low response rates. The six-level imputed age variable was reduced to three categories: 18 to 34, 35 to 54, and 55 + . We used the imputed race/ethnicity variable and combined multiple categories due to low response rates. We left the imputed values of “White, Non-Hispanic” and “Black, Non-Hispanic” as categories of their own, and combined the values for “American Indiana/Alaskan Native Non-Hispanic,” “Hispanic,” and “Other race, Non-Hispanic” into one category, “Hispanic/Other.” We also combined values for computed levels of highest educational attainment. “Did not graduate High School” and “Graduated High School” were combined into one category, “High School Graduate or Below.” The two categories left on their own are “Attended College or Technical School” and “Graduated from College or Technical School.” Six computed income response categories were collapsed into three: “Less than $25,000,” “$25,000–49,999,” and “$50,000 + .” Finally, marital status responses of “Married” and “Member of unmarried couple” were combined into “Married/Cohabitating.” “Separated”, “Divorced”, and “Widowed” were all combined into one value, and “Never Married” was left as a category of its own.
The BRFSS includes several questions related to both cigarette smoking and alcohol use, which were included as covariates. We used two questions to ascertain smoking status: 1) Have you smoked at least 100 cigarettes in your entire life? and 2) Do you now smoke cigarettes every day, some days, or not at all? Never smokers are those who answered no to the first question, former smokers are those who answered yes to the first question then “not at all,” and current smokers are those who smoke both some days and every day. Current alcohol use is defined as participants who reported having at least one drink of any alcoholic beverage in the past 30 days.
The county of residence for each respondent was used to create a new variable indicating region of residence. The three regions we examined were the Appalachian region, as defined by the Appalachian Regional Commission (Appalachian Regional Commission 2022), the Delta region, as defined by the Delta Regional Authority (Delta Regional Authority 2023), and Central Kentucky. For participants who were missing county information, we used an imputed region variable from the BRFSS to ascertain the region of residence. The BRFSS imputed region variable represents the following six regions of Kentucky: Bluegrass, Central, Eastern, KIPDA, Northern, and Western. While there is some overlap between our three regions and the six imputed BRFSS regions, the KIPDA and Northern regions contain only counties located in what we defined as Central Kentucky. These two imputed regions were used to define the region of residence for some participants in Central Kentucky. At the time this data was collected, only one state bordering Kentucky had legal recreational use and sales (Illinois). Three bordering states had legal medical use (Ohio, Virginia, and West Virginia). Virginia legalized recreational use in July 2020, though recreational sales have yet to begin.
Data analysis
We conducted all analyses using SAS 9.4 (SAS Institute, Cary, NC), and followed CDC guidelines to ensure proper handling of the complex sampling design and survey weights to produce population-based prevalence estimates across the two years of pooled data (CDC 2022a). The use of the survey weights is necessary to make generalizations from the sample to the population, as they adjust for noncoverage and nonresponse and force the total number of cases to equal population estimates for each geographic region (CDC 2022b). We performed sensitivity analysis of different classifications of heavy use compared to daily use, using a range of at least 15–29 days. Cross-tabulation was used to assess cannabis use prevalence overall by demographic, socioeconomic, and geographic factors, and to assess modes of use and reason for use by the same. We also calculated age-adjusted rates of cannabis use for the Appalachian and Delta regions, using Central Kentucky as the reference population. Chi-squared tests were used to assess differences in these demographic, socioeconomic, and geographic factors by cannabis use status.
As a comparison to Kentucky’s overall prevalence of cannabis use, we calculated the total prevalence of cannabis use in other states where it was also illegal for any purpose. For 2020, this included Idaho, Indiana, Mississippi, South Carolina, Tennessee, and Wyoming, and for 2021, Idaho, Indiana, and Wyoming. We also calculated their modes and reasons for using cannabis. We chose these states because they are the only ones, besides Kentucky, where cannabis was illegal for any purpose at the time of data collection and used the BRFSS optional cannabis use module.
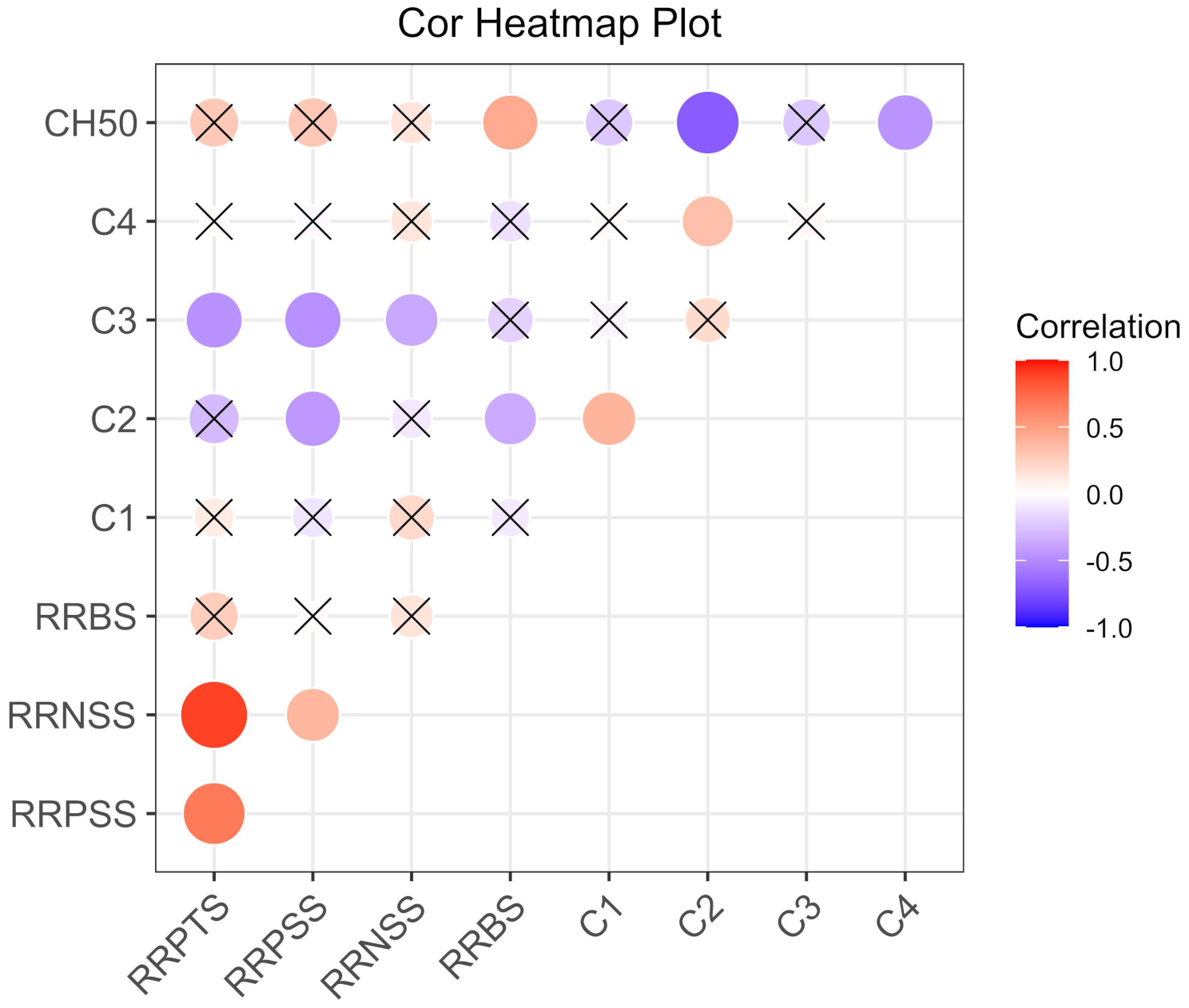
Lastly, logistic regression was used to examine predictors of cannabis use before and after adjustment for all other factors examined here. We assessed multicollinearity among the predictor variables using several methods. The Pearson correlation coefficients were computed to identify highly correlated pairs of variables. Variance Inflation Factors (VIFs) were calculated for each predictor, with VIF values exceeding 5 considered indicative of multicollinearity. Additionally, we examined the condition index, with values above 30 suggesting potential multicollinearity.






留言 (0)