
記住我
Bile is a biological fluid primarily composed of bile acids (BA), cholesterol, phospholipids, and proteins. It is synthesized in the liver and stored in the gallbladder. Its main physiological function is to facilitate the absorption of fats in the small intestine during digestion (Begley et al., 2005). Several bile-related diseases can alter bile function, but the most common is the formation of gallstones in the gallbladder or bile ducts, known as cholelithiasis or Gallstone (GS) disease. GS disease is one of the most common biliary tract diseases and a major public health concern in many countries. The incidence rate of gallstones is rising because of the change of living standard. Previous ultrasonography (US)-based epidemiologic studies have shown prevalence rates of 9.7–19.5% in European countries, 10–12% in the United States, and 2–5% in Asian countries (Yoo and Lee, 2009; Ryu et al., 2016; Sacks et al., 2018). Nearly 75% of patients with gallstones have no obvious symptoms in the initial stages (Sun et al., 2022). According to the site of lithiasis, cholelithiasis is mainly divided into cholecystolithiasis, hepatolithiasis, and extrahepatic bile duct stones. As the gallstones progress in development, they may trigger symptoms such as nausea, epigastric colic, diarrhea, anorexia, etc. Eventually, gallstone obstruction can lead to life-threatening conditions such as acute cholangitis, acute cholecystitis, and biliary pancreatitis (Tanaka et al., 2018; De Simone et al., 2022). Until now many strategies, including traditional open surgery, laparoscopic operation, and robotic surgery, have been applied for the treatment of cholecystolithiasis with choledocholithiasis (Lv et al., 2016). However, each strategy has its advantages and disadvantages and none of the methods could provide a satisfactory effect. For instance, while cholecystectomy is commonly performed, it carries risks of complications that can significantly compromise a patient's health and overall quality of life (Shabanzadeh et al., 2016; Barahona Ponce et al., 2021).
The recurrence of gallstones is of paramount importance, with high recurrence rates and a wide range of recurrence times. According to studies, the recurrence rate after gallstone surgery is approximately 10% to 50%, and recurrence may occur within months to years after surgery (Boerma et al., 2002; Allen et al., 2006; Ye et al., 2020). Various factors may influence gallstone recurrence, including dietary habits, lifestyle, genetic factors, gallbladder dysfunction, obesity, changes in bile biochemical components, etc. (Cheon and Lehman, 2006). Gallstone recurrence has significant implications for patient health and medical management. Recurrence may lead to patients experiencing pain, discomfort, and complications again, and may even require repeat surgical treatment. Additionally, recurrence increases medical costs and treatment burden for patients, causing inconvenience and anxiety in their lives.
Although the exact mechanisms underlying the formation of gallstones remain incompletely understood, the process often involves multiple factors, including genetic predisposition, age, gender, excessive hepatic cholesterol secretion, impaired gallbladder motility, abnormal bile composition (Nardone et al., 1995; Wang et al., 2010; Shabanzadeh et al., 2017; Idowu et al., 2019; Granel-Villach et al., 2020). Patients with gallstones often have comorbidities such as diabetes and cardiovascular diseases. These conditions, due to metabolic abnormalities, inflammatory responses, impaired gallbladder motility, and the effects of medications, increase the likelihood of gallstone formation and elevate the risk of recurrence (Man et al., 2022; Meng and Liu, 2023; Portincasa et al., 2023; Zhu et al., 2023). In addition, microbes are increasingly recognized as a potential causative agent in the development of gallstone disease. In recent years, an increasing number of studies have found that microbes play a crucial role in the formation and progression of gallstones (Grigor'eva and Romanova, 2020). Studies have shown the presence of living bacteria in gallstones. The flora in the biliary tract and duodenum are highly homologous and closely related to the formation of gallstones. Microbes can enter the biliary system from the duodenum by migrating through the sphincter of Oddi. They can also spread hematogenously to the liver and from there into bile (Neri et al., 2005; Helaly et al., 2014). When in bile, microbes play an important role as nucleating factors, participating in the alteration of bile chemical composition and the nucleation of gallstones, which may lead to complications such as gallbladder or bile duct infections (Maurer et al., 2005).
The number of molecular studies focusing on the association between the biliary microbiome and gallstones has been increasing (Swidsinski and Lee, 2001; Stewart et al., 2002; Begley et al., 2005; Stewart et al., 2006; Wang et al., 2018; Shen et al., 2020). For example, a study by Liang et al. demonstrated that patients with Sphincter of Oddi laxity (SOL) had a more severe bacterial infection in the bile duct microenvironment and a higher lithogenic potential (Liang et al., 2016). The microbiota in the intestine, bile ducts, and gallbladder may contribute to gallstone formation (Shen et al., 2015; Kose et al., 2018; Molinero et al., 2019; Hu et al., 2022). Additionally, dysbiosis of the biliary microbiota has been associated with the recurrence of bile duct stones (Choe et al., 2021; Tan et al., 2022). Several studies have indicated that different bacterial species and bile compositions may increase the formation of recurrent common bile duct (CBD) stones (Swidsinski and Lee, 2001; Stewart et al., 2006).
Previous research has employed various techniques to study bile microbiota, such as microbial culture, polymerase chain reaction (PCR) targeting specific bacteria, 16S rRNA sequencing, metagenomics, and transmission electron microscopy. Conventional techniques like these have long been used to identify biliary microbiota, but most have focused on bacteria (Brook, 1989; Swidsinski and Lee, 2001; Stewart et al., 2002). As early as 1989, Brook et al. used culture methods to grow bacteria from 123 bile specimens, with the main bacteria being Escherichia coli, group D Streptococcus, Klebsiella sp., Clostridium sp., Bacteroides sp., and Enterobacter sp. (Brook, 1989). Wu et al. (2013) were the first to apply 16S rRNA sequencing to bile and gallstone samples from cholesterol gallstone patients. Another study reported unbiased metagenomic sequencing of bile samples from 15 patients with common bile duct stones, identifying 13 novel bile bacteria (Shen et al., 2015). A recent study using 16S rDNA sequencing found potentially harmful microbes (Streptococcus, Clostridium, and Kocuria) in gallstones collected during surgery that may cause postoperative complications (Ploszaj et al., 2021).
In recent years, research on the microbiota in gallstone bile has become increasingly abundant. Most studies are based on 16S rRNA, and using this technology, the bile bacterial profiles of healthy individuals and gallstone patients have been revealed, showing significant differences in the relative abundance of different groups between the two sample sets. In bile samples from control group patients, sequences belonging to the family Propionibacteriaceae were more abundant, while in bile samples from gallstone patients, sequences belonging to Bacteroidaceae, Prevotellaceae, Porphyromonadaceae, and Veillonellaceae were detected at higher frequencies (Molinero et al., 2019). The taxonomic composition of bile bacterial communities also showed significant differences between common bile duct stones and gallbladder stones (Park and Park, 2024). Moreover, a recent culture-based study found differences in bile microbiota between gallstone patients with and without complications (Hirata et al., 2023). Additionally, a recent study combining 16S rRNA gene sequencing and proteomics identified 158 microbial taxa in bile samples, discovering taxa such as Streptococcus, Staphylococcus, and Clostridium, which may contribute to gallstone formation, as well as bacteria involved in biofilm formation, such as Helicobacter pylori, Cyanobacteria, Pseudomonas, E. coli, and Clostridium (Yang et al., 2023).
To date, there have been no large cohorts characterizing the microbiota in gallstone bile, and the understanding of microbial differences among different clinical characteristics remains insufficient. This study uses clinical bile microbiology culture results from 9,939 gallstone patients to explore the bile microbiota characteristics in gallstone patients and compare microbial differences among different clinical characteristics. This may provide a deeper understanding of the role of microbiota in gallstones and their association with various clinical features, potentially offering more effective strategies for the prevention, diagnosis, and treatment of gallstones, thereby reducing patient suffering and medical burdens.
2 Methods 2.1 Study design and participantsA total of 9,939 patients diagnosed with gallstones and admitted for surgery between January 2017 and December 2023 at the Third Hospital of Shandong Province were included in this study. The study was approved by the Institutional Ethics Committee of the Third Hospital of Shandong Province (KYLL-2024064). Clinical data, including age, gender, type of gallstone, gallstone size, comorbidities, and bile culture microbiota information, were extracted from medical records (Supplementary Tables S1, S2). The study design is outlined in Figure 1.
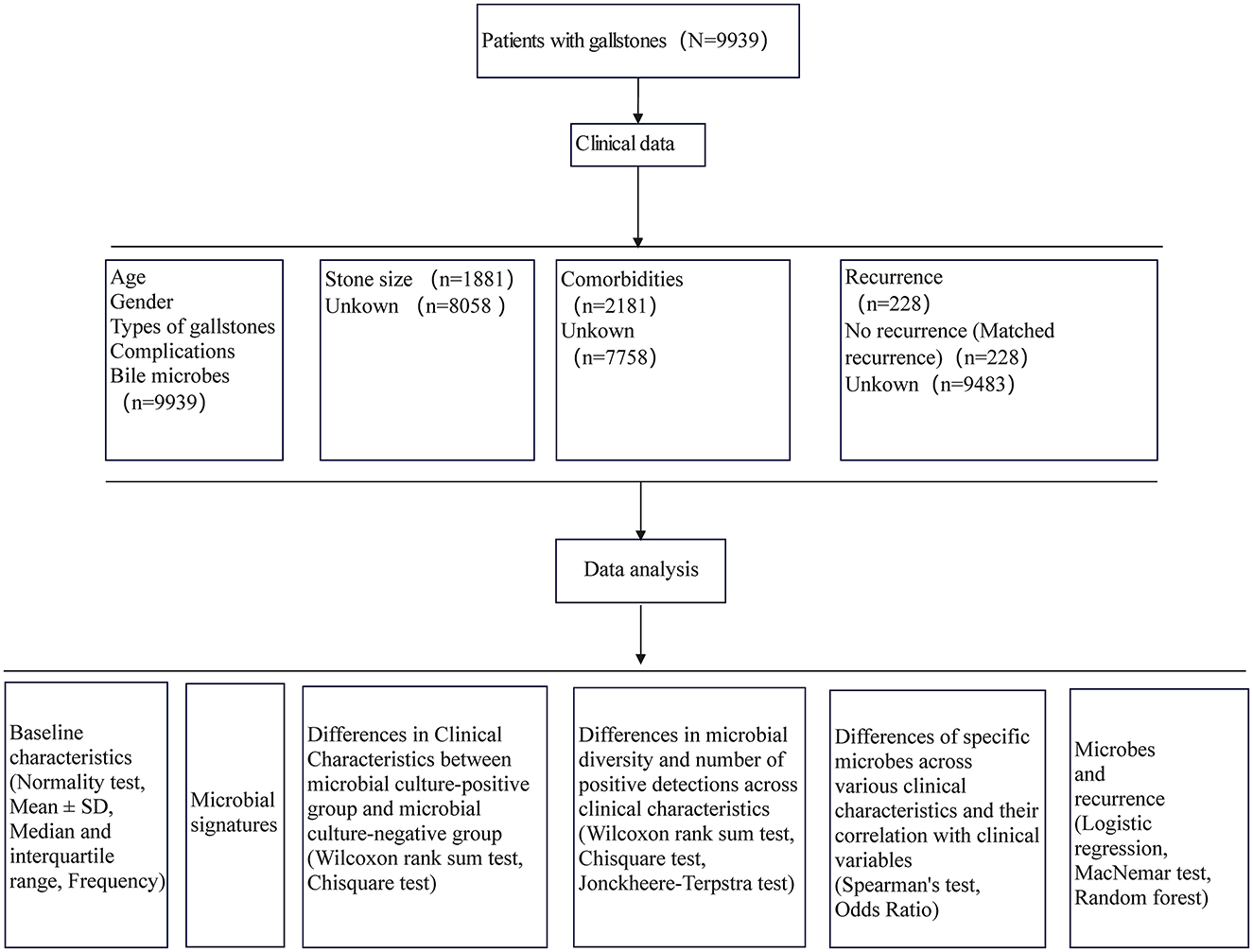
Figure 1. Study design.
2.2 Clinical definitions 2.2.1 Gallstone typeGallstones were classified based on their location into extrahepatic bile duct stones (EBD), hepatolithiasis bile duct stones (HBD), and cholecystolithiasis.
2.2.2 ComplicationsIn this study, complications refer to cholecystitis, cholangitis, and pancreatitis in gallstone patients.
2.2.3 RecurrenceTo avoid the impact of postoperative residual stones on recurrence, recurrence was defined as re-hospitalization and re-diagnosis of gallstones confirmed by imaging with no residual stones and more than 6 months after the initial surgery (von Schönfels et al., 2013). Recurrence patients were matched by gender and age with non-recurrence patients who had not been re-hospitalized for more than 2 years after surgery and were confirmed to have no recurrence through follow-up. All hospital admissions within 30 days were considered the same admission, while entries exceeding 30 days were defined as re-admissions (Shabanzadeh et al., 2019).
2.2.4 ComorbiditiesComorbidities included hypertension, respiratory diseases, coronary heart disease, diabetes, renal cyst, cerebral infarction, fatty liver, venous thrombosis, gallbladder adenomyomatosis, gallbladder polyp, malignant tumor, and cirrhosis of the liver. The selection criterion was based on the top 12 most frequent comorbidities.
2.2.5 Respiratory diseasesIn this study, respiratory diseases included bronchitis, bronchiectasis, bronchial cyst, bronchial fistula, bronchial asthma, bronchial obstruction, solitary pulmonary nodule, emphysema, pneumonia, tuberculosis, atelectasis, pulmonary hypertension, chronic obstructive pulmonary disease, pulmonary fibrosis, pulmonary bullae, hamartoma, pulmonary embolism, interstitial lung disease, hilar lymphadenopathy, pulmonary edema, lung consolidation, polycystic lung, and pulmonary cavity.
2.2.6 Malignant tumorsMalignant tumors in this study included thyroid malignancies, esophageal malignancies, gastric cardia malignancies, lung malignancies, breast malignancies, gastric malignancies, secondary peritoneal malignancies, secondary abdominal wall skin malignancies, secondary abdominal cavity malignancies, secondary abdominal lymph node malignancies, secondary mediastinal malignancies, secondary spinal malignancies, endometrial malignancies, liver malignancies, bile duct malignancies, gallbladder malignancies, bladder malignancies, pancreatic malignancies, colon malignancies, rectal malignancies, small intestine malignancies, duodenal malignancies, kidney malignancies, ureteral malignancies, secondary lymph node malignancies, secondary bone malignancies, prostate malignancies, cervical malignancies, and ovarian malignancies.
2.2.7 Gallstone sizeGallstone size information was obtained for 1,891 participants, retaining only the longest diameter of the largest stone to represent stone size.
2.3 Microbial culturesBile samples were inoculated onto Columbia blood agar and MacConkey agar under sterile conditions for isolation and culture. Pathogens were purified and identified using an automated microbiology analyzer (VITEK2-COMPACT, BioMerieux, France). Quality control strains included Klebsiella oxytoca ATCC 700324 and Enterococcus casseliflavus ATCC 700327.
2.4 Statistical analysisIn descriptive statistics, normally distributed continuous variables are presented as mean ± SD, while non-normally distributed continuous variables are reported as median with interquartile range (IQR). Categorical variables are reported as percentages. Comparison of non-normally distributed continuous variables between two categorical variable groups was conducted using the Wilcoxon rank sum test. For comparison of categorical variables between two categorical variable groups, the Chi-square test was utilized. Analysis of differences in categorical variables among ordered categorical variable groups was performed using the Chi-square test, followed by post-hoc multiple comparisons if significant, and trends were analyzed using the Cochran-Armitage Trend Test. The Jonckheere-Terpstra test was used to compare non-normally distributed continuous variables among ordered categorical variable groups, followed by post-hoc multiple comparisons if differences were detected. Correlation analysis between ordered categorical variables or continuous variables and continuous variables was conducted using Spearman's correlation coefficient. Odds ratios (OR) were used to analyze the relationship between two categorical variables. The MacNemar test was employed to compare differences in the frequency of positive microbes between patients before and after recurrence. In the analysis of factors influencing recurrence, missing data for comorbidity and gallstone size information were imputed using the random forest model-based imputation method implemented in R's missForest package (Stekhoven and Bühlmann, 2012), with out-of-bag error rates from random forest used to report imputation results for complications and maximum gallstone diameter information. Logistic regression analysis was performed to evaluate factors influencing recurrence. Multivariate binary logistic regression analysis was conducted for variables that showed statistical significance in univariate analyses. All statistical tests were two-sided, and a P-value below 0.05 was considered statistically significant. Statistical analyses were performed using SPSS® Statistics version 22 (IBM, Armonk, NY, USA) and R version 4.3.2.
3 Results 3.1 Baseline characteristicsBaseline characteristics of various clinical conditions are summarized in Table 1. Among 9,939 patients, females (5,299, 53.30%) were significantly more prevalent than males (4,640, 46.70%) (P < 0.001). The age distribution showed the highest proportion in the 60–74 age group (3,420, 34.41%), while the < 45 age group had the lowest proportion (1,488, 14.97%). Gallstone types were predominantly cholecystolithiasis (52.21%), followed by only EBD stones (40.17%). Patients without complications (6,731, 67.72%) was higher than those with complications (3,208, 32.28%). Maximum gallstone diameter, representing stone size, was available for 1,881 individuals, ranging from 2 to 60 mm, with 1,737 (92.34%) having sizes ≤ 20 mm. The most frequent sizes were 6 mm (247, 13.13%) and 10 mm (247, 13.13%) (Supplementary Figure S1A). Complications data were available for 2,181 patients, all of whom had at least one complication, with the highest proportion having one complication (878, 40.26%). As the number of complications increased, the number of patients decreased (Supplementary Figure S1B). Analysis of combinations of all patients' complication types revealed 317 unique combinations (Supplementary Table S3), with the top 10 combinations based on patient count, where only respiratory system diseases were most common (203, 9.31%), followed by hypertension alone (175, 8.02%) (Supplementary Figure S1C). Regarding recurrence, only 228 patients (2.30%) returned for diagnosis of recurrent gallstones, though this does not represent the recurrence rate as some recurrent patients may have sought treatment elsewhere without follow-up, categorized as “Unknown”. Subsequently, matching by age and gender was performed from the “Unknown” group to classify patients who did not recur as “No recurrent”. Among recurrent patients, recurrence occurred between 181 and 2,287 days, with a median of 616.00 days.
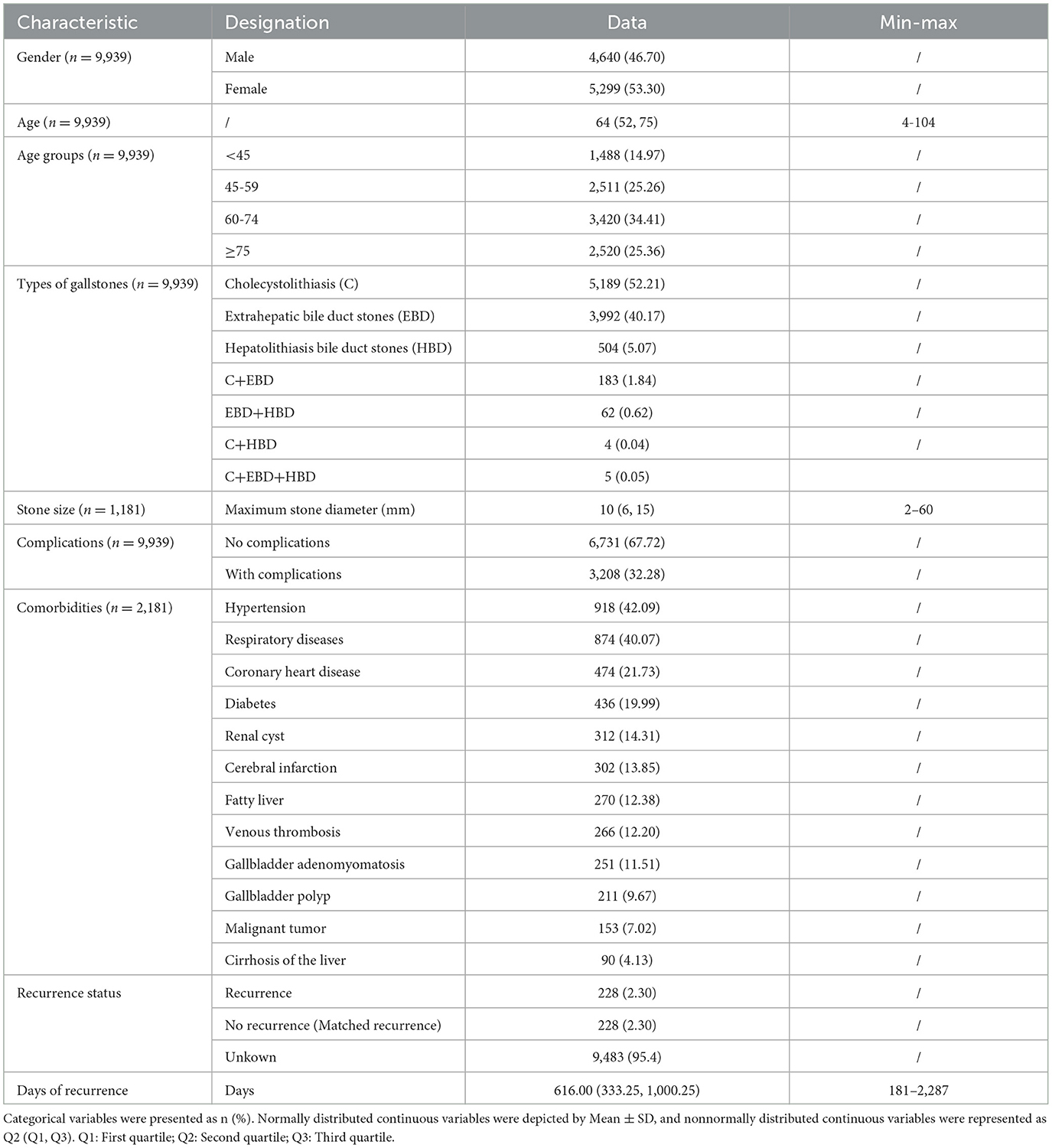
Table 1. Demographic and clinical characteristics.
3.2 Bile microbial characteristics in gallstone patientsIn this study, 76 types of microbes were cultured from 5,153 (51.85%) patients, while no microbes were cultured from 4,786 (48.15%) patients (Supplementary Table S1). These 76 microbes included five fungi (Candida parapsilosis, Candida tropicalis, Cyberlindnera jadinii, Meyerozyma guilliermondii, Pichia kudriavzevii) and 71 bacteria, spanning three phyla (p__Ascomycota, p__Firmicutes, p__Proteobacteria), five classes (c__Alphaproteobacteria, c__Bacilli, c__Betaproteobacteria, c__Gammaproteobacteria, c__Saccharomycetes), 13 orders, 19 families, and 31 genera (Figure 2).
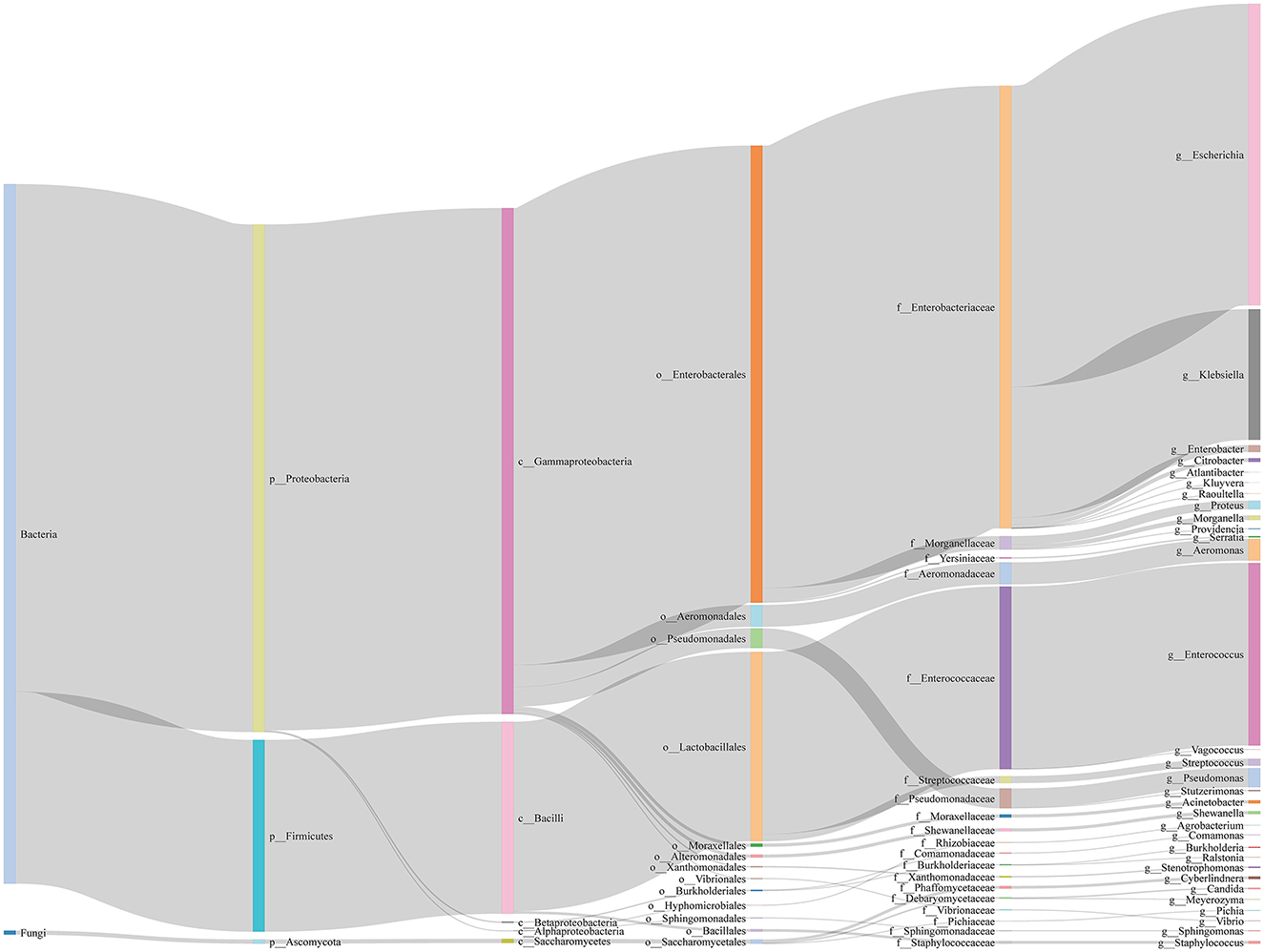
Figure 2. Sankey diagram of microbes in bile of all samples. We show the taxonomic ranks kingdom, phylum, class, order, family, genus.
Regarding sample distribution, the number of people containing 1, 2, 3, and 4 species of microbes is 3,403, 1,573, 175, and 2, respectively, which shows that the higher the number of species, the lower the number of people located (Figure 3A). To identify dominant species, we analyzed the number of positive samples for each species, finding that E. coli, Klebsiella pneumoniae, and Enterococcus faecalis had the highest positive detection frequencies, with 3,033, 1,287, and 1,264 occurrences, respectively (Figure 3B).
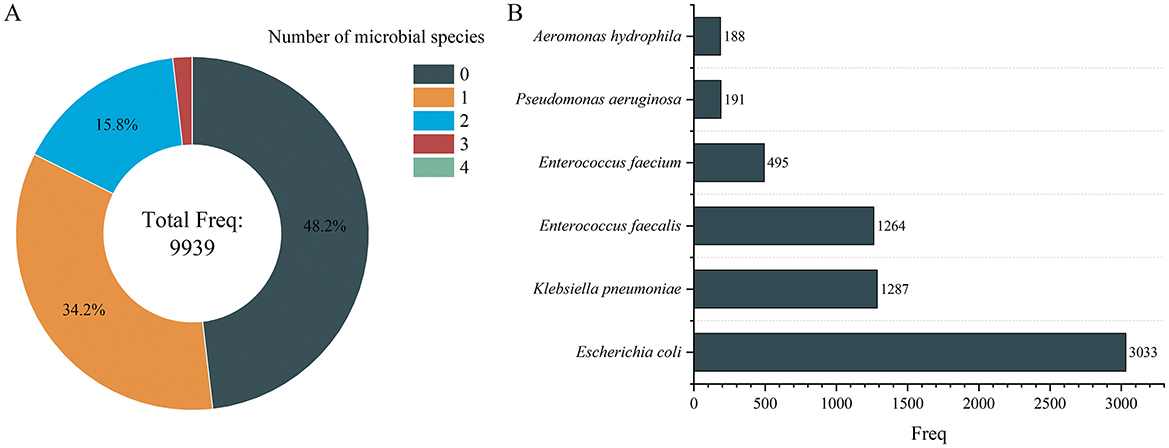
Figure 3. Number of microbial species distribution in gallstone individuals (A) and microbial distribution of dominant species (B). Only the microbes with a frequency >100 individuals are displayed in (B).
3.3 Differences in clinical characteristics between microbial positive and negative groupsWe explored whether there were significant differences in clinical characteristics between the Microbial Positive Group (MP group, n = 4,786) and the Microbial Negative Group (MN group, n = 5,153). The results showed that the MP group had significantly higher age (P < 0.001) and stone size (P = 0.043) compared to the MN group (Figures 4A, B). However, the effect size for stone size was small (r = 0.047), indicating that although the difference is statistically significant, the actual clinical impact of this difference is minimal. The occurrence frequencies of EBD stones (P < 0.001) and HBD stones (P = 0.015) were significantly higher in the MP group than in the MN group, while cholecystolithiasis were more frequent in the MN group (P < 0.001) (Figure 4C). Additionally, the incidence of hypertension was significantly higher in the MP group compared to the MN group (P = 0.034) (Figure 4C).
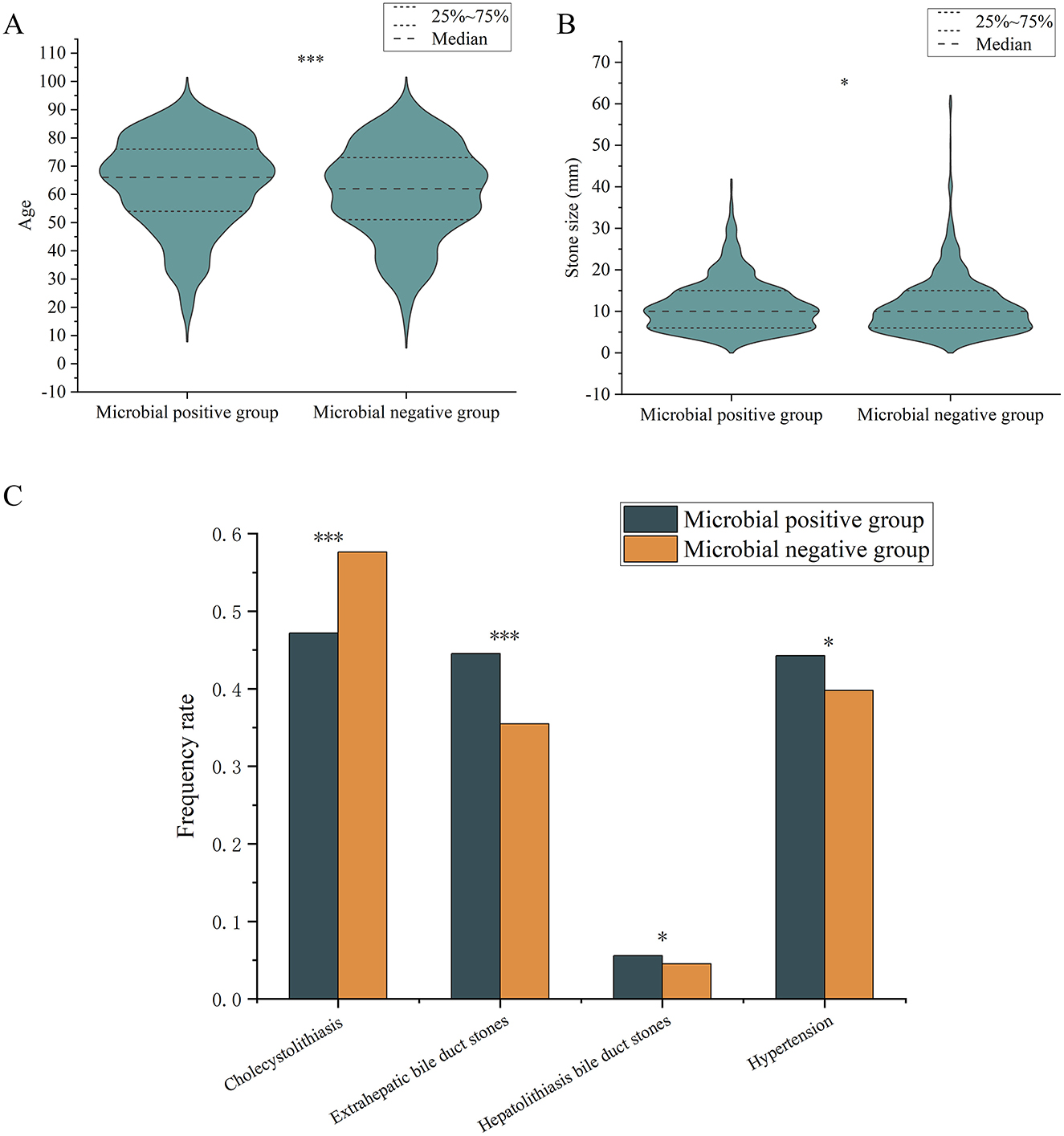
Figure 4. Differences in frequency rate of various variables between microbial positive and negative groups. (A) age; (B) stone sizes; (C) types of gallstones and comorbidities. “*” indicates P < 0.05; “***” indicates P < 0.001. Only comparisons with significant statistical difference (P < 0.05) are shown.
3.4 Differences in microbial diversity and positive detection rates across clinical characteristicsWe further compared microbial diversity and positive microbial detection rates across different clinical characteristics (gender, age, gallstone types, presence of complications, recurrence status). The results indicated significant differences in microbial diversity and positive detection rates among different age groups (P < 0.001), gallstone types (P < 0.001), and recurrence status (P = 0.012; P = 0.002) (Figure 5). Specifically, microbial diversity was significantly higher in the 45–59 age group, patients with HBD stones and mixed stones, and no recurrent group. The positive detection rate was significantly higher in patients aged ≥75, those with EBD stones and HBD stones, and in the recurrent group.
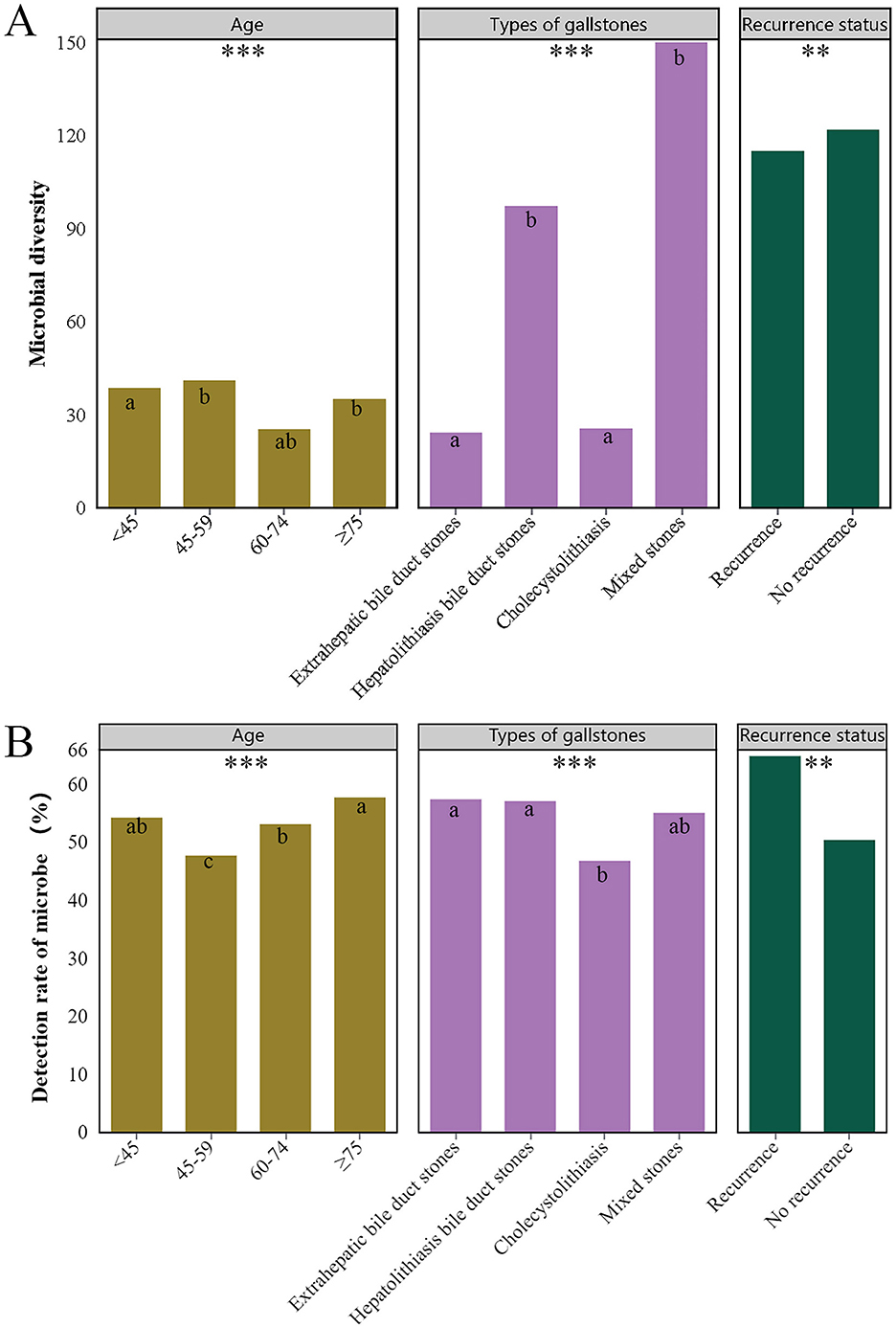
Figure 5. Differences in microbial diversity (A) and detection (B) rates across various clinical characteristics. Only clinical characteristics with significant differences are shown in the figure, namely different age groups, types of gallstones, and recurrence status. Different superscript letters (a, b and c) indicate significant differences. *** indicates P < 0.001, ** indicates P < 0.01.
3.5 Differences in microbial diversity and positive detection rates across clinical characteristicsBased on clinical variables, we categorized the patients into male and female groups, four different age groups, groups with four different gallstone types, groups with or without complications, and recurrence vs. non-recurrence groups, to explore the differences in specific microbes across these classifications. The results showed that Streptococcus sanguinis exhibited a significant difference between males and females (P = 0.036), but its frequency was very low, with only five detections among 5,299 females and none among 4,640 males.
The positive frequencies of E. coli (P < 0.001), Enterococcus faecium (P < 0.001), and K. pneumoniae (P < 0.001) differed significantly among the four groups, and all of them were significantly higher in the ≥75 years age group than in the other three groups (Figure 6A).
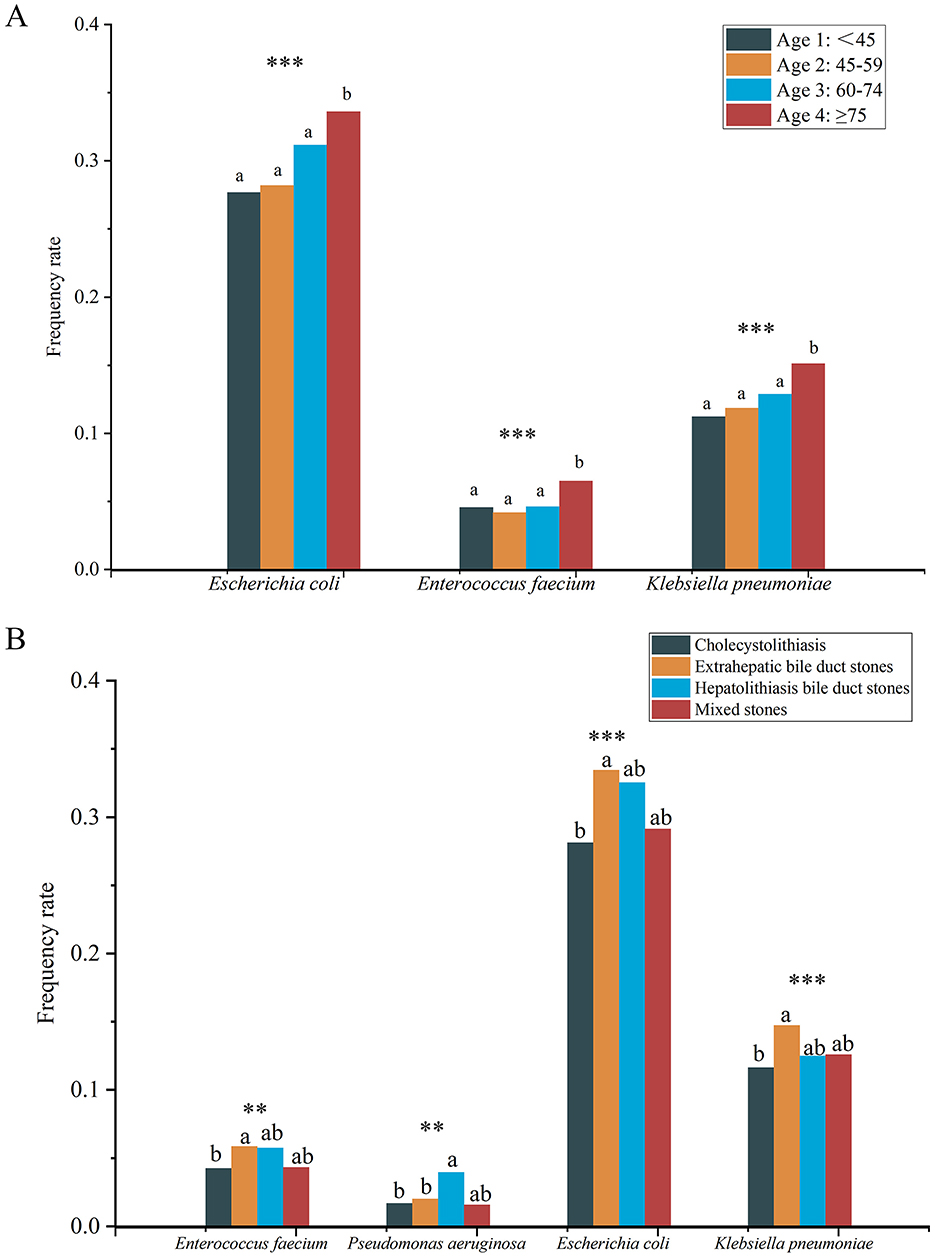
Figure 6. Differences in frequency rate of specific microbes among four different age groups (A) and different types of gallstones (B). Different lowercase superscript letters indicate significant differences among different groups (P < 0.05). *** indicates P < 0.001, ** indicates P < 0.01.
Significant differences were also found in the positive frequencies of E. coli (P < 0.001), K. pneumoniae (P < 0.001), E. faecium (P = 0.004), and Pseudomonas aeruginosa (P = 0.004) among different gallstone types (Figure 6B). Specifically, the positive frequencies of E. faecium, E. coli, and K. pneumoniae were significantly higher in the EBD group compared to the cholecystolithiasis group, while P. aeruginosa had a significantly higher positive frequency in the HBD group compared to the EBD and cholecystolithiasis groups. It is noteworthy that no significant differences were found in the frequencies of any microbes between the groups with or without complications, and between the recurrence and no recurrence groups.
To further explore the association between microbes and various clinical variables, we performed odds ratio (OR) analysis. The results indicated that 15 microbes were significantly associated with clinical variables (Supplementary Figure S2). While the data analysis revealed meaningful correlations, it is important to note that the frequencies of these microbes were relatively low in the total sample (2–26 occurrences), which might introduce random effects and potentially affect the robustness and generalizability of our findings.
3.6 Microbes and recurrenceThe aforementioned analysis found that microbial diversity was significantly reduced in the recurrence group compared to the no recurrence group. However, no significant differences in the frequencies of specific microbes were observed between these two groups, and there was no significant difference in recurrence rates between the MN and MP groups.
To further investigate the relationship between the number of microbial species and recurrence, we divided the patients into no microbe group, single microbe group, and multiple microbe group (2 or 3 microbial species) and compared the differences in recurrence frequencies among these groups. The results showed that the recurrence rate in the single microbe group was significantly higher than in the other two groups (P < 0.001) (Figure 7A).
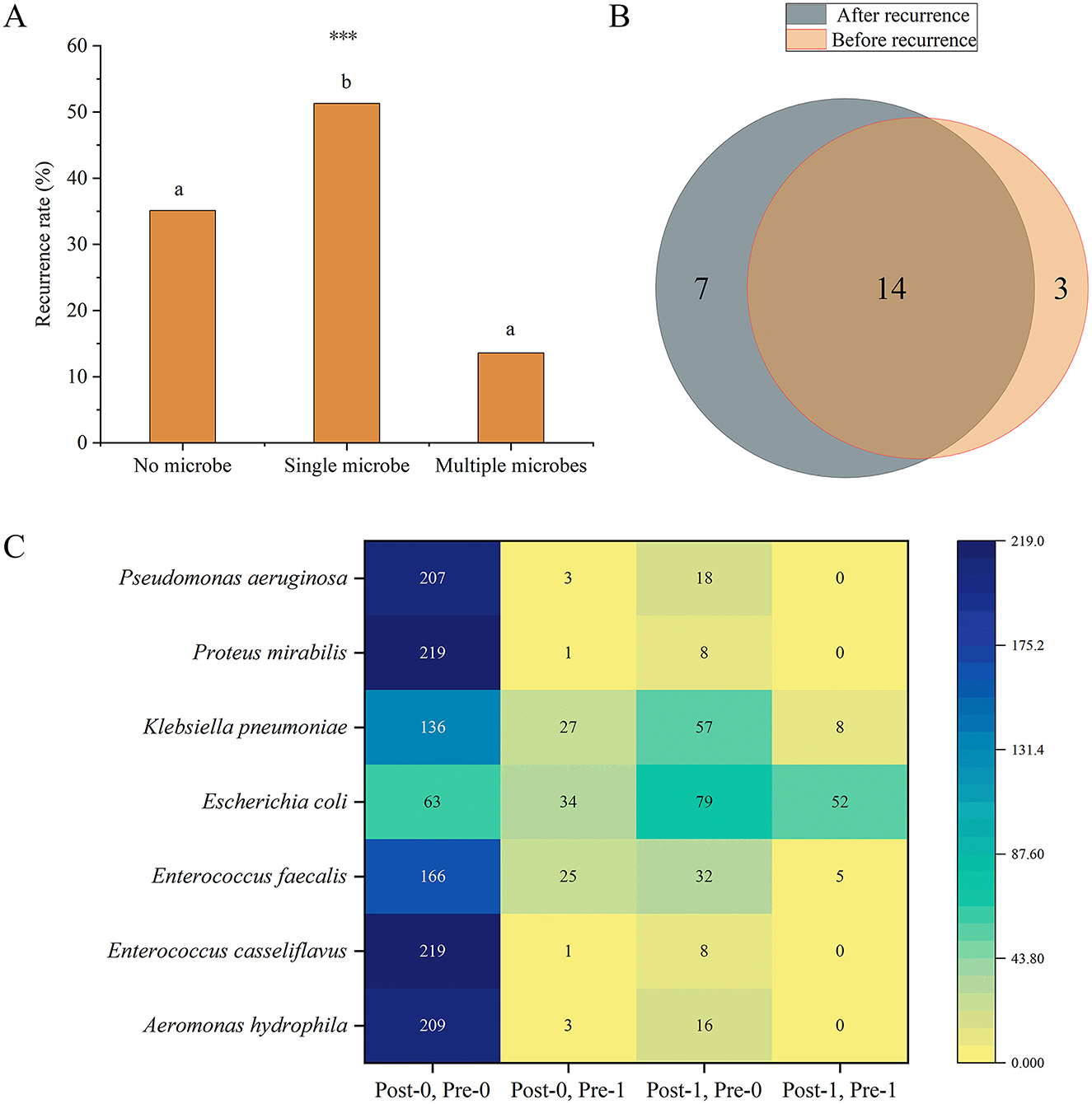
Figure 7. (A) Differences in recurrence frequencies among the groups with no, single, and multiple microbes' groups. Different lowercase superscript letters indicate significant differences among different groups (P < 0.05). *** indicates P < 0.001. (B) Venn diagram of the number of microbial species present before and after recurrence. (C) Distribution of the frequencies of microbes with significant differences before and after recurrence. The heatmap shows the distribution of frequencies for seven microbes under different conditions before (Pre) and after (Post) recurrence. The vertical axis lists the microbial species, while the horizontal axis represents different condition combinations. Post-0, Pre-0 indicates the number of patients who were negative for the microorganism both before and after recurrence; Post-0, Pre-1 indicates the number of patients who were positive before recurrence and negative after recurrence; Post-1, Pre-0 indicates the number of patients who were negative before recurrence and positive after recurrence; Post-1, Pre-1 indicates the number of patients who were positive both before and after recurrence. Numerical labels indicate specific frequency counts, and the shading of the color represents the magnitude of the counts, with darker colors indicating higher frequencies.
Moreover, we further analyzed the changes in microbes before and after recurrence in patients with recurrence. Among the 228 recurrence patients, 17 microbes were detected before recurrence, and 21 microbes were detected after recurrence. 14 microbes were common to both before and after recurrence (Figure 7B). We primarily focused on microbes whose frequencies showed significant changes before and after recurrence. The results revealed that the frequencies of seven microbes (Aeromonas hydrophila, P = 0.004; E. casseliflavus, P = 0.039; E. faecium, P = 0.013; E. coli, P < 0.001; K. pneumoniae, P = 0.002; Proteus mirabilis, P = 0.039; P. aeruginosa, P = 0.001) were significantly different before and after recurrence, and all of these microbes were detected in more patients after recurrence (Figure 7C).
To identify factors influencing recurrence, we conducted univariate and multivariate regression analyses. Univariate regression analysis (including all clinical variables and 76 microbes) initially screened the factors affecting recurrence (Supplementary Table S4). Using these variables, along with sex and age as basic variables, we further performed multivariate binary logistic regression analysis (Supplementary Table S5). The results indicated that age (OR, 0.97; 95% CI, 0.95–0.99, P = 0.001), stone size (OR, 1.06; 95% CI, 1.03–1.08, P < 0.001), diabetes (OR, 2.45; 95% CI, 1.51–3.96, P < 0.001), venous thrombosis (OR, 2.94; 95% CI, 1.56–5.51, P = 0.001), cirrhosis of the liver (OR, 5.71; 95% CI, 1.99–16.34, P = 0.001), malignant tumors (OR, 3.26; 95% CI, 1.51–7.07, P = 0.003), coronary heart disease (OR, 5.71; 95% CI, 1.99–16.34, P = 0.014), and the microbial species (OR, 2.89; 95% CI, 1.77–4.71, P < 0.001) were significant predictors of recurrence (Supplementary Table S5, Figure 8A). We further used these variables to construct a random forest model. The MeanDecreaseGini and MeanDecreaseAccuracy provided by the random forest model were used to indicate the importance of variables within the model (Figure 8B). The results showed that stone size contributed the most to model accuracy and purity. The model's accuracy, precision, recall, F1 score, and ROC-AUC values (Figure 8C) were 0.801, 0.721, 0.860, 0.784, and 0.862, respectively, indicating that the model is an excellent predictive tool with good performance and high predictive power in forecasting recurrence.
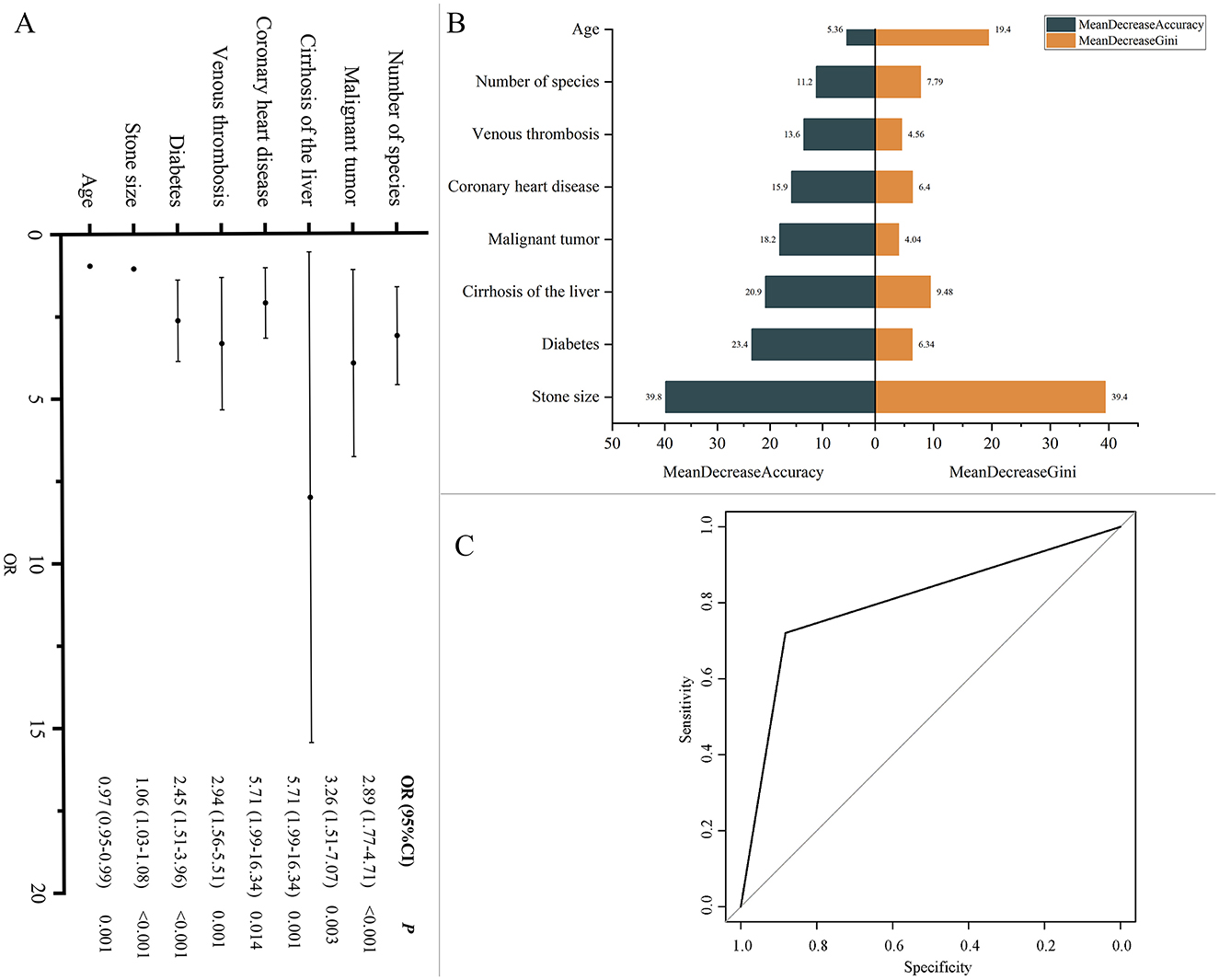
Figure 8. (A) Factors influencing recurrence. Multivariate binary logistic regression analysis was conducted to calculate odds ratios (ORs) and 95% confidence intervals (CI), assessing factors associated with recurrence. (B) Model variable importance based on MeanDecreaseGini and MeanDecreaseAccuracy. (C) ROC Curve for recurrence prediction model. ROC curve illustrating the performance of the model in terms of sensitivity and specificity.
4 DiscussionThis study analyzed the clinical characteristics and bile microbiology of 9,939 patients with gallstones. The results showed that there were significantly more females than males in the study population, and the age distribution was mainly between 60 and 74 years. Gallbladder stones were the most common type, accounting for over half of the cases. Microbial cultures were positive in 5,153 patients (51.85%), yielding 76 microbes (5 fungi and 71 bacteria). We further analyzed the data from various perspectives, including differences in clinical characteristics between MP and MN groups, variations in microbial diversity and positivity rates across different clinical characteristics, differences in specific microbes with varying clinical features and their correlation with clinical variables, and the relationship between microbes and recurrence. These analyses revealed several important clinical and microbial features, providing a foundation for further exploration of recurrence mechanisms and clinical management.
Among the 9,939 gallstone patients, females significantly outnumbered males, and the majority of patients were in the 60–74 age group. A recent nationwide study on the age, gender, geographic, and clinical differences in gallstone disease in China found that, regardless of anatomical location, the prevalence of gallstones significantly increases with age (P < 0.001), with the age-standardized prevalence higher in females than in males (5.41% vs. 4.85%, P < 0.001) (Song et al., 2022). Another study reported that the prevalence of gallstone disease increases with age, with male and female prevalence rates of 7.1% and 10.4%, respectively (Zhang et al., 2022). Our findings are consistent with previous studies, indicating that gallstones are more common in the elderly, with a higher prevalence in females. Regarding gallstone types, gallbladder stones were the most prevalent, reflecting their common occurrence in clinical practice.
Bile in healthy individuals is typically sterile; however, under certain conditions, such as bile duct obstruction, bacteria can proliferate in the stagnant bile. Earlier hypotheses suggested that different bacterial species might increase the formation of gallstones and biliary diseases through specific enzyme activities or biofilm production; several studies have proposed their association with bacterial infections (Kosowski et al., 1987; Lazcano-Ponce et al., 2001; Sattar et al., 2007). However, the exact mechanism of this phenomenon remains unclear (Hoogerwerf and Soloway, 1999; Vitetta et al., 2000). The role of bacteria in biliary disease formation is primarily considered in relation to cholelithiasis, which accounts for 90% of global cholelithiasis cases (Gomes et al., 2009). The involvement of bacteria in the formation of biliary stones is still debated. The formation of gallstones is attributed to bacteria originating from the intestine that ascend to the bile ducts due to various predisposing conditions (Englesbe and Dawes, 2005). Escherichia coli and other gut bacteria, such as Enterococcus spp., are the most common bacteria in these infections. These bacteria can adhere to and colonize the biliary epithelium using the same surface proteins known as adhesins (Ljungh and Wadström, 2002). Factors such as bacterial mucus, antibiotic resistance in bile, and biofilm formation by bacteria are considered crucial in gallstone formation. Long-term exposure to bile salts is known to induce biofilm formation in enteric pathogens from the Enterobacteriaceae family, such as Salmonella and Shigella spp., as well as emerging pathogens like E. coli, K. pneumoniae, Enterococcus spp., and Clostridium spp. (Tsuchiya et al., 2018). Furthermore, biofilm formation and anaerobic energy metabolism are considered potential microbial mechanisms involved in gallstone formation. The bacterial composition of the stones and identified enteric bacteria, such as Enterobacter spp., Enterococcus spp., Escherichia spp., Klebsiella spp., and Salmonella spp., are contributors to gallstone formation (Ballal et al., 2001; Sattar et al., 2007; Gomes et al., 2009; Joo and Otto, 2012). In our study, microbial cultures were positive in 5,153 patients (51.85%), with E. coli, K. pneumoniae, and E. faecalis being the most common microbes. This finding aligns with other studies identifying common pathogens associated with gallstone-related infections (Ballal et al., 2001; Sattar et al., 2007; Gomes et al., 2009; Lévay et al., 2013; Tajeddin et al., 2016; Pagani et al., 2023). E. coli is a common human pathogen, a Gram-negative, facultative anaerobic rod from the Enterobacteriaceae family, capable of causing various infections in different anatomical sites and invading the bile ducts during cholestasis, contributing to gallstone formation (Tajeddin et al., 2016; Blesl and Stadlbauer, 2021). K. pneumoniae was first reported in Taiwan in 1980 and gradually became the leading pathogen of pyogenic liver abscess (PLA) in Asia, commonly found in East Asian populations, often associated with diabetes and gallstones (Serraino et al., 2018; David et al., 2021). E. faecalis is a Gram-positive bacterium found in the gastrointestinal tracts of humans and animals, classified as a facultative anaerobe, with dual metabolic lifespans that enhance its robustness and stress resistance, and is associated with human infections, particularly in immunocompromised individuals, causing diseases such as endocarditis, meningitis, pneumonia, peritonitis, visceral abscesses, urinary tract infections, and sepsis (Boeder et al., 2024). Studies have shown that E. faecalis is abundant in patients with chronic hepatobiliary diseases and may induce hepatic tumorigenesis (Xie et al., 2016; American Association for Cancer Research, 2021; Große et al., 2021; Iida et al., 2021; Awoniyi et al., 2023).
This study is the first to compare the clinical characteristics of bile MP and MN groups in patients with gallstones. It was found that patients in the MP group had significantly higher age, and incidence of hypertension compared to the MN group, indicating that the presence of microbes may be associated with more severe conditions. In addition, the frequency of bile duct stones was significantly higher in the MP group than in the MN group whereas the opposite was true for cholecystolithiasis (P < 0.001), suggesting that microbes play different roles in the formation and development of stones at different sites (Lee et al., 2023), and that the high frequency of bile duct stones may be related to the complex anatomy of the biliary system and its greater susceptibility to microbial infection. In contrast, the formation of cholecystolithiasis may be more influenced by the environment of the gallbladder itself.
Microbial diversity was particularly enriched in the 45–59 age group, as well as among patients with HBD and mixed stones. The relatively stable immune system activity and biliary microenvironment in patients aged 45–59 may support a diverse microbial community, potentially reducing pathogen colonization and infection. The complex structure of intrahepatic bile ducts provides various ecological niches for the coexistence of multiple microbes, while mixed stones may reflect the interaction between the gallbladder and bile ducts, promoting microbial diversity (Feng et al., 2022). The positive detection rate of microbes was significantly higher in patients aged ≥75, and those with EBD and HBD stones. The increased positive detection rate in elderly patients (≥75 years) may be due to immune system decline and a higher likelihood of chronic diseases, which heighten infection risk (Lee et al., 2023). The high microbial positivity rate in bile duct stones might be linked to the complex microenvironment within the bile ducts and their susceptibility to infections, making them a favorable habitat for microbes.
We further analyzed the differences in specific microbes across various clinical characteristics and their correlations with clinical variables. The results showed that the positive frequencies of E. coli, E. faecium, and K. pneumoniae were significantly higher in the ≥75 age group compared to other age groups, which may be related to the declining immune function in elderly patients. The adaptability and antibiotic resistance of E. coli within the biliary tract make it more likely to proliferate in older patients; meanwhile, E. faecium is known for its antibiotic resistance and is commonly associated with nosocomial infections (Boeder et al., 2024). The increased risk of infection in elderly patients may be further exacerbated by frequent hospitalizations and the use of broad-spectrum antibiotics. K. pneumoniae is associated with a variety of infections, including pneumonia, urinary tract infections, and biliary infections (Xie et al., 2016; American Association for Cancer Research, 2021; Große et al., 2021; Awoniyi et al., 2023; Boeder et al., 2024), and its high positive frequency in elderly patients is particularly notable, possibly due to the higher rates of hospitalization and invasive procedures (e.g., catheterization and biliary stenting) in this population, which increase the risk of infection. These findings highlight the importance of heightened vigilance in the prevention and management of biliary infections in elderly patients. In different types of gallstones, the positive frequencies of E. faecium, E. coli, and K. pneumoniae were significantly higher in the EBD group compared to the cholecystolithiasis group, which may be attributed to the open structure of the extrahepatic bile ducts, increasing the risk of infection. In the HBD group, the positive frequency of P. aeruginosa was significantly higher than in the EBD and cholecystolithiasis groups, potentially due to its adaptability to the complex bile duct structure and liver environment, as well as its high antibiotic resistance. Studies have shown that 30% of cholesterol gallstones can be cultured for strains that secrete β-glucuronidase and phospholipase A2, with P. aeruginosa exhibiting the highest β-glucuronidase activity, which may be a key factor in cholesterol gallstone formation (Peng et al., 2015). Additionally, the results of the culture method revealed that biofilm-forming bacteria (P. aeruginosa, E. coli, K. pneumoniae, Enterococcus spp., and Acinetobacter spp.) coexist in various combinations and are the main bacteria associated with cholelithiasis (Tajeddin et al., 2016; Pagani et al., 2023). These organisms can form robust biofilms, enhancing colonization and antibiotic resistance, which presents challenges in treatment. This suggests the need for increased monitoring and targeted therapy against these species, particularly in elderly patients with compromised immune function and those with bile duct stones. Furthermore, our study explored the associations between microbes and various clinical variables using OR analysis. Although we identified significant associations between 15 microbes and specific clinical variables in a sample of 9,939 cases, it is important to note that the detection frequency of each microbe was relatively low. We believe that the current findings may be influenced by chance and bias, limiting the value of further analysis and discussion. Therefore, we do not recommend an in-depth exploration of these associations based on the existing data. Instead, future research should focus on microbes with greater clinical significance and higher detection frequencies.
Gallstone disease recurrence is a common and serious issue. Existing studies indicate that patients with recurrent gallstones often have poorer clinical outcomes, which is often accompanied by a higher complication rate and a more frequent need for surgical intervention, especially an increase in the incidence of gangrenous cholecystitis during the COVID-19 pandemic (De Simone et al., 2022). In this study, microbial diversity was found to be lower in the recurrence group compared to the no recurrence group. The rich microbial community in the non-recurrent group may fight against pathogenic bacteria through mechanisms such as competitive inhibition and production of antimicrobial substances, preventing the overgrowth of pathogenic bacteria and the re-formation of stones and reducing the risk of recurrence (Lee et al., 2023). Our findings are consistent with previous reports. In the study by Choe et al., which examined the microbial characteristics and bile composition of patients with recurrent common bile duct (CBD) stones after endoscopic treatment using 16S rRNA sequencing, the microbial richness was significantly lower in the recurrence group, and microbial evenness was also reduced. Differences in the overall microbial community were observed between the recurrence and non-recurrence groups (Choe et al., 2021). Additionally, another study based on 16S rDNA gene sequencing also demonstrated a significant reduction in biliary microbial diversity in patients with recurrent CBD stones (Tan et al., 2022). These findings further support the critical role of microbial diversity in the recurrence of gallstone disease. In our study, the number of patients with positive microbial cultures was significantly higher in the recurrence group, which may be related to persistent infections and residual microbes. Patients with recurrent gallstones may experience ongoing biliary infections, or residual microbes from an initial infection that was not fully eradicated, thereby increasing the risk of stone recurrence. Further analysis revealed that the recurrence rate in singe microbe group was significantly higher than in groups of no microbe and multiple microbes. This suggests that the presence of a single pathogen may increase the risk of gallstone recurrence by influencing biofilm formation and inducing persistent inflammation. In contrast, the coexistence of multiple microbes may reduce the risk of recurrence by promoting microbial competition and ecological balance, which can inhibit the overgrowth of certain pathogenic bacteria. The lower recurrence rate in the no microbe group may be due to a reduced inflammatory response and biofilm formation, processes that are closely associated with stone formation and recurrence. In summary, these results indicate that microbial diversity plays a key role in the recurrence of gallstone disease, offering new insights into the prevention and treatment of gallstone recurrence.
Seven microbes (A. hydrophila, E. casseliflavus, E. faecium, E. coli, K. pneumoniae, P. mirabilis, P. aeruginosa) showed significant frequency differences before and after recurrence, and all seven were present in more patients after recurrence, suggesting they may play a crucial role in gallstone recurrence. Changes in microbial frequency before and after recurrence may reflect dysbiosis or suboptimal antimicrobial treatment during the patient's course of therapy. As previously mentioned, Enterococcus faecium, E. coli, and K. pneumoniae are dominant microbial species in the bile of gallstone patients, and their frequencies differed significantly before and after recurrence. The high adaptability and persistence of E. coli and K. pneumoniae in the biliary tract may promote cholesterol crystal formation, exacerbating stone recurrence. Additionally, their ability to form biofilms increases the difficulty of clearing infections. E. casseliflavus and E. faecium are common enterococci with pathogenicity and antibiotic resistance (Narciso-Schiavon et al., 2015; Britt and Potter, 2016). E. casseliflavus has a high affinity for the biliary system and is prone to causing biliary and liver infections (Yoshino, 2023). E. faecium exhibits resistance to multiple antibiotics, including vancomycin and oxazolidinone (Boeder et al., 2024), which may increase the difficulty of infection control in the recurrence group. In 2021, an E. faecium strain carrying an oxazolidinone resistance gene was isolated from the bile of a common bile duct stone patient in Shenzhen, China, highlighting the complexity and resistance of this pathogen within the biliary system (Deng et al., 2023). The high pathogenicity and antibiotic resistance of these bacteria may exacerbate biliary inflammation, promoting the formation and recurrence of gallstones, particularly as E. faecium's resistance complicates the eradication of infections in recurrent patients. A. hydrophila is an emerging pathogen found widely in aquatic environments and has been reported to cause various severe infections, such as gastroenteritis, skin infections, peritonitis, bacteremia, meningitis, and necrotizing fasciitis (Citterio and Francesca, 2015). In one case report, a 72-year-old female patient with gallstones and hypertension died from necrotizing fasciitis caused by A. hydrophila following laparoscopic cholecystectomy (Janjua et al., 2024). Another case involved a 72-year-old elderly patient with gallstones and rheumatoid arthritis on immunosuppressive therapy (tocilizumab) who developed septicemia and acute suppurative cholangitis due to A. hydrophila (Okumura et al., 2011). These cases emphasize the high pathogenicity of A. hydrophila in postoperative infections and its severe impact on prognosis. Its broad virulence factors may trigger or exacerbate biliary inflammation in gallstone patients, thereby promoting stone recurrence. P. mirabilis is known for its ability to produce urease, which breaks down urea to produce ammonia, alkalinizing the local environment and facilitating stone formation (Armbruster and Mobley, 2012; Norsworthy and Pearson, 2017). Its role in gallstone recurrence may be similar, promoting recurrence by altering the local environment. Pseudomonas aeruginosa, as a highly resistant pathogen capable of forming biofilms, has been widely recognized for its role in biliary infections and gallstone formation (Peng et al., 2015; Tajeddin et al., 2016; Pagani et al., 2023). The increase in this bacterium after gallstone recurrence may be related to changes in the biliary environ
留言 (0)