
記住我


There were 656 consecutive patients who underwent first HCT between 2016 and 2021 for AML in CR, CRi, or MLFS at City of Hope. Of these, 312 had pre-HCT marrow evaluated for MFC-MRD performed at University of Washington and received FluMel or MAC regimen. Patient demographics and transplant characteristics are summarized in Table 1. Briefly, of the 312 patients with available data, 44 (14.1%) had MFC-MRD+ disease on pre-transplant bone marrow assessment. Most patients were in first remission in the entire cohort (84.3%) as well as among MRD+ patients (70.5%). The median age was 61 years old (range: 22–82) in the MRD+ group compared to 56 (19–79) in the MRD- group (p = 0.065). Of MRD+ patients, those who received FluMel had a median age of 68 (29–82), compared to 50 (22–73] in the MAC group. Upon stratification of patients for ELN risk, more patients in the adverse risk group had MRD+ prior to transplant (19.7%, n = 26/132), compared to intermediate (9.8%, n = 13/132) and favorable risk (10%, n = 5/50) (p = 0.052).
Transplant outcomesAt the median follow-up of 26.3 months (range:4.4–74) for surviving patients, the estimated 24-month OS, LFS and CIR in those with MFC-MRD+ were 47.7% (95% confidence interval [CI], 32.5–61.5), 40.9% (95% CI, 26.5–54.8), and 38.6% (95% CI, 24.2–52.8); and those with MFC-MRD- were 78.0% (95% CI, 72.5–82.5), 73.9% (95% CI, 68.2–78.7), and 14.6% (95% CI, 10.6–19.1). On multivariate analysis, MFC-MRD+ was independently predictive of worse OS and LFS with hazard ratio (HR) of 2.80 (95% CI, 1.8–4.34; p = <0.001) and 2.92 (95 CI, 1.95–4.42; p ≤ 0.001), respectively (Table 2). MFC-MRD+ was also associated with higher CIR, HR = 3.13 (95% CI, 1.86–5.26; p ≤ 0.001). MFC-MRD+ status was not predictive of non-relapse mortality (NRM) or acute GVHD outcomes. Interestingly, MRD+ was associated with reduced incidence of chronic GVHD (HR = 0.57, 95%CI 0.35–0.93, p = 0.028) on univariate analysis.
Table 2 Multivariate analysis of transplant outcomes.We examined MRD by other methods including PCR, NGS, or FISH/cytogenetics; 21 of 44 patients with MFC-MRD+ were also MRD+ by an additional method. There were 23 patients with positive MFC-MRD while MRD negative by other methods. There was no difference in LFS or CIR in patients who tested positive by one or more methods (data not shown).
By multivariate analysis, other variables associated with transplant outcomes were; age (≤59 vs ≥60) for OS (HR = 1.64, 95% CI, 1.09–2.49, P = −0.031); and KPS (90–100 vs. <90) for OS (HR = 1.63, 95% CI, 1.10–2.42, p = 0.013), LFS (HR = 1.66, 95% CI, 1.15–2.39, p = 0.006) and CIR (HR = 1.84, 95% CI, 1.13–3.0, p = 0.016); conditioning (MAC vs. RIC) for OS (HR = 1.48, 95% CI, 1.00–2.21, p = 0.049) but not LFS, CIR, or NRM; remission status (CR1 vs CR2+) for LFS (HR = 1.87, 95% CI, 1.23–2.84, p = 0.003), CIR (HR = 2.41, 95%CI, 1.42–4.09, p = 0.001), and for grade 2–4 acute GVHD (HR = 1.55, 95% CI, 1.02–2.35, p = 0.048) (supplementary Table 2).
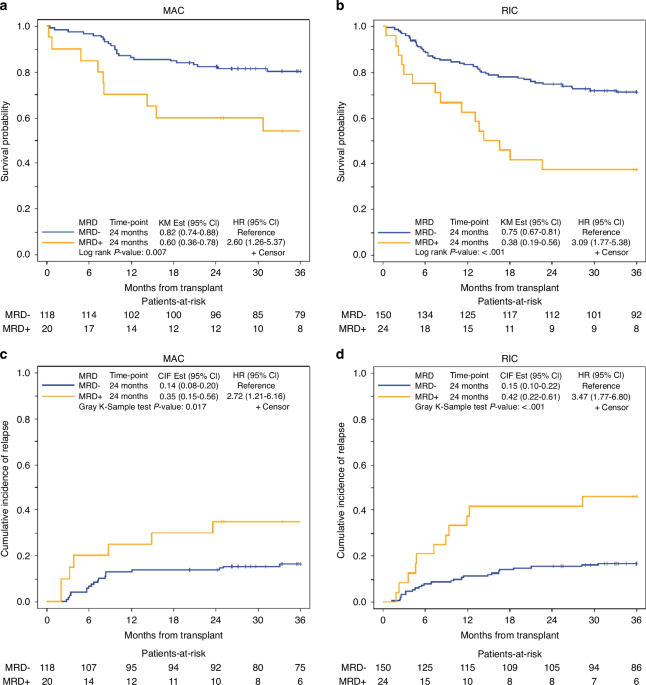
Impact of MRD-MFC in subgroups, conditioning intensity (FluMel and MAC)As shown in supplementary Table 1 conditioning intensity was associated with OS (HR = 1.48, 95% CI, 1.00–2.21, p = 0.049) in favor of MAC regardless of MRD status, but there was no statistically significant association with LFS, CIR, or NRM. We examined the impact of MFC-MRD separately in FluMel (n = 24 MRD+ and 150 MRD−) and MAC (n = 20 MRD+ and 118 MRD−); and showed MRD+ was associated with significantly worse 2-year OS in patients who received both MAC (60% vs. 82%, p = 0.007) and FluMel (38% vs. 75%, p = <0.001) (Fig. 1a, b, Table 3) with HR of 2.6 and 3.09, respectively. Similarly, higher 2-year CIR was observed in patients with MRD+ who received MAC (35% vs 14%, p = 0.017) and FluMel (42% vs. 15%, p = <0.001) (Fig. 1c, d, Table 3) with similar HR of 2.72 and 3.47, respectively. Among MFC-MRD+ patients (n = 44) there was no significant difference between those who received MAC (n = 20) compared with FluMel (n = 24) in 24-month OS (60% vs. 38%, p = 0.21), or CIR (35% vs. 42%, p = 0.59), respectively (Fig. 2).
Fig. 1: Overall survival and cumulative incidence of relapse by pre-transplant MRD status in patients who received reduced intensity vs. myeloablative conditioning.
a OS in MRD+ and MRD− patients who received MAC. b OS in MRD+ and MRD− patients who received RIC. c CIR in MRD+ and MRD− patients who received MAC. d CIR in MRD+ and MRD− patients who received RIC.
Table 3 Overall survival and cumulative incidence of relapse by conditioning and GVHD prophylaxis.Fig. 2: Overall survival and cumulative incidence of relapse by conditioning regimen (RIC vs. MAC) in patients with pre-transplant MRD− vs. MRD+ status.
a OS of MAC vs. RIC in MRD− patients. b OS of MAC vs. RIC in MRD+ patients. c CIR of MAC vs. RIC in MRD− patients. d CIR of MAC vs. RIC in MRD+ patients.
Of patients treated with FluMel with MRD+ disease, 10/24 received melphalan 100 mg/m2 and 14 received 140 mg/m2. Only 2 patients who received 100 mg/m2 are alive at time of analysis; 5 patients experienced relapse and 2 patients died during the peri-transplant period with NRM. No patients received doses of melphalan above 140 mg/m2.
Impact of MRD-MFC in subgroups, GVHD prophylaxis (Tacro/Siro and PTCy)The use of tacro/siro or PTCy as GVHD prophylaxis was not associated with significant differences in OS, LFS, or CIR (Supplementary Table 1). We examined the impact of MFC-MRD+ separately in tacro/siro (n = 28) and PTCy (n = 16). MRD+ was associated with slightly worse OS compared to MRD- in patients who received tacro/siro at 2 years (61% vs. 76.0%, HR 1.82, p = 0.041), whereas in those who received PTCy, there was a larger difference (25% vs. 82%, HR 6.28, p = <0.001) (Fig. 3a, b, Table 3). Similarly, higher CIR was observed in patients with MRD+ compared to MRD- who received tacro/siro (29% vs 16% at 2-years, p = 0.035) and PTCy (56% vs. 12% at 2 years, p = <0.001) (Fig. 3c, d, Table 3) with HR or 2.16 and 5.49, respectively. Among MFC-MRD+ patients (n = 44), OS was longer in those who received tacro/siro (n = 28) compared with PTCy (n = 16) with 24-month OS (61% vs. 25%, p = 0.042) with HR of 2.16 (Fig. 4a, b); however, there was no significant difference in CIR noting small sample size (29% vs. 56%, p = 0.14) (Fig. 4c, d).
Fig. 3: Overall survival and cumulative incidence of relapse by pre-transplant MRD status in patients who received PTCy-based compared to tacrolimus/sirolimus-based GVHD prophylaxis.
a OS in MRD− and MRD+ patients who received PTCy-based GVHD prophylaxis. b OS in MRD− and MRD+ patients who received tacrolimus/sirolimus-based GVHD prophylaxis. c CIR in MRD− and MRD+ patients who received PTCy-based GVHD prophylaxis. d CIR in MRD− and MRD+ patients who received tacrolimus/sirolimus-based GVHD prophylaxis.
Fig. 4: Overall survival and cumulative incidence of relapse by GVHD prophylaxis in patients with pre-transplant MRD− vs. MRD+ status.
a OS of tacrolimus/sirolimus-based vs. PTCy-based GVHD prophylaxis in MRD− patients. b OS of tacrolimus/sirolimus-based vs. PTCy-based GVHD prophylaxis in MRD+ patients. c CIR of tacrolimus/sirolimus-based vs. PTCy-based GVHD prophylaxis in MRD− patients. d CIR of tacrolimus/sirolimus-based vs. PTCy-based GVHD prophylaxis in MRD+ patients.
Impact of MRD-MFC in subgroups, ELN risk groupAs shown in Table 2, ELN risk stratification was not independently associated with OS, LFS, CIR or NRM. There was a trend towards improved survival in favorable or intermediate risk disease, and similarly a trend towards higher CIR and shorter LFS in those with adverse risk disease. The 2-year CIR in MRD+ vs. MRD- in the intermediate ELN risk group was 36% vs. 12% (95% CI, p = 0.004) with HR of 3.69. In the ELN favorable risk group, the 2-year CIR in MRD+ vs MRD- was 80% vs 9% (95% CI, p < 0.001) with HR of 15.67. In the ELN adverse risk group, there was no statistically significant difference in the 2-year CIR in MRD+ vs. MRD- with 31% vs. 20% (95% CI, p = 0.124) experiencing relapse (Supplementary Fig. 2).
留言 (0)