Even though the rehabilitation plays a key part in the patient’s recovery after major trauma, this is mainly performed upon individual/regional clinic standards. Evidence-based literature on conduction of rehabilitation in polytrauma patients is rare to non-existent even though they are available for more isolated injury pattern. To a certain extent this is understandable, since standardized and reproducible research in this field is not easily possible, as polytrauma with all its varying definitions does not describe one specific injury pattern that can be targeted by one specific treatment approach but more a condition that is brought together by multiple injuries. Therefore, one would hardly be able to conduct any kind of randomized clinical trial on comparable patient cohorts with the aim to evaluate which one is more effective.
Yet, despite its obvious challenges, at least a standardized approach in the initial assessment and prioritization of different therapies is urgently required.
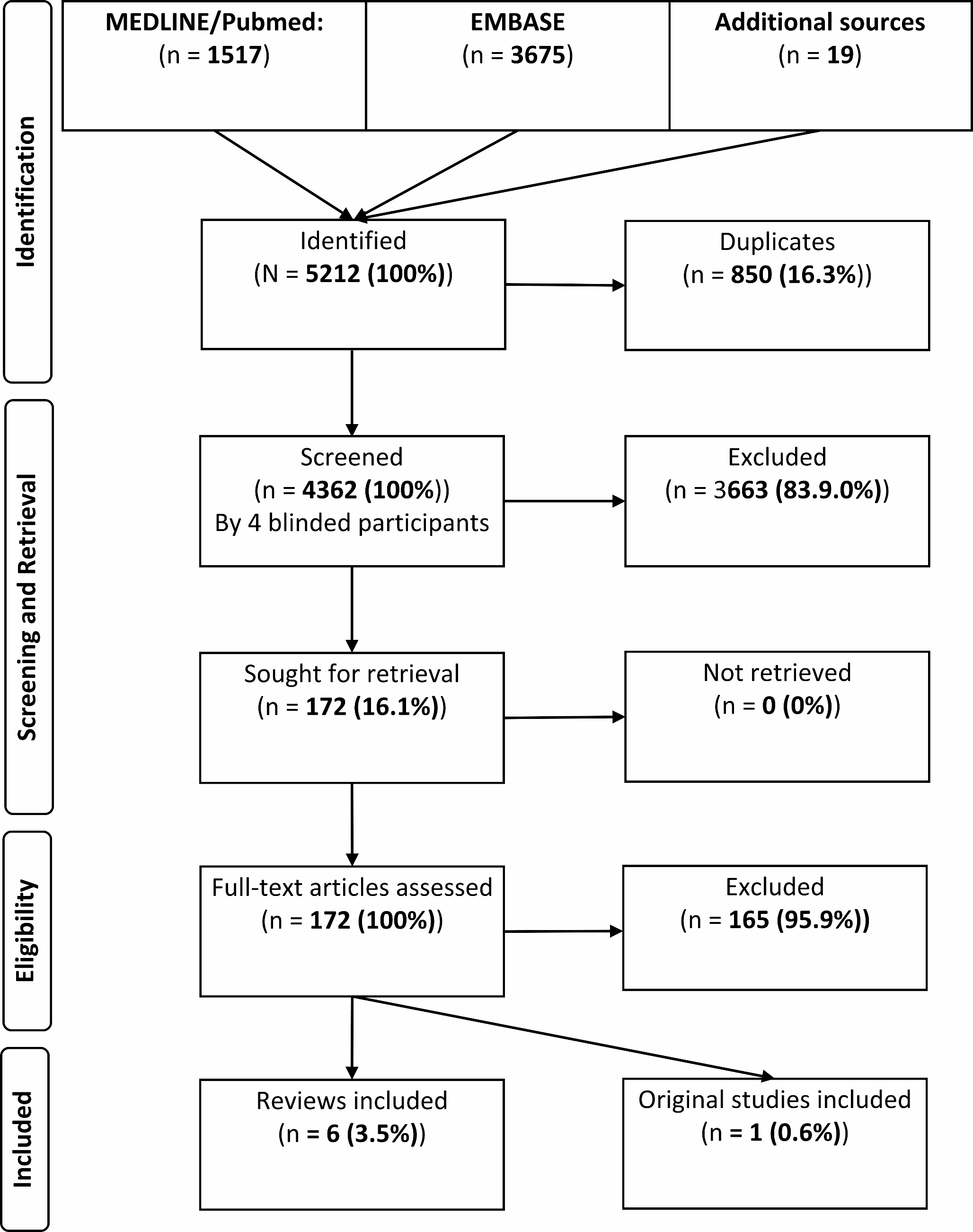
The reported literature in this article presents an overview of existing articles with emphasis on the different aspects stratified to the individual rehabilitation stage.
Based on the findings of this systematic review, we are able to formulate following main statement:
The fact, that there is a lack of evidence in polytrauma rehabilitation has already been addressed by previous publications [3, 11]. Also in our extensive literature search, no clinical trial was identified that delivered elevated evidence on the rehabilitation in polytrauma patients. Sporadic literature was identified addressing the subjective feedback of patients and professionals on conducted polytrauma rehabilitation [12]. Yet, this is mainly focused on procedural procedures and self-perceptions that are difficult to objectify but provide important aspects to improve constantly the overall quality of rehabilitation.
Additionally, the authors could not identify specific recommendations in existing guidelines. Most guidelines on polytrauma care are focused on the initial phase and surgical/medical procedures or are focused on isolated injury patterns, which they provide specific rehabilitation advice on [13, 14]. One of the few more general recommendations identified were an immediate start of physio- and occupational therapy next to psychological support [15].
The “Rehabilitation gap/hole” is a term that is often referred to in the existing literature. It is meant as a loss of rehabilitation time on the road to recovery. This risk especially occurs in the interface between different rehabilitation stages as the patient for example does not present enough rehabilitation potential for post-acute rehabilitation or organizational hurdles occur to transfer the patient from acute rehabilitation [16]. The DGU® proposed a new rehabilitation phase, called “early rehabilitation” that may bridge space between the acute and post-acute stage to strengthen the rehabilitation potential and might facilitate further therapy [17].
In our review of the literature, we were able to identify specific challenges that may occur during the rehabilitation journey and might impair the patient’s outcome. Those challenges should be tackled specifically by a multidisciplinary team, good organization and involvement of the patient in all belonging steps (Fig. 3).
In our review, we identified multiple therapies, aims and challenges in the respective rehabilitation phase. Following, we conclude the most important aspects in a description of an optimal rehabilitation process.
Acute rehabilitation
Rehabilitation should start as early as possible respective to the patient`s injury pattern and interaction capability (intubation/cerebral deficits). Specialists of the involved clinics are required to give detailed restrictions and limitations, according to which the patient may be mobilized and trained. Based on this, the multidisciplinary rehabilitation team, preferably consisting of members of physiotherapy, occupational therapy etc. should conduct adjusted rehabilitation from the very beginning [4]. Depending on the patient’s status and impairments, further specialists for i.e. dysphagia/speech therapy and psychological workup can be involved [6, 7] (Table 3).
The initial aim in the acute phase is to (1) Improve the rehabilitation potential and (2) Prevent complications (i.e. thromboembolic events or pulmonary complications). If the patient cannot interact, passive movements of the extremities can be performed; otherwise, this can be done actively and depending on the injury pattern and related restrictions, mobilization in or outside the bed can be performed [18]. This should support DVT (deep vein thrombosis) preventions that should already exist respective to the injury pattern (i.e. intracranial bleeding) either medical (anticoagulation) or device supported (pneumatic cuffs) [19]. In addition, breathing/airway therapy should be conducted especially in the presence of thoracic injuries to prevent complications as pneumonia.
As soon as the required rehabilitation potential is reached and medical/surgical therapy is finished, the patient should be transferred to a specialized rehabilitation facility. This requires good interdisciplinary communication and professional management of the rehabilitation chain [4]. Delay of specialized rehabilitation due to organizational problems should be strongly avoided [8]. Also re-transfer back to the acute hospital due to complications is a major problem that occurs in around 8% of cases [20].
Post-acute rehabilitation
The specialized rehabilitation has the potential to put the entire focus on the rehabilitation process, which is usually not possible in the acute hospital, where rehabilitation only takes place a short time a day. The aim in this “post-acute” setting is (1) Regaining physical function, (2) Setup for vocational/social reintegration and (3) Holistic therapy [8, 10]. Since the patient may not be able to pursue their former work even after completed rehabilitation due to disabilities or long-term functional limitations, social workers and vocational managers should be included into this process if not already done in the acute rehabilitation phase. Good involvement of the patient’s relatives is also important since they will play a major role especially after the patient is dismissed back into their former life [5]. Support in the social environment is required but may not exceed a certain level that the patient`s own growth is restricted. If psychological anomalies are observed or mentioned by the patient, a psychological consultancy should be conducted and followed up [8]. Consistent communication with initially treated hospital is essential to consult them in case, medical issues (i.e. infection, extraordinary pain, etc.) occur which might require a revision surgery or an intensive medical workup [20].
Long-term rehabilitation
After the post-acute rehabilitation is finished and the patient is dismissed into their former life, a long-term rehabilitation is required. The aim hereby is to (A) Improve functionality to the best possible condition, (B) Support the patient in the vocational and social reintegration and (C) Assist in residual issues as (chronic) pain or dealing with disabilities [8]. Since this stage is usually performed in an outpatient physiotherapy setting, it requires good preparation to not lose track of the patient afterwards since it is the one that relies the most on the patient’s motivation [5]. Medical aftercare organized by the responsible department with regular visits of the consultation hours are also required to identify medical problems and to track with the rehabilitation process with potential further changes of initial restrictions. Also there might be a need for further surgeries according to the reconstruction plan and clinical/radiological follow up of the osseous healing process are required to identify potential problems.





留言 (0)