Item selection and questionnaire development
The development and validation of the final RG-Psy followed multiple steps.
First, items were selected from the original RG as well as from Webber and Huxley’s adaptation for the UK (i.e. Resource Generator UK (RG-UK)) [10]. The RG-UK was built according to a rigorous methodology, has good consistency and high reliability. Selected items were then adapted by an expert in the sociology of mental health (VL) to be consistent with the psychiatric profession, in collaboration with a psychiatric clinical pharmacist (JL).
The response categories were also developed on the basis of the RG, the RG-UK and the International Social Survey Programme (ISSP) version [9], following the same steps. Each item has a 6-point response scale and is rated from 0 to 6 according to how close the resource was to the respondent. A cumulative scale, or unipolar scale, was used in the RG and therefore retained in the RG-Psy, as it is the best model for measuring social capital [8]. Answers were coded “0” when the respondent did not need a certain resource or it was not applicable to their situation, while answering the socially closest resource was coded “6”.
Second, the content validity of the draft version was assessed by conducting individual cognitive interviews with an expert panel of six clinicians (e.g. psychiatrists, clinical pharmacists). Cognitive methods aim to determine the process used by respondents to complete the survey [11, 12]. The think-aloud strategy is one of the cognitive interview techniques, and was chosen for the development of this questionnaire as it works better for self-administered questionnaires [12]. In this strategy, respondents are asked to think aloud while answering the questions, in order to identify the path leading to their response and to understand the reasons for any misunderstanding and how the question was misunderstood.
Variables potentially associated with the RG-Psy score
In addition to the RG-Psy, further data were collected, including age, gender, primary spoken language (i.e. Dutch or French), region of practice, practice setting (e.g. hospitals), number of years of practice and status (i.e. psychiatrist or resident in psychiatry).
Study population
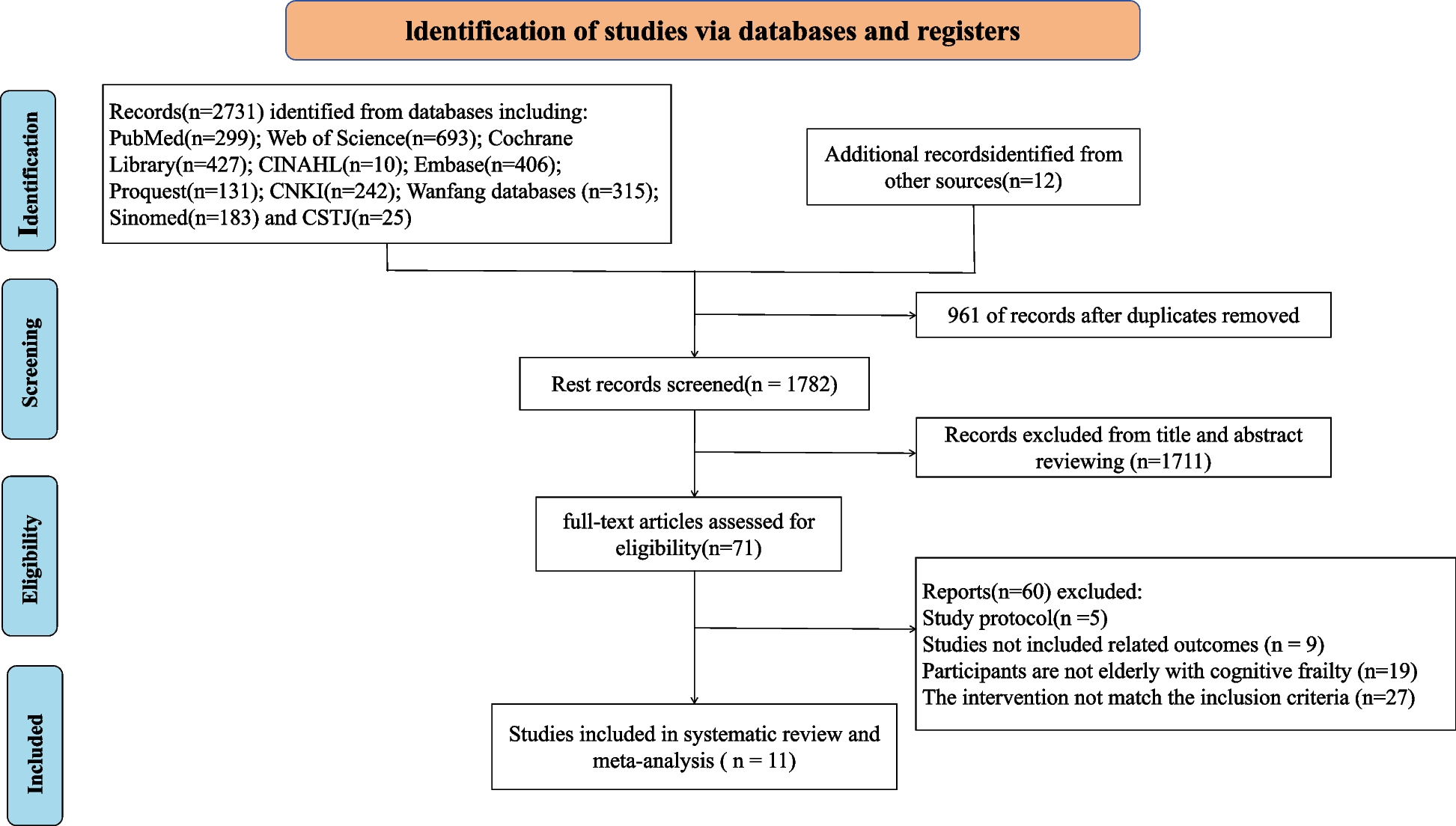
All adult psychiatrists and residents in psychiatry currently working in Belgium were eligible. In order to perform a probability sampling, the federal list of all psychiatrists licensed to work in Belgium was used to identify our target population. In addition, all residents in adult psychiatry were identified by contacting the head of the department of psychiatry in each Belgian medical school. E-mail addresses were obtained through hospital websites or phone calls for psychiatrists working in other settings (e.g. outpatient care).
Data collection
Our Belgian cross-sectional survey was distributed between April and July 2022 as an online self-administered questionnaire, available in French and Dutch. A link to the survey was sent by e-mail with personalised invitations. Psychiatry residents were contacted through their supervisors, who forwarded the invitation with a link to the survey. A maximum of three reminders were sent every 7 to 10 days to clinicians who did not complete or open the questionnaire. Data were extracted one month after the last reminder was sent.
Evaluation of psychometric characteristics
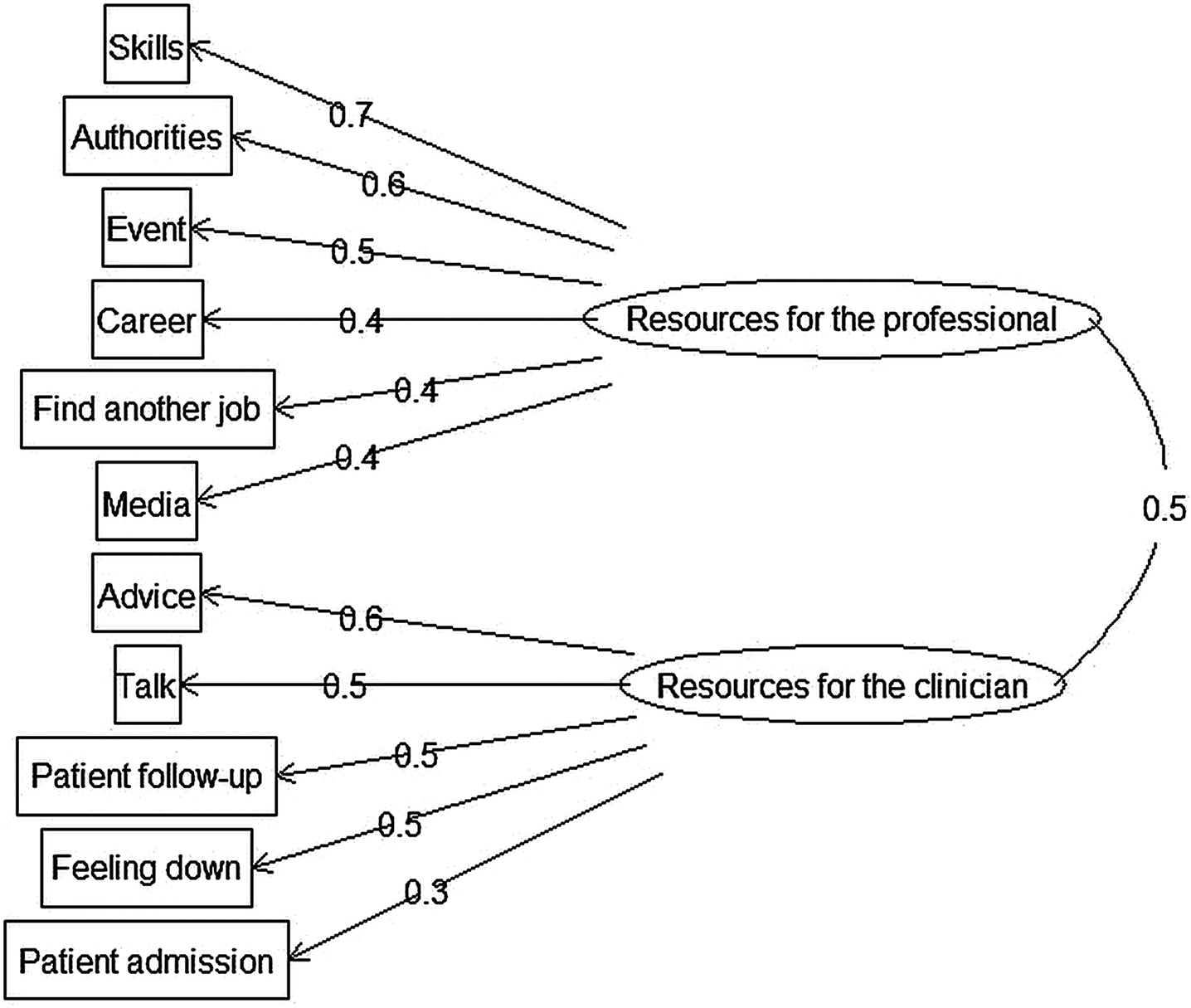
An exploratory factor analysis (EFA) was conducted to assess the structure validity of the scale. EFA aims to identify the underlying dimensions of a domain [13] in order to determine the latent structure of the scale [14]. When different theoretical constructs are identified [13], this indicates the scale is better summarised using subscales [15]. EFA was used instead of confirmatory factor analysis as there was no clear hypothesis regarding the structure of the factors [13, 15].
In order to check the appropriateness of carrying out an EFA, the adequacy of the data must be verified. A Kaiser-Meyer-Olkin (KMO) test was used, where a KMO ≥ 0.6 indicates sampling adequacy [16]. Bartlett’s test of sphericity was also performed to reject the hypothesis of independence between variables. Finally, inspection of the correlation matrices was undertaken [16].
There are several methods of factor extraction, such as principal component analysis, maximum likelihood and principal axis factorisation. Principal component analysis is considered a reduction method, while maximum likelihood and principal axis factorisation are used to test the statistical significance of factor loadings and correlations between factors, as well as to calculate confidence intervals. Principal axis factorisation is best used when there is a significant violation of normality [13, 17, 18]. EFA with maximum likelihood for factor extraction was therefore used, because it is the most appropriate method when the data are relatively normally distributed, which was ensured for both univariate and multivariate normality [14]. The number of factors to be retained was determined using the scree test, which involves examining the graph of eigenvalues of unrotated factors (i.e. the scree plot) and identifying the point where the slope breaks. The number of points above the break determine the number of factors to be retained [13, 14, 17]. Promax rotation (i.e. oblique method) was used because items were correlated [13, 17]. After rotation, items loading ≥ 0.3 for one factor were kept and grouped with the corresponding factor. Cross-loadings were assessed, and defined as an item loading on more than one factor [17].
Internal consistency was then examined using Cronbach’s alpha for each subscale and the total scale, and also using item-total correlation (ITC) [19]. Internal consistency refers to “the extent to which items are correlated (homogeneous), thus measuring the same concept” [15]. A Cronbach’s alpha between 0.7 and 0.9 indicates reliable internal consistency [15]. ITC calculates the correlation of each item with the mean total score of the scale [19]. Different threshold values for ITC to keep an item in the scale have been described, mainly 0.2 [20, 21] and 0.4 [19].
Finally, test-retest reliability was verified using the intra-class correlation (ICC), as this is the most appropriate parameter for continuous measurements [15]. A purposive sample of eight respondents were asked to complete the survey twice at one-week intervals. An ICC above 0.7 is considered reliable [15, 21].
Statistical analysis
The sum of all item responses was used to calculate the total RG-Psy score, which was the dependent variable. A multivariable linear regression model was run with stepwise backward elimination based on the Akaike Information Criterion to select the final model, in which p-values < 0.05 were considered significant. Factors included in the initial model are detailed in the Online supplementary material (eTable 1). Statistical analysis was conducted using R software version 4.0.3. The packages car, rms, psych and dplyr were used.
Ethics
This study was approved by the ethics committee of Université Catholique de Louvain (No. 2022/08FEV/055).
Participation was voluntary, and each respondent provided informed consent before completing the questionnaire. Responses were anonymous.







留言 (0)