
記住我






The 2022 Kenya Demographic and Health Survey (KDHS) data was used in this study, which used a two-stage stratified sampling approach. The first stage involved selecting 1692 enumeration areas (EAs) or clusters from a master sample frame of 129,067 EAs from the 2019 Kenya population and housing census using equal probability and independent selection [12]. The second stage involved household listings to build a sampling frame from which 25 households per cluster were chosen. If a cluster had fewer than 25 households, all of them were sampled. The survey was carried out in 1691 clusters in total. The Inner-City Fund (ICF) aided in the pre-testing of study tools as well as the training of data collectors. Data was collected between February and July 2022. All women between the ages of 15 and 49 who were regular members of the selected families or who had slept in those households the night before the survey were interviewed in Swahili or English. This analysis comprised 11,863 women who were either pregnant or had just given birth during the previous 5 years out of 32,156 women who answered the survey. We got explicit permission to use the 2022 KDHS dataset from the MEASURE DHS website (https://www.dhsprogram.com/data/available-datasets.cfm). Although the dataset comprised numerous variables, we only investigated and used those that were significant and appropriate to our study.
Study variablesDependent/outcomesThe quality of PNC was computed as a dependent variable in this study. The quality of postnatal care was a composite variable computed from multiple binary outcomes (yes vs. no) which included whether the mother or their baby had received certain services from health workers during the first two days of the postnatal period. The services included examining the newborn’s umbilical cord, showing the mother how to clean the umbilical cord, observing the mother while breastfeeding their newborns, taking the newborn’s temperature and the mother’s blood pressure, counseling or advising the mother about breastfeeding, family planning, vaginal bleeding, and danger signs associated with newborn illness. Therefore, the quality of PNC was defined as the mother receiving all these postnatal services (yes). If the mother missed one of the nine postnatal services (no) then they were considered to have not received quality PNC [20].
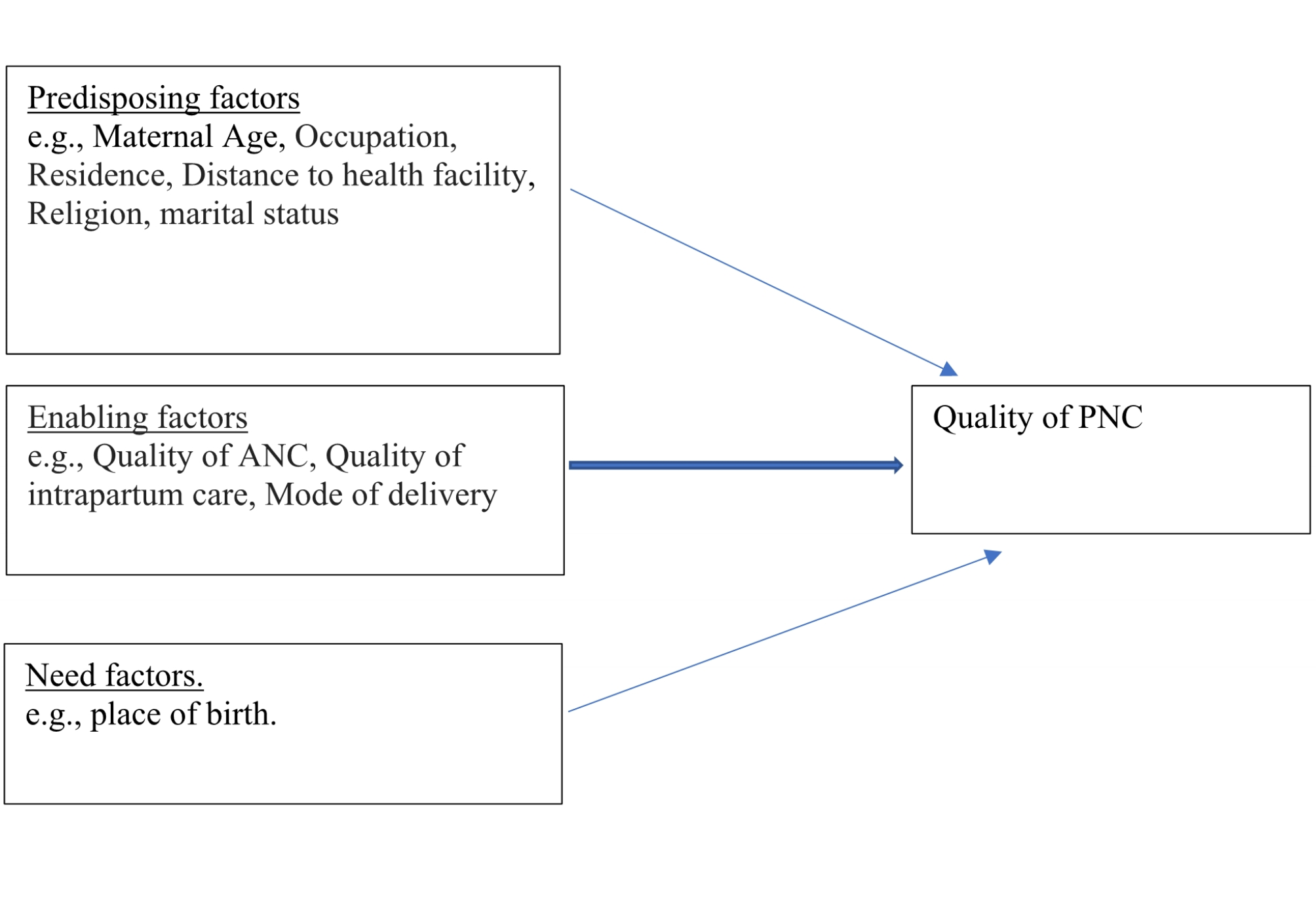
Independent variablesBased on the literature review and the availability of the variables of interest in the KDHS dataset, factors included in the analysis were categorized into three namely sociodemographic, obstetric, and health facility-related characteristics [3, 7, 11, 19,20,21]. These variables were also further categorized into predisposing, enabling, and need factors (Fig. 1).
Fig. 1 Sociodemographic characteristics
Sociodemographic characteristicsWe included nineteen sociodemographic factors in the analysis. These factors included wealth index in five classes (poorest to richest), husband and maternal education (tertiary, secondary or none/primary), marital status (married, separated/divorced/widowed, or single), age in years (15–19, 20–34, 35–49), husband and maternal working status (no or yes), residence (rural or urban), and religion (Muslim, Christian, or others). The region was categorized into the eight provinces of Kenya (Rift Valley, Nairobi, Central, Northeastern, Eastern, Western, Coast, and Nyanza). Family composition was measured as the number of household members (≤ 4 or ≥ 5). Telephone ownership, and exposure to mass media such as television, newspapers, the internet, and radio (no or yes) were also included in the analysis. Maternal autonomy was assessed through two proxy variables namely, who makes healthcare-seeking decisions for the mother/participant (self, jointly with partner or another person, partner, or others) and who heads the household (male or female). It is worth noting that the wealth index was calculated by 2022 KDHS from information on household asset ownership using principal component analysis [12].
Obstetric and child-related factorsThirteen obstetric and child-related factors were included in the analysis, such as the number of living children, the birth interval in months (≤ 24 or ≥ 25 ), receiving information about PNC from a community health worker (yes or no), antenatal care (ANC) visits (≤ 3 or ≥ 4), timing of first ANC visit in months (0–3, 4–6, 7–9), age at first birth in 5 year age groups (≤ 19yrs, 20-24yrs, 25-29yrs, 30-34yrs, ≥ 35), mode of delivery (vaginal or cesarean), and wantedness of the pregnancy (yes or no).
Two composite variables (quality of antenatal care and intrapartum care) were included in the analysis. The quality of antenatal care was computed from multiple binary outcomes (yes or no) which included whether the mother had received all eight services provided during ANC (such as taking off urine samples and blood samples, breastfeeding counseling, taking blood pressure, nutritional counseling, monitoring fetal heartbeat, receiving advice about the danger signs of pregnancy (bleeding), and receiving (or buying) iron tablets) [22]. Whereas receiving the quality of intrapartum care was constructed from three binary variables (yes/no), namely (1) receiving skilled assistance during birth; (2) facility-based delivery, and (3) the skilled birth attendant placing the baby on the mother’s chest within one hour after birth. Therefore, receiving quality antenatal or intrapartum care meant a woman receiving all elements of antenatal or intrapartum care which was recategorized as a binary outcome (yes/no). Lastly, child-related factors included the sex of the child (male, female), and the current age of the child in years (≤ 1, ≥ 2 years).
Health facility factorsWe included five variables related to the place of delivery or PNC such as who assisted the mother during delivery and in the postnatal period (doctor, nurse/midwife/clinical officer, or others), the specific place of delivery (non-governmental organizational (NGO), public, private, and faith-based organization (FBO) health facilities or clinics), and being treated with respect at the health facility (sometimes, all the time, or not at all). Minutes to a health facility of birth (≥ 61, 31–60, ≤ 30) were also added to the analysis as a proxy indicator of access to the health facility.
Statistical analysisData were cleaned and dummy variables were established before analysis. For all categorical variables, descriptive statistics such as frequencies were calculated at the univariate level. Pearson chi-square statistics and univariate logistic regression were used to identify independent factors associated with the quality of PNC. All variables with P-values less than 0.05 were included in simple multivariate logistic regression to determine the characteristics associated with the quality of PNC while controlling for confounders. The odds ratios for all variables are presented with 95% confidence intervals. To analyze the data, the complex samples package in SPSS (Version 20) was utilized, which helped account for the complicated sample design inherent in DHS data.
The complex sample package gives correct parameter estimates since it accounts for sample stratification, weighting, and clustering that happened during the study participants’ sampling [23, 24]. DHS sample weights were also applied to all frequencies computed to account for unequal probability sampling in different strata and assure the representativeness of the study results [23, 24]. During preliminary analysis, a variance inflation factor (VIF) of less than 10 was used as a criterion to examine multi-collinearity among all predictor variables in the model [23, 24]. The cutoff was not surpassed by any of the factors.
Ethical considerationThe Inner-City Fund (ICF) Institutional Review Board granted ethical approval for the investigation described in the datasets. The study was also conducted by the Kenya National Bureau of Statistics in collaboration with other stakeholders. Because the secondary data is publicly available, no additional ethical permission was required to examine it. However, MEASURE DHS granted access to the 2022 KDHS datasets (https://www.dhsprogram.com/data/available-datasets.cfm). Written informed consent was obtained from human participants and written informed consent was also obtained from legally authorized representatives of minor participants.
留言 (0)