
記住我







This single-center prospective study was approved by the institutional review board (M2023762) and registered in ClinicalTrials.gov (NCT06359795). Written informed consent for the evaluation and publication of anonymized data was obtained from all participants.
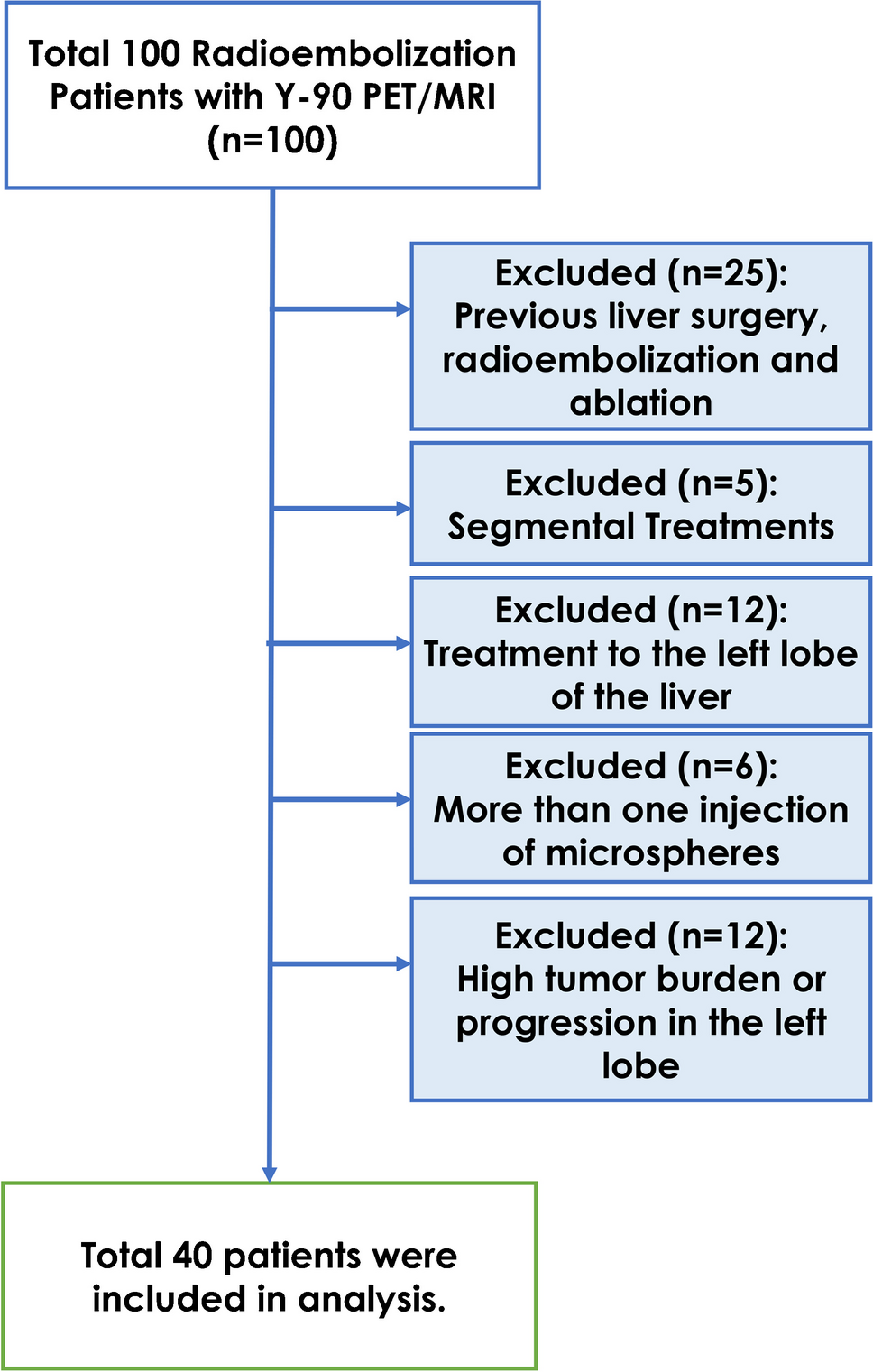
Patients diagnosed with TED based on European Group on Graves’ Orbitopathy (EUGOGO) criteria were included [5]. While, individuals were excluded with any of the following: 1) underwent bilateral orbital surgery, 2) received glucocorticoid, monoclonal antibody therapy, or external radiation therapy for TED within the past month, 3) were unable to maintain a supine position for the examination, or 4) were planning pregnancy, pregnant, or in the lactation period. From December 2023 to May 2024, 23 individuals with TED were consecutively recruited. Simultaneously, 10 healthy controls (20 eyes) were enrolled. All participants underwent [18F]AlF-NOTA-FAPI-04 PET/CT scan. The TED eyes were classified by CAS-driven assessment as active (CAS +) or inactive (CAS-). [18F]AlF-NOTA-FAPI-04 PET analysis included both qualitative and quantitative evaluations. Qualitative analysis categorized TED eyes as positive (FAPI +) or negative (FAPI-), while quantitative analysis including SUVmax and target-to-backgroud ratio (TBR) of EOM. The SUVmax and TBR in EOMs was compared among CAS-/FAPI + , CAS + /FAPI + , CAS-/FAPI-, CAS + /FAPI-, and control groups in patient-based and eye-based analyses. Additionally, pathological assessment was conducted on EOM samples from the TED patients who underwent both strabismus and orbital decompression surgery. The pathological results were used as gold standard to evaluate the diagnostic accuracy of CAS-driven and FAPI-driven assessments. Correlations between SUVmax and pathological findings were also analyzed. A flowchart of patient enrollment and study profile was shown in Fig. 1.
Fig. 1
Flowchart of participant enrollment and study profile. CAS = Clinical Activity Score, FAPI = fibroblast activation protein inhibitor, TED = thyroid eye disease
Clinical activity score-driven assessment of TEDThe CAS comprises seven items for the first visit: 1) spontaneous retrobulbar pain, 2) pain on attempted upward or downward gaze, 3) redness of eyelids, 4) redness of conjunctiva, 5) swelling of caruncle or plica, 6) swelling of eyelids, and 7) swelling of conjunctiva (chemosis) [5]. TED is defined as active if CAS is ≥ 3/7. A ten-item CAS was used for follow-up assessments, incorporating three additional items: 8) an increase in exophthalmos ≥ 2 mm, 9) a decrease of eye movements in any direction of gaze ≥ 8°, 10) a decrease of visual acuity ≥ 1 line on the Snellen chart during a period of 1–3 months [5]. TED is defined as active if CAS is ≥ 4/10.
At enrollment, TED activity was clinically assessed eye-by-eye based on CAS-driven criteria by two experienced ophthalmologists (Y.W. and J.Z., both of them with > 15 years of experience in orbitopathy), categorizing all TED eyes as CAS + or CAS-. For patient-based analysis, a TED patient was classified as CAS- if both eyes were categorized as CAS-; otherwise, they were classified as CAS + . Detailed history of all TED patients, including subjective orbital symptoms, symptoms duration, and duration of thyroid disease, was recorded by a single ophthalmologist (D.Y., with 15 years of experience in orbitopathy, Table S1) at the first visit. Additionally, the history of smoking and thyroid-related disease was documented.
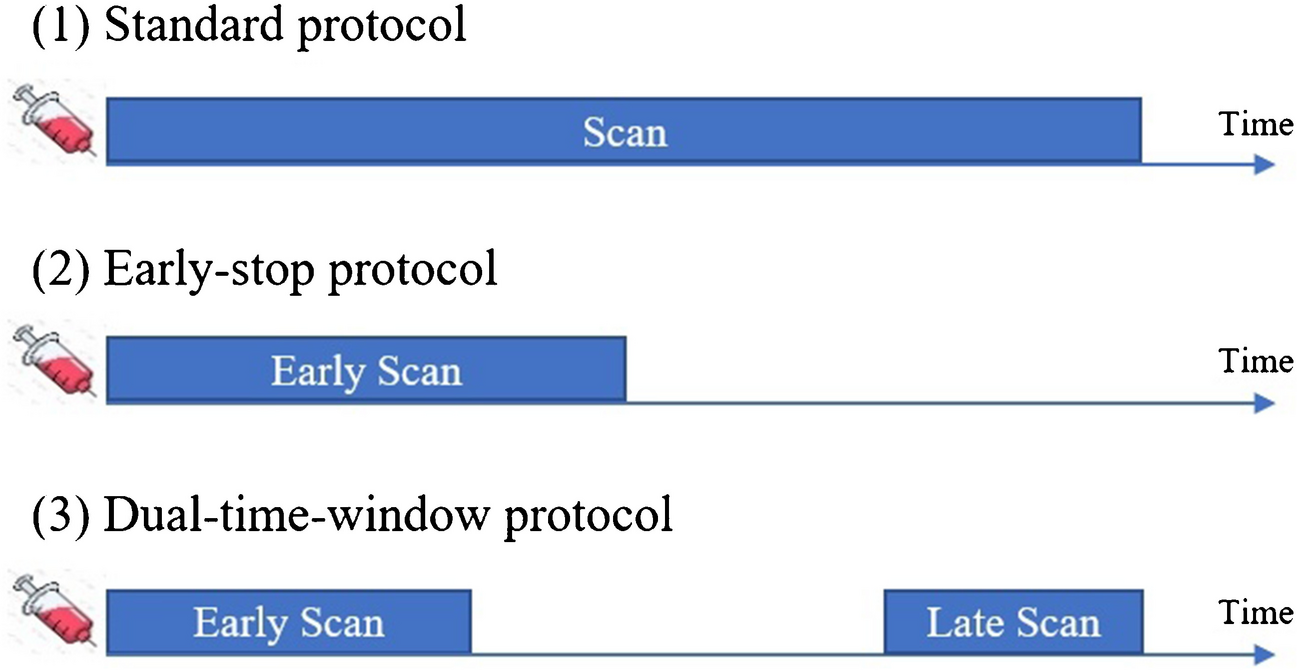
[18F]AlF-NOTA-FAPI-04 PET/CT imagingThe [18F]AlF-NOTA-FAPI-04 was obtained from DC AMS PHARMA (Beijing, China). The injection dose of [18F]AlF-NOTA-FAPI-04 was 3.7–5.55 MBq/Kg (0.1–0.15 mCi/Kg). The head was positioned within the PET field-of-view (FOV) for 6 min per bed to acquire imaging, 60–80 min after radiotracer injection on the PET/CT scanner (Biograph 64, Siemens, Germany). All corrections and reconstructions were conducted using the software provided by the PET/CT manufacturer.
Imaging analysisThree experienced nuclear medicine physicians (H.L., L.S., and W.Z., all of them with > 10 years of experience in PET/CT) assessed the PET/CT images. Reviews were performed in the absence of clinical data. TED eyes were visually classified as FAPI + if any EOM showed high FAPI uptake compared to the background; otherwise, they were classified as FAPI-. The FAPI-driven assessment was conducted eye-by-eye. For patient-based analysis, a TED patient was classified as FAPI- if both eyes were categorized as FAPI-; otherwise, they were classified as FAPI + . In case of disagreement among the readers, the final result was determined by consensus. The SUVmax of superior rectus muscle (SRM), medial rectus muscle (MRM), lateral rectus muscle (LRM), and inferior rectus muscle (IRM) was measured by the same nuclear medicine physician (H.L.) using the region-of-interest (ROI) method. A 1-cm ROI was placed on the soft tissue of the occipital region for background measurement. The TBR of EOMs was defined as (SUVmax of EOMs)/(SUVmax of background) and was quantified.
Pathological analysisIn total, 15 TED patients underwent both strabismus and orbital decompression surgery. Sixteen EOMs samples were obtained with patient consent and Ethical Committee approval (ethical No. M2024362) by the same ophthalmologist (Y.W.). The samples were formalin-fixed and paraffin-embedded (FFPE) for Hematoxylin–eosin (H&E) staining, Masson trichrome staining, and FAP immunochemistry staining. Pathological grading was defined and summarized in Table 1 [21, 22]. The inactive TED was pathologically defined as having both an inflammation and a fibrosis score ≤ 1, and a fibroinflammatory score ≤ 2. Otherwise, the EOMs samples were classified as active. All slices were reviewed and graded by experienced pathologists (H.W. and J.L, both of them with > 15 years of experience in pathology) in the absence of clinical and imaging data. In case of disagreement among the readers, the final result was determined by consensus.
Table 1 Pathological grading systemStatistical analysisResults were analyzed and visualized with Prism V.10 (GraphPad Software, San Diego, CA). Data were represented as mean ± standard deviation or median (percentiles 25–75). Comparisons among multiple groups for SUVmax and TBR were performed using analysis of variance for normally distributed data; otherwise, the Kruskal–Wallis test was used. P < 0.05 was considered as statistically significant. Significance levels are indicated as suggested by Prism Software: ns, no significant difference, *P < 0.05, ** P < 0.01, ***P < 0.001.
留言 (0)