
記住我
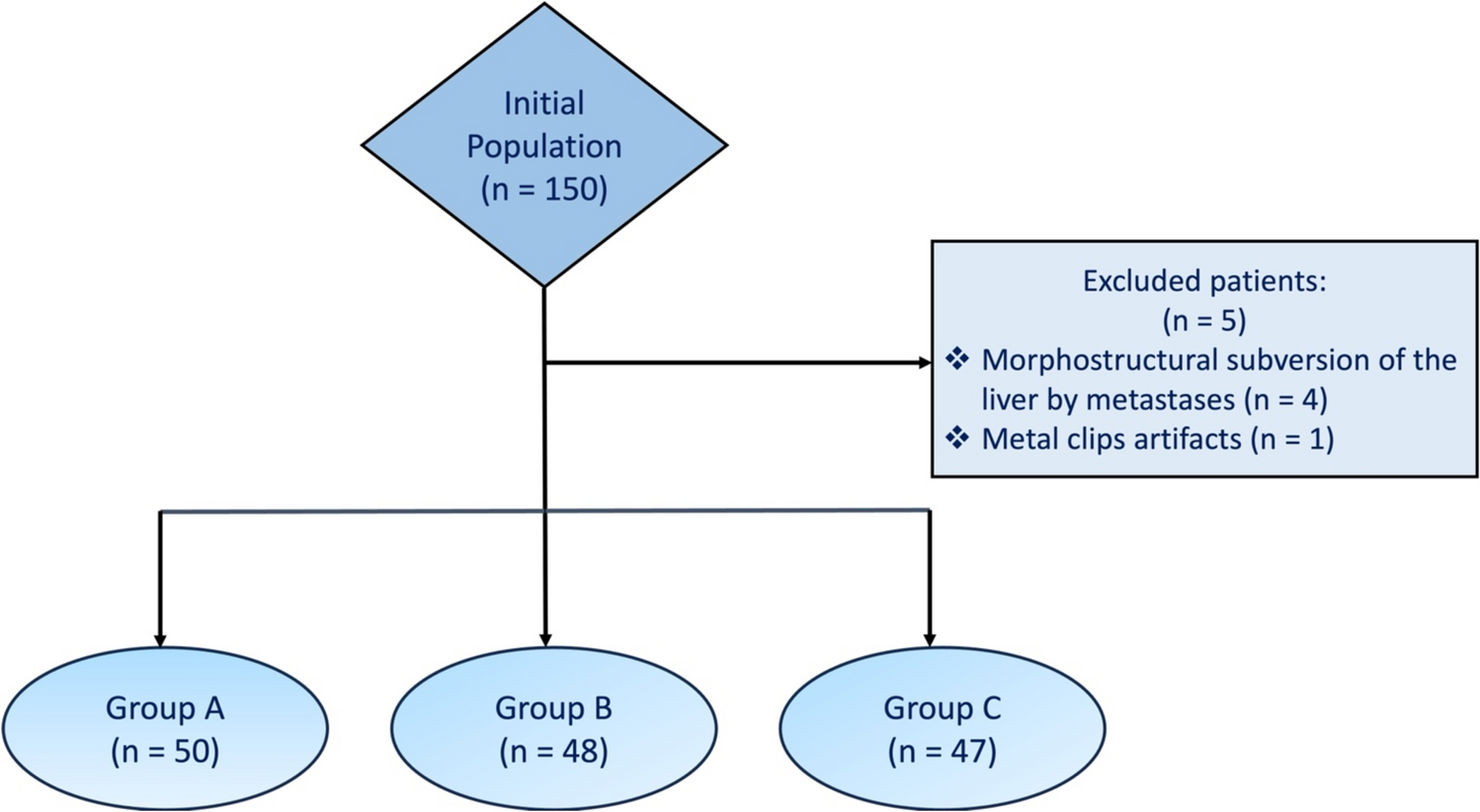





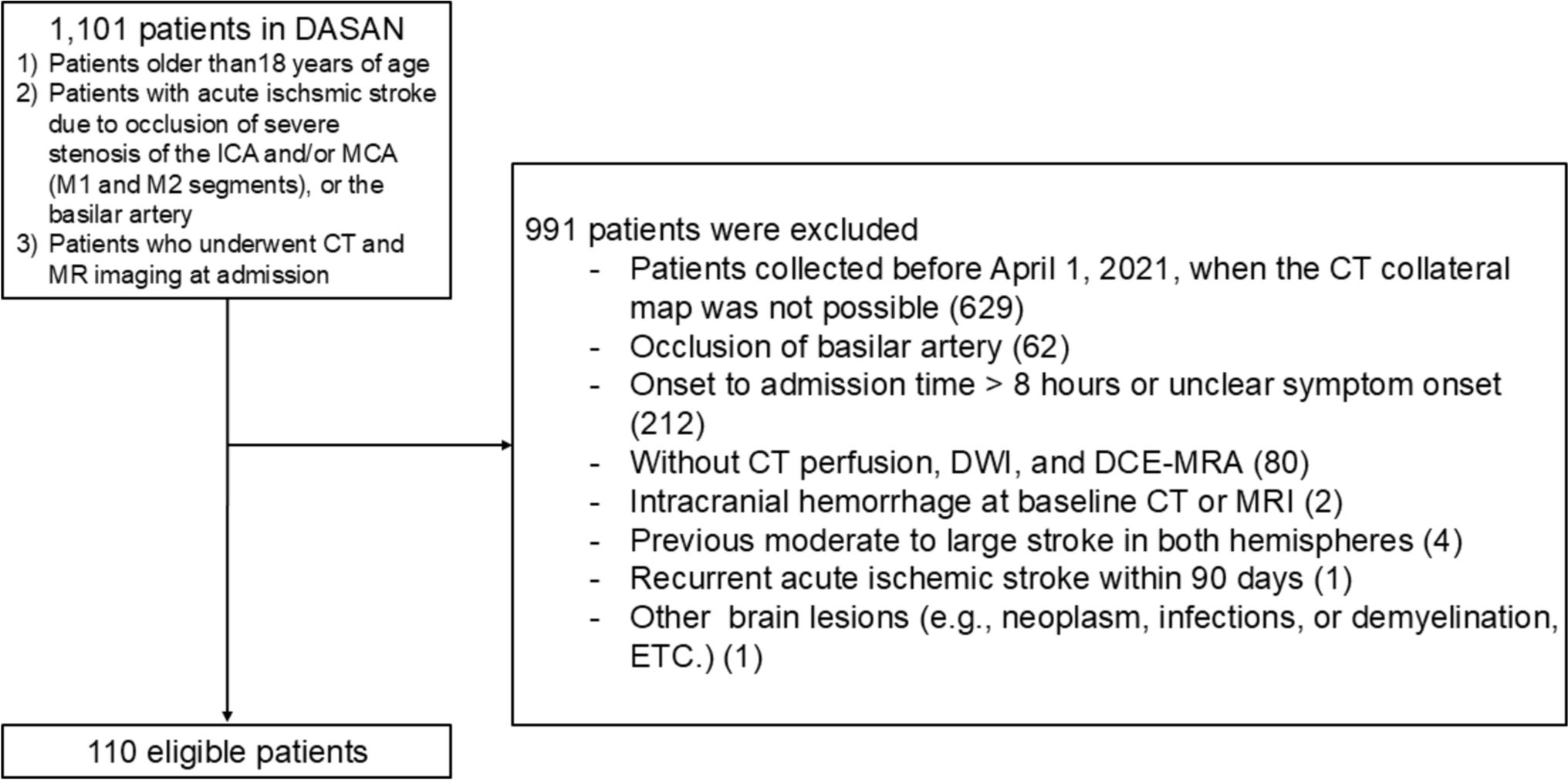
For this retrospective analysis, we selected patients from the ongoing Database of Acute ischemic Stroke Analysis Network (DASAN), prospectively gathered from two university hospitals starting January 1, 2016. The following DASAN inclusion criteria were used: (1) aged 18 years and older; (2) had AIS on DWI due to occlusion or severe stenosis of the internal carotid artery and/or the M1 or M2 segment of the middle cerebral artery (MCA) or the basilar artery; and (3) underwent brain CT imaging followed by MR imaging including DWI and DCE-MRA consequently at admission. Patients with steno-occlusion of the internal carotid artery and/or M1 or M2 segment of the MCA who were evaluated within 8 h of symptom onset and underwent CT perfusion, DWI, and DCE-MRA at admission were selected for this study. The exclusion criteria were as follows: patients whose data were collected before April 1, 2021, those for whom a CT collateral map was not possible, those with unclear symptom onset time, those with intracranial hemorrhage at baseline CT or MRI, those with a previous moderate to large stroke in both hemispheres, those who experienced recurrent AIS within 90 days, or those with other brain lesions (e.g., neoplasm, infection, or demyelination) (Fig. 1). Among the included patients, those who underwent follow-up DWI (f/uDWI) and angiography within 7 days and had unchanged stenoocclusive arterial lesions on follow-up angiography were selected for subgroup analysis to compare the predictive performance for f/uDWI lesion volume between the CMC lesion volume and the Tmax > 6 s lesion volume. Patient evaluations included demographic data, medical history, vascular risk factors, routine blood tests, brain imaging, and cardiological tests. Stroke severity was assessed using the National Institutes of Health Stroke Scale (NIHSS).
Fig. 1
Flowcharts showing patient inclusion. DASAN = database of acute ischemic stroke analysis network, DCE-MRA = dynamic contrast-enhanced magnetic resonance angiography, DWI = diffusion-weighted imaging, ICA = internal carotid artery, MCA = middle cerebral artery
Imaging protocol and postprocessing for generating of the CT and MRA collateral mapsNoncontrast brain CT, head and neck CT angiography, and CT perfusion were conducted using dual-source CT scanners. The CT perfusion protocol involved 49.5-s (s) acquisition, consisting of 18 scans with a 1.5-s interval, followed by 3 scans with a 3-s interval, 3 scans with a 4.5-s interval at 70 kVp and 150 mAs, 96 × 2 × 0.6-mm detector collimation and 114 mm z-axis coverage. Images were acquired with a 7-s delay after injection of 45 ml of iodinated contrast medium with 350 mg iodine/ml at a rate of 5 mL/s, followed by a saline chase of 40 ml at a rate of 5 mL/s. We developed an in-house software developed using Python (version 3.8.10) to generate a CT collateral map, 3-dimensional color-coded arterio- and venographies, and dynamic angiography. The sequential postprocessing steps for the CT collateral map and angiographies are demonstrated in Fig. 2.
Fig. 2
Postprocessing sequences for the CT collateral map using CT perfusion source images: (1) opening and reading DICOM source images of CT perfusion; (2) storing all acquired CT perfusion image data in a 4-dimensional matrix; (3) creating maximum intensity projection images for each time point representing bolus passage for each phase (A); (4) obtaining arterial and venous time-intensity curves for regions of interest on the major arteries (the middle cerebral artery, anterior cerebral artery or terminal internal carotid artery) in the nonischemic hemisphere and the superior sagittal sinus by plotting intensity changes in the region of interest (B); (5) separating the 4-dimensional images from CT perfusion into 5-phase data sets based on bolus passage status, plotted on the time-intensity curves (arterial phase = from the beginning of arrival of the contrast in the major artery to the arterial bolus peak; capillary phase = from just past the arterial bolus peak to just before the venous bolus peak in the superior sagittal sinus; early venous phase = first half of the venous phase from the venous bolus peak to the starting point of the venous plateau; late venous phase = second half of the venous phase; delay phase = from just past the venous phase to the end of the dynamic phase); and (6) reformatting the image data sets of each 5 phases into 5-phase axial image sets (CT collateral map) by averaging the intensities with the desired reconstruction parameters (slice range covering nearly the entire brain, slice thickness ranging from 7 to 15 mm, slice distance, and number of slices) (C). Using the optimal signal difference phase (the time point at which the maximum signal difference between the arterial and venous signal intensity-time curves in the arterial phase), color-coded arteriogram, venogram and dynamic angiography were simultaneously generated (D). The postprocessing time from loading source images of CT perfusion to generating the CT collateral map and angiographies was approximately 5 min
MRI was performed with 3-Tesla MRI scanners with acquisition parameters similar to those used in the previous study [10]. Utilizing source data from DCE-MRA, 3-dimensional rotational arteriography was conducted to determine the arterial status, and an MRA collateral map was reconstructed to evaluate the CP status. The MRA collateral map was generated using an in-house program following methods previously published [10], similar to those used for the CT collateral map.
Collateral perfusion grading system and imaging analysisBaseline and follow-up DWI lesion volumes were quantified using MEDIHUB STROKE software (version 2.1.0; JLK Inc., Seoul, Korea) [18]. The lesion growth ratio was calculated as the ratio of the f/uDWI lesion volume to the bDWI lesion volume, with lesion growth was defined as a lesion growth ratio ≥ 1.2 to account for the impact of vasogenic edema on the follow-up lesion volume. Given the perfusion thresholds of < 30% of the contralateral mean cerebral blood flow rate (CBF < 30%) and Tmax > 6 s are generally utilized for estimating the ischemic core and penumbra, respectively [19,20,21,22], the lesion volumes of baseline CBF < 30% (CBF < 30% lesion volume) and Tmax > 6 s were automatically computed using RAPID software. The mismatch ratio was defined as the ratio of Tmax > 6 s lesion volume to CBF < 30% lesion volume.
Three raters (H.G.R., with 23 years of experience as a neuroradiologist, H.J.K., with 8 years of experience as a neurosurgeon, and N.I.S., as fourth-year neurosurgery resident) who were blinded to all clinical and other imaging data independently graded the CP scores of both CT and MRA collateral maps in a blinded manner on two separate occasions, one week apart. The CP scores were as follows: 5, excellent; 4, good; 3, intermediate to good; 2, intermediate to poor; 1, poor; and 0, very poor (Table 1) [11, 12]. Final CP scores were determined by consensus among the raters. The CMC and CMEV lesion volumes were also measured by the three raters using Medical Image Processing, Analysis, and Visualization (MIPAV; version 7.1.1; National Institutes of Health, Bethesda, MD) as described in a previous study [12]. In the CMC, regions within the ischemic hemisphere with reduced perfusion compared to the contralateral hemisphere, and in the CMEV, regions of persisted hypoperfusion from the CMC were manually delineated on each slice using the freehand drawing brush tool (Fig. 3). The MIPAV software then automatically calculated the volume of the delineated areas across all slices by converting each outlined region into a voxel of interest. The final CMC and CMEV lesion volumes were determined by averaging the volumes measured by the three raters. The collateral ratio was calculated as the ratio of the CMC lesion volume to the CMEV lesion volume. In cases where the DWIs, CBF < 30%, and Tmax > 6 s lesion volumes measured by the software were 0 ml due to small lesions or when the collateral perfusion status was too favorable to detect hypoperfused lesions on the CT collateral map, volume values were considered 0.1 ml for statistical analysis.
Table 1 Collateral perfusion grading system for analysis of the CT and MRA collateral mapsFig. 3
Images of an 82-year-old woman with occlusion of the right middle cerebral artery (MCA) demonstrated on CT angiography (A). This patient had a premorbid modified Rankin Scale (mRS) score of 0, and her National Institutes of Health Stroke Scale (NIHSS) score at admission was 12. She received intravenous thrombolysis followed by intraarterial thrombectomy, resulting in complete recanalization of the occluded artery. Her 90-day mRS score was 3. Upon admission, a brain CT scan (B) showed indistinct differentiation between the cortical gray matter and white matter in the right temporal and insular regions, making it difficult to precisely determine the extent of the baseline lesion. CT perfusion analysis using RAPID software (RAPID, RapidAI®, Menlo Park, CA, USA) (C) indicated a baseline lesion volume of 0 ml, as measured by a relative cerebral blood flow threshold of < 30%, meaning the baseline lesion could not be identified. The CT collateral map, generated from the CT perfusion images (D–H) at admission, indicated poor collateral perfusion (collateral perfusion score of 1: collateral perfusion delay involving more than half of the MCA territory in the early venous phase and less than half in the late venous phase). Diffusion-weighted imaging (DWI) (I), performed immediately after the CT scan, revealed acute infarct signals in the right MCA territory. The extent of the DWI lesion at admission closely corresponded with the hypoperfused area visible up to the early venous phase on the CT collateral map (F). This suggests that even without DWI, the baseline lesion can be identified using a CT collateral map. The baseline lesion shows slight evolution on DWI on day 1 after recanalization of the occluded MCA (J). K and L are images shown on Medical Image Processing, Analysis, and Visualization (MIPAV; version 7.1.1; National Institutes of Health). These images display the hypoperfused lesion highlighted in the early venous (K) and capillary (L) phases, respectively, for assessing the hypoperfused lesion volume on the collateral map
Statistical analysisPatient characteristics are presented as the mean ± standard deviation or median (interquartile range [IQR]) for continuous variables, or as the number of patients (%) for categorical variables. Differences in the distribution of patient characteristics across CP scores were analyzed using the Chi-square test, Fisher’s exact test, ANOVA and the Kruskal‒Wallis test, as appropriate. The interrater reliabilities for CP grading of both CT and MRA collateral maps and the measurement of hypoperfused lesion volumes in the CMC and CMEV were assessed using Kendall’s coefficient of concordance for an ordinal response and concordance correlation coefficient (CCC) for a continuous response, respectively. The agreement between the CP scores of the CT and MRA collateral maps was evaluated using the weighted Cohen’s kappa coefficient. To assess the accuracy of bDWI and f/uDWI lesion volumes between the conventional perfusion thresholds (CBF < 30% and Tmax > 6 s lesion volumes) and CT collateral map values (CMC and CMEV lesion volumes), CCC and linear regression analyses were performed. The correlation of the mismatch and collateral ratios with the lesion growth ratio was determined using the CCC. Significance levels were set at a 2-tailed P value less than 0.05. Statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC).
留言 (0)