
記住我





The study was approved by the Institutional Review Board at Banan Hospital and Xinqiao Hospital. The requirement for individual informed consent was waived because of the retrospective nature of the study, and the data were anonymized. The clinical data of patients with aneurysms who were consecutively admitted to our participating centers between August 2011 and May 2021 were retrospectively analyzed. The exclusion criteria for this study were as follows: (1) age younger than 18 years; (2) nonsaccular aneurysms, (such as fusiform, dissection, traumatic or infectious aneurysms); (3) diagnosed with vascular diseases (such as vascular malformations and moyamoya disease) and (4) incomplete clinical or CTA image data.
All the aneurysms were divided into two groups: stable aneurysms and unstable aneurysms. The criteria for unstable aneurysms included RIAs (more prone to rebleeding), aneurysm progression (size increase ≥ 1 mm, shape change or rupture) during follow-up on CTA or MRA and aneurysms associated with neurological symptoms (e.g., blepharoptosis) [16, 29, 30]. The remaining aneurysms were defined as stable aneurysms. Asymptomatic UIAs were followed for ≥ 3 months via CTA or MRA to determine whether the aneurysms were stable.
Acquisition of clinical and morphological featuresPatient clinical characteristics, including sex, age, alcohol consumption status, smoking status, hypertension status, diabetes mellitus status, cerebrovascular sclerosis status, heart disease status and history of aneurysmal SAH, were collected from medical records. Cerebrovascular sclerosis was defined as diffuse atherosclerosis of the brain, luminal stenosis and small vessel occlusion, the diagnosis was made on the basis of CTA or transcranial ultrasound.
All the CTA images were transferred to the GE Advantage workstation (Advantage Windows 4.5) to generate 3D-volume renderings (VRs). As in the previous studies, the morphological parameters of aneurysms were measured directly from 3D-VRs [31, 32]. All the CTA images were evaluated separately by two observers (one with 10 years of experience in vascular imaging and the other with 20 years of experience in neuroradiology) who were blinded to patient information and stability status. For patients with asymptomatic UIAs, follow-up images of the aneurysms were used to determine whether the aneurysm grew, and the first CTA study was used for analysis. Continuous data were calculated as average values obtained by the two observers. Discrepancies in categorical data were resolved by a third reader (with 25 years of experience in neuroradiology).
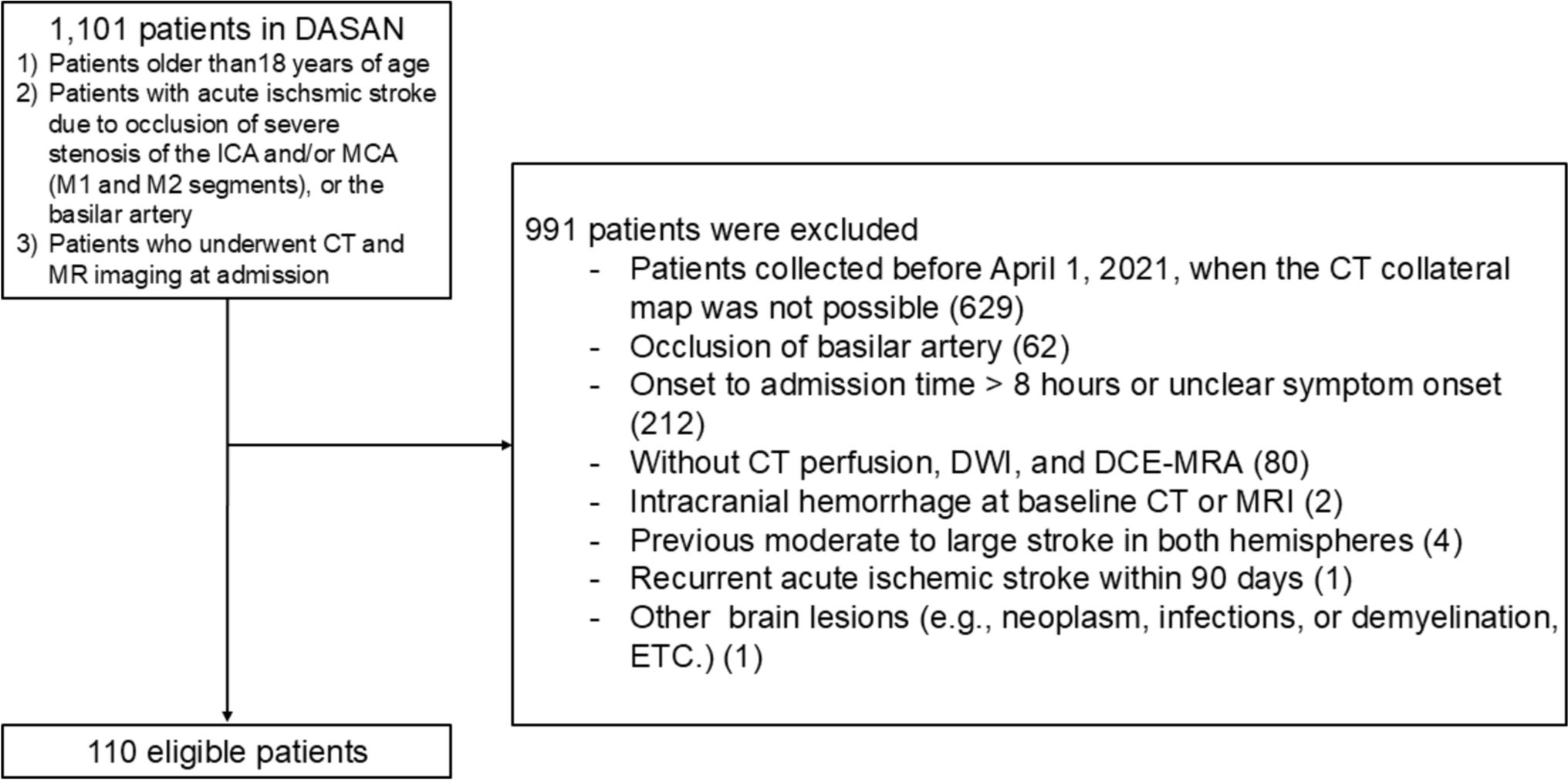
The locations of the aneurysms were classified as the internal carotid artery (ICA), middle cerebral artery (MCA), anterior cerebral artery (ACA), anterior communicating artery (ACoA), posterior communicating artery (PCoA) or posterior circulation artery (PCA). The categorical morphological variables included the origin of the aneurysm (sidewall or bifurcation type), shape of the aneurysm (regular or irregular shape) and number of aneurysms. Aneurysms located at parent artery bifurcations were defined as the bifurcation type, and those originating from only one parent vessel were defined as the sidewall type [33]. An aneurysm with a lobular or daughter sac was defined as having an irregular shape. Multiple aneurysms were defined as the presence of more than 2 aneurysms in a single patient. The size of the aneurysm (maximum size, neck width, depth and width), the flow angle (FA) and the diameter of the parent artery were measured manually (Fig. 1). In addition, four secondary geometric morphology indices, including the aspect ratio (AR, depth/neck width), size ratio (SR, depth/parent artery diameter), depth-to-width ratio (DW, depth/width) and bottleneck factor (BF, width/neck width), were calculated. These variables have been clearly depicted in the previous literature [31].
Fig. 1
The image shows the method for the following dimension measurements: neck width (the largest cross-sectional diameter of the aneurysm neck), depth (the longest diameter between the neck and dome), width (the maximum distance vertical to depth), maximum size (the largest measurement in terms of maximum dome diameter or width), flow angle (angle between aneurysm depth vector and the vector of the centerline of the parent artery) and parent artery diameter (defined as the largest cross-sectional diameter of the artery)
Splitting aneurysms for DL model developmentTwo neuroradiologists used the Dr. Wise Multimodal Research Platform (https://keyan.Deepwise.com) to manually annotate the aneurysm contours layer-by-layer on the CTA images. First, the window width and level of the delineated CT image were adjusted to (400, 1000). The region of interest (ROI) of the aneurysm was subsequently positioned according to the aneurysm outline (Fig. 2). If there were any discrepancies, a third reader (with 25 years of experience in neuroradiology) joined the discussion to determine the final aneurysm outline. After aneurysm segmentation, all the images were randomly divided into training and internal validation sets with no duplication of data between the two sets.
Fig. 2
The image shows an aneurysm (a, arrow) and the region of interest of the aneurysm (b)
The DL modeling process includes image preprocessing, feature extraction and classification. For image preprocessing, all images of the maximum slices of the aneurysm were resized to a fixed scale of 112 × 112 for two-dimensional (2D) modeling. Then, random horizontal flip, random vertical flip and random rotation by 30 degrees were applied to increase the amount of data and improve the utilization of the training set. For model training, a residual pretrained network (ResNet-34), which is a classic convolutional neural network (CNN) model, was used. In the process of training the model, we update the parameters. To match the number of classes, the output size was changed to 2.
During training, the batch size and the initial learning rate were set to 128 and 0.001, respectively. The number of epochs for model iteration was 500. The CrossEntropyLoss function was used to calculate the loss between the model’s prediction and the real class. We used the Adam optimization algorithm to update the neural network weights iteratively. We randomly selected the initial values of the weights from a uniform distribution, and the bias was initialized to 0. To output the classification predictions, the final DLM was chosen if the model had the highest accuracy values within 500 training epochs.
Construction of different modelsSix prediction models were constructed based on three types of features (clinical, morphological and DLM output probabilities) to determine the ability of these signatures to predict the stability of aneurysms. Model A (clinical features): Several basic clinical features of the patient, such as age, gender and alcohol consumption status, were used to construct Model A to assess the stability of the aneurysm via an LR ML algorithm. Model B (morphological features): The difference between Model B and Model A is that the input variables of Model B are related to the morphological features of the aneurysms, such as their location and the size. Model C (CTA images): This model, which is based on a convolutional neural network (ResNet-34), extracts DL features from the CTA images. Model D (clinical features and Model C’s prediction probability): Clinical features and the DLM output (prediction probability) of Model C are used as inputs to Model D, which is then built via an LR algorithm. Model E (clinical and morphological features): Clinical features and morphological features are used as inputs to Model E, which is then built via an LR algorithm. Model F (clinical features, morphological features and Model C’s prediction probability): This Model F uses an LR algorithm with clinical features, morphological features and Model C output probability as inputs.
Statistical analysisStatistical analyses were performed using SPSS software (version 25.0, IBM Corp., Armonk, NY, USA) and R software (version 4.2.2; www.r-project.org). Categorical features are presented as numbers (%) and were analyzed using the chi-square test or Fisher’s exact test. Continuous features are reported as the means ± standard deviations, and the Shapiro–Wilk test was used to determine normality, followed by Student’s t-test or the Mann–Whitney U-test. Clinical and morphological features were screened via univariate and multivariate LR analyses on the basis of the training dataset. LR algorithms were used for ML modeling to assess aneurysm stability. We assessed the performance and clinical utility of the models with receiver operating characteristic (ROC) curve, area under the curve (AUC) with 95% confidence interval (CI), accuracy, sensitivity, specificity, calibration curve and clinical decision curve analyses. The Delong test was used to compare the differences in ROC curves between the different methods. A P value < 0.05 was considered to indicate statistical significance.
留言 (0)