
記住我






Clear aligners have become a popular treatment alternative for adult patients seeking an effective and esthetic alternative to traditional orthodontic appliances.[1-3] In addition to the advantages of clear aligners in providing esthetics and comfort to the patients, they enable control of the force system by utilizing planning software and advanced algorithms.[1] However, the orthodontic treatment using clear aligners is not limited to moving teeth digitally.[4] The dental movements resulting from the clear aligners are mechanical movements that release different forces depending on the severity and type of malocclusion, requiring careful pre-planning.[2-4] Improvements and innovations added to the clear aligners, most notably the optimized attachments and customized grading, have increased the precision of tooth movements and provided a wider and more efficient range of orthodontic force delivery.[1,5] Auxiliary methods, such as elastics and partial fixed appliances, contribute to applying adjunctive biomechanics, which lead to more precise control of individual tooth movements and increase the predictability of orthodontic treatment results when using clear aligners.[6]
Ackerman et al. introduced the aeronautical terms “roll, pitch, and yaw” to describe three-dimensional orthodontic problems in spatial planes.[7] With the advent of 3D records, this classification gains importance in analyzing malocclusion deviations across all planes. Much like an airplane, which can move along three planes (front/back, side-to-side, and up/down) and rotate around three axes (horizontal, axial, vertical), the dentition and jaws require a complete description of orientation in space.[7] Roll describes the tipping of the occlusal plane from side to side, pitch refers to its upward or downward tilt in the anterior or posterior regions, and yaw denotes rotation around a vertical axis.[7] These descriptors allow for a more precise analysis of midline deviations, canting, and asymmetries, especially in complex malocclusions involving unilateral Class II or III relationships and crossbites.[7] The inclusion of yaw, previously omitted due to the lack of detection in clinical records, now offers a more comprehensive approach with 3D imaging technologies.[7]
Dentoalveolar expansion is a widely used treatment for maxillary transverse deficiencies with “yaw defects” but must be approached with caution to avoid adverse biological effects.[7-10] Unintended consequences such as gingival recession, alveolar bone deformities (fenestrations and dehiscence), and root resorption have been documented.[8-10] Research suggests that the effectiveness of maxillary expansion decreases as the amount of expansion increases.[10-12] During expansion, posterior teeth undergo both tipping and bodily movement, with tooth inclination increasing proportionally to the degree of expansion.[10-12] Studies also show that many patients develop dehiscences and experience reductions in buccal bone thickness following maxillary expansion.[9,13,14] Therefore, a thorough periodontal evaluation, ideally using cone-beam computed tomography (CBCT), is crucial before initiating treatment.[13,15] CBCT is particularly useful for detecting bone and periodontal defects, especially in adult patients, allowing for better treatment planning and prevention of complications.[13,15]
This article highlights the potential of expansion using clear aligner therapy (CAT) with a precise CBCT evaluation integrated with treatment planning software. In addition, it illustrates satisfying results using an efficacious protocol and precise planning of the staging, the attachments and auxiliary means in correcting a posterior crossbite accompanied by mild crowding in an adult individual.
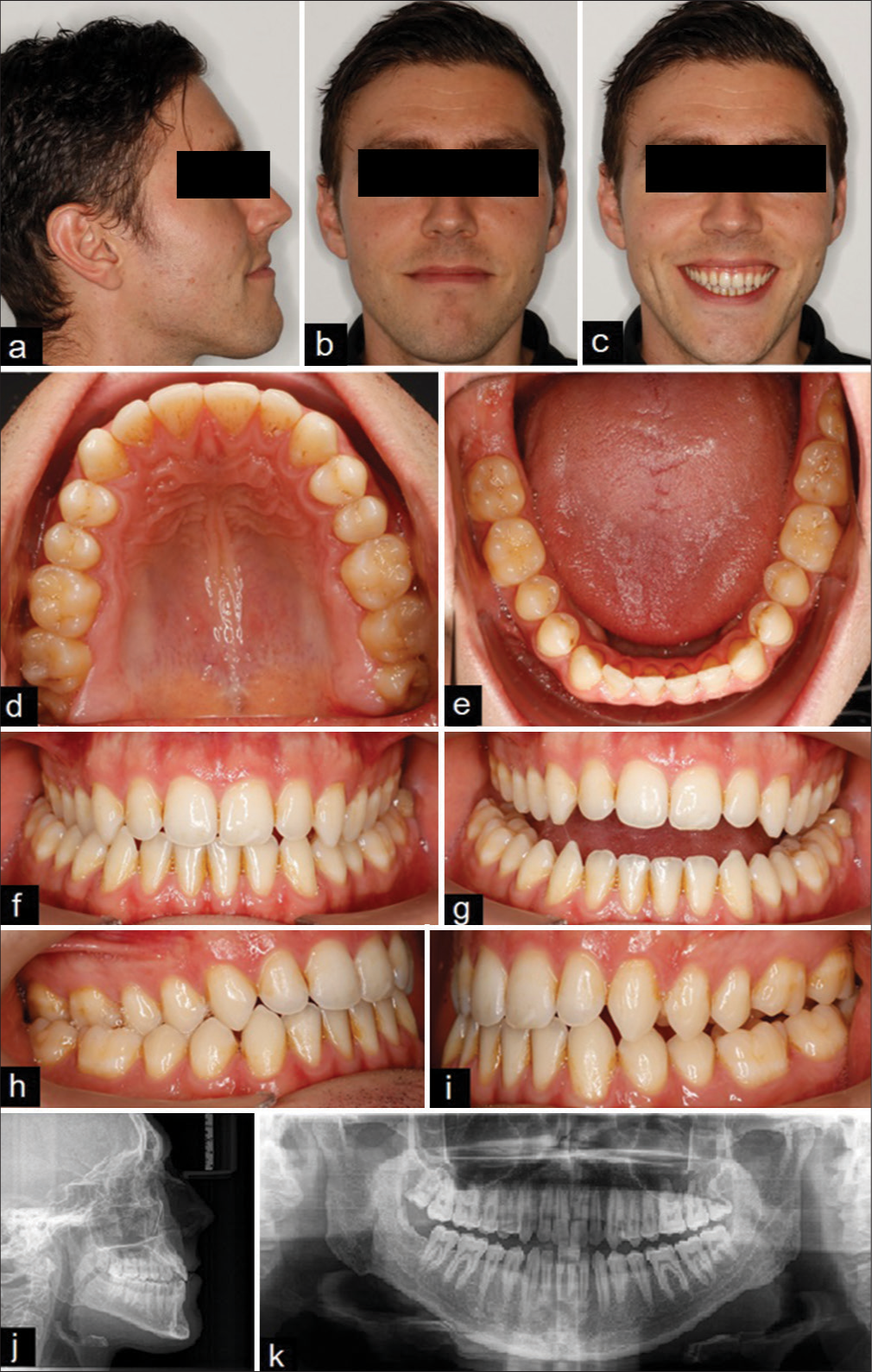
CASE REPORT Case historyA 33-year-old male patient came to the clinic with the main complaint of posterior crossbite and crowded anterior teeth. There was no family, genetic, or medical history, and the patient did not undergo any previous orthodontic treatment.
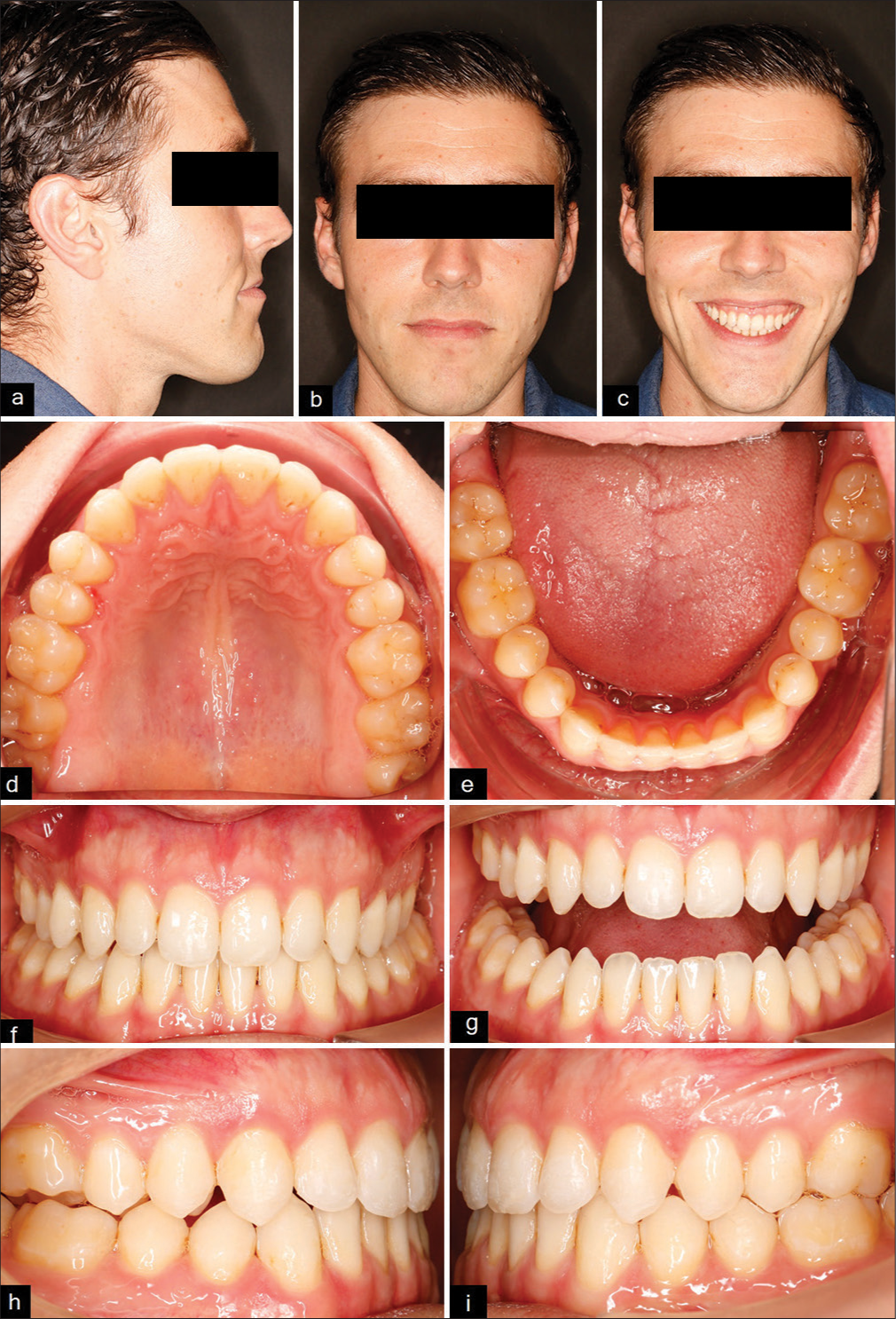
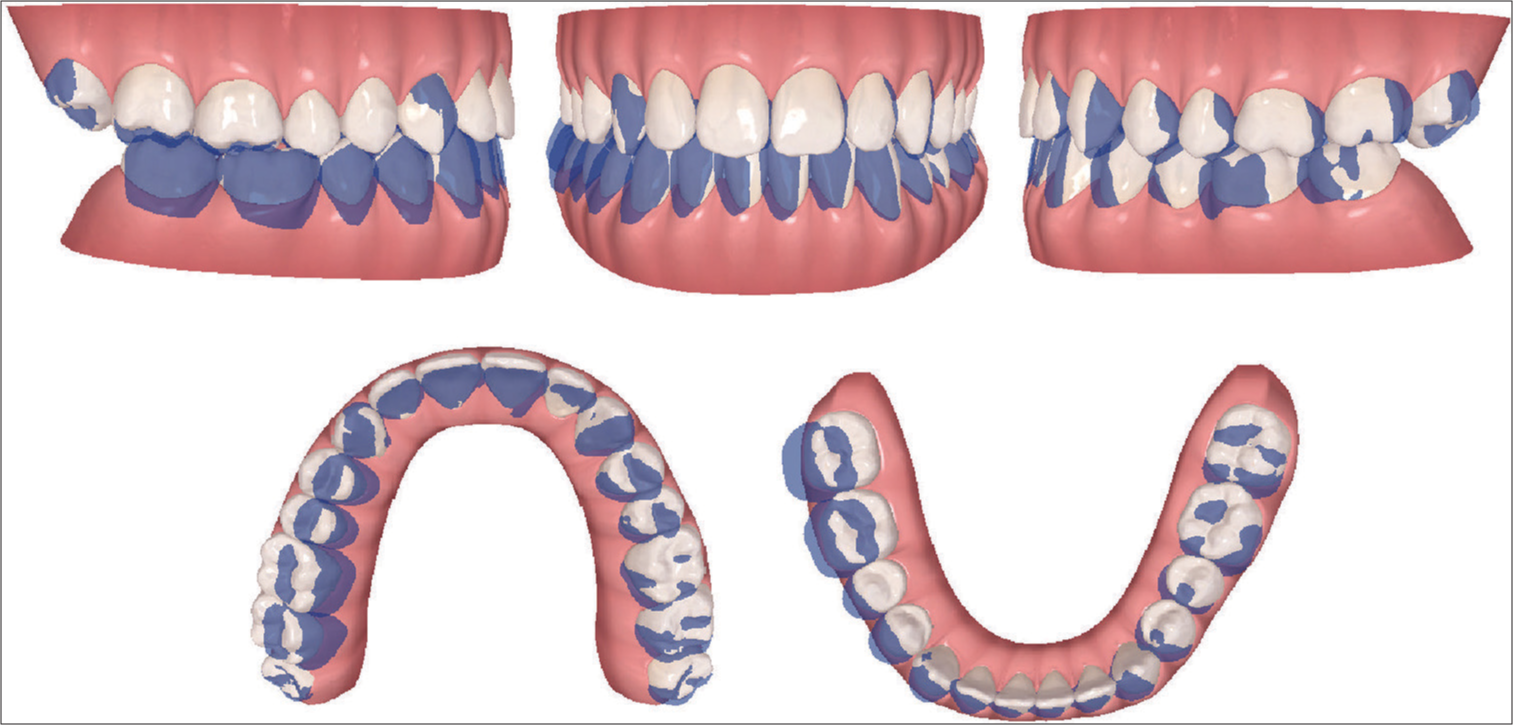
Clinical findingsExtraoral examination revealed facial symmetry with an increased lower facial third in the vertical plane. The upper dental midline coincided with the facial midline, the smile line was high with increased gingival show, and the smile arch was reversed. The profile was concave with a normal clinical the Frankfort-mandibular plane angle (FMA) and retrusive upper and lower lips. On intraoral examination, it was detected a unilateral crossbite on the right side, extending from the first premolar to the second molar, class III molar relationships, class I canine relationships, bilaterally, normal overjet of 1.4 mm; shallow overbite of 1.7 mm; and deviation of the lower dental midline from the upper one by about 2 mm to the right side. Both upper and lower arches were ovoid. Tooth size-arch length discrepancy analysis revealed a mild crowding of 1.5 mm on the upper dental arch and 1.5 mm on the lower dental arch [Figure 1]. Oral health was good, and no parafunctional habits were recorded.
Export to PPT
Radiographic diagnostic assessmentThe panoramic radiograph showed full dentition except for the right lower third molar, with no bony or periapical lesions or temporomandibular joint (TMJ) disorders [Figure 1]. Cephalometric analysis [Table 1] demonstrated a skeletal class III pattern with a negative The ANB angle is the difference between SNA (sella-nasion to A point) and SNB (sella-nasion to B point) with a slight vertical growth pattern. Dentally, the upper incisors were normally positioned, while the lower incisors were slightly retroclind with a slightly increased interincisal angle. The CBCT integrated within ClinCheck Pro 6.0 software demonstrated the possibility of posterior dentoalveolar expansion without the formation of fenestration or loss of bone support [Figure 2].
Table 1: Cephalometric analysis pre-and post-treatment.
Parameter Pre-treatment Post-treatment Skeletal 1 SNA 73 73 2 SNB 75 74 3 ANB -2 -1 4 SNPg 77 77 5 SN/FH 11 11 6 NL/NSL 8 8 7 ML/NSL 38 38 9 Bjork 402 402 Dental 10 U1-NL- ANGULAR 103 101 11 U1-NA- ANGULAR 26 22 12 L1-ML- ANGULAR 92 87 13 L1-NB-ANGULAR 29 24 14 U1/L1 127 134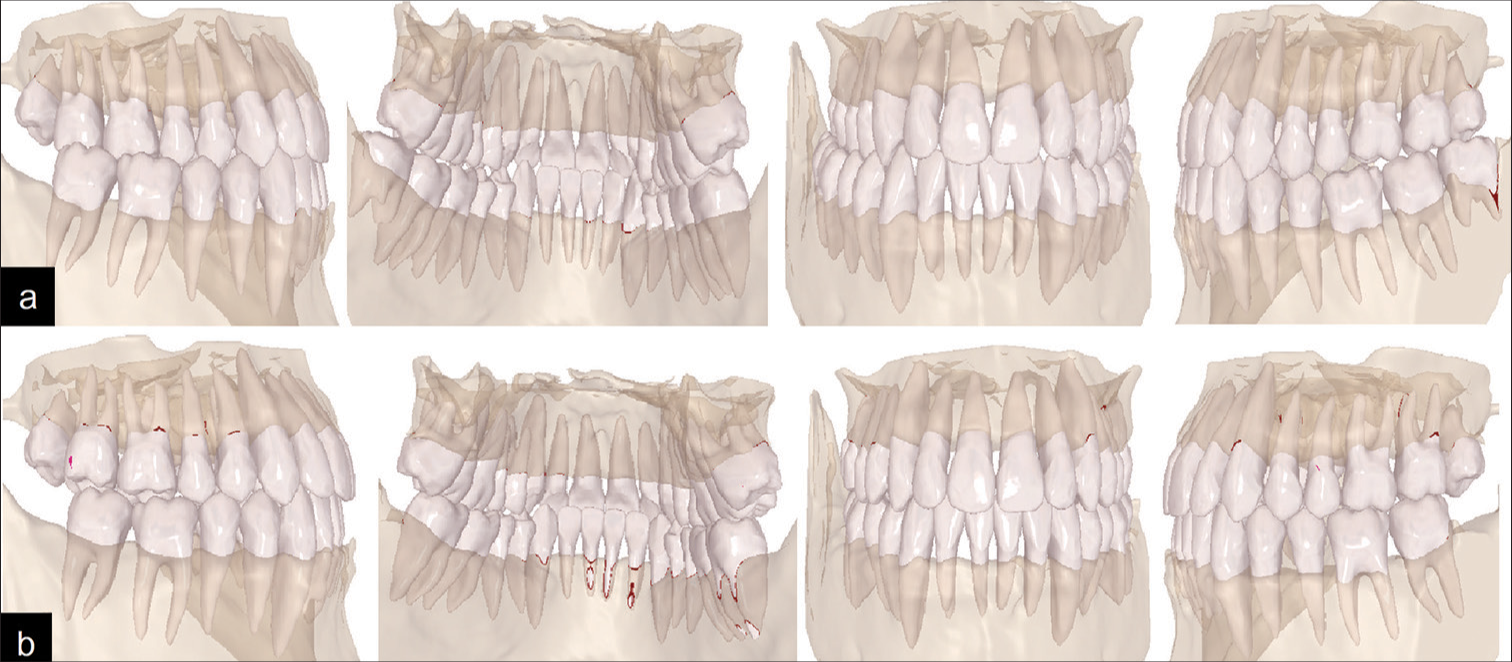
Export to PPT
Treatment objectives and treatment planThe treatment objectives included correcting the posterior crossbite, the mild crowding on both arches, the posterior open bite, and the lower midline deviation, and achieving bilateral class I canines and molars relationships with an optimal smile arch and lip line. The preferred treatment method was Invisalign aligners therapy (Align Technology Inc, Santa Clara, CA, USA). It was planned to correct the unilateral crossbite by applying cross-elastics and solve the mild crowding and the lower midline deviation by sequential distalization of the left lower teeth after extraction of the lower left third molar, aided by the application of class III intermaxillary elastics. In addition, the cant correction was planned using intra-maxillary elastics applied between two palatal and buccal mini screws on the left side of the upper jaw. All procedures were carried out in compliance with the ethical principles established in the Declaration of Helsinki.
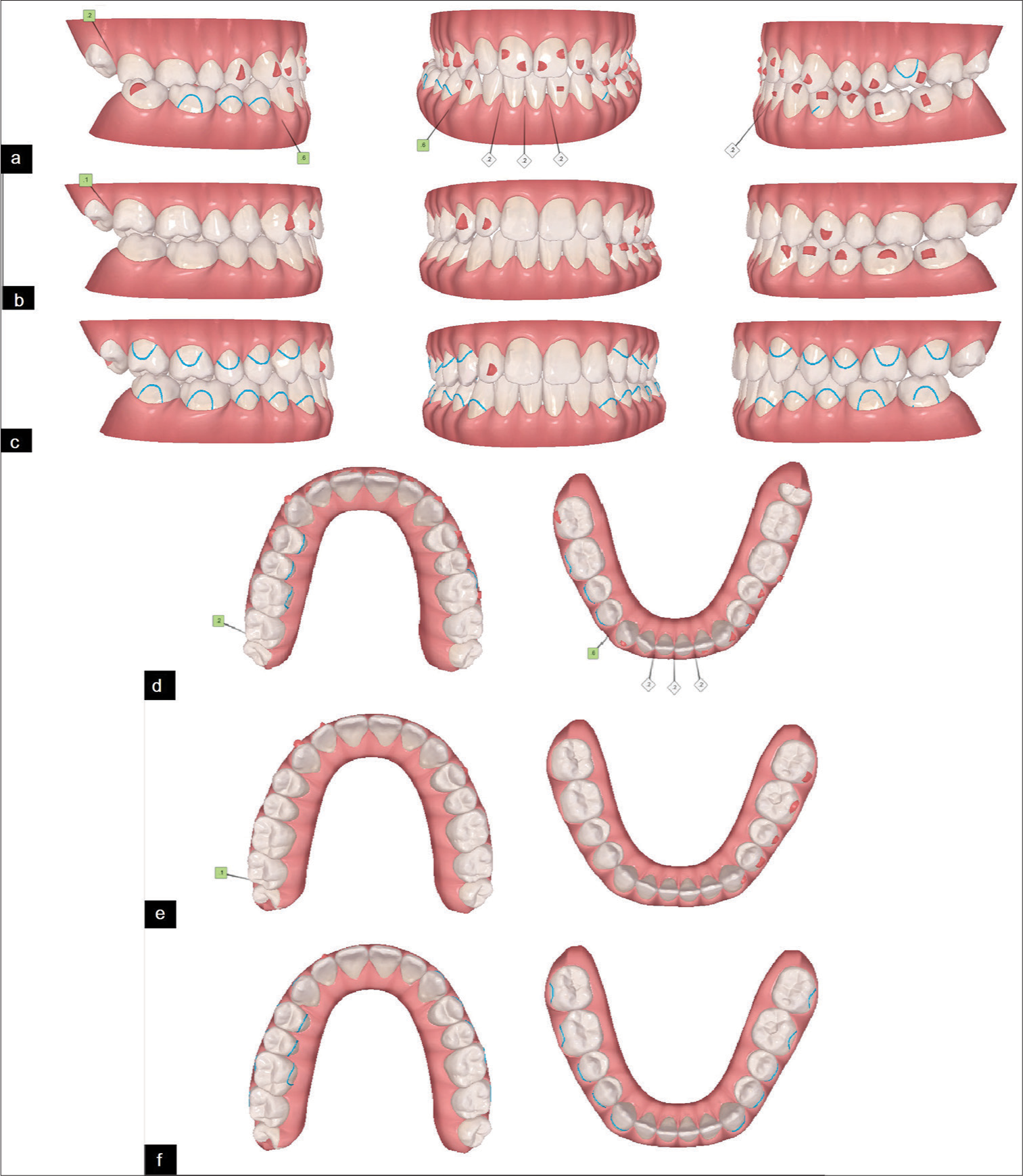
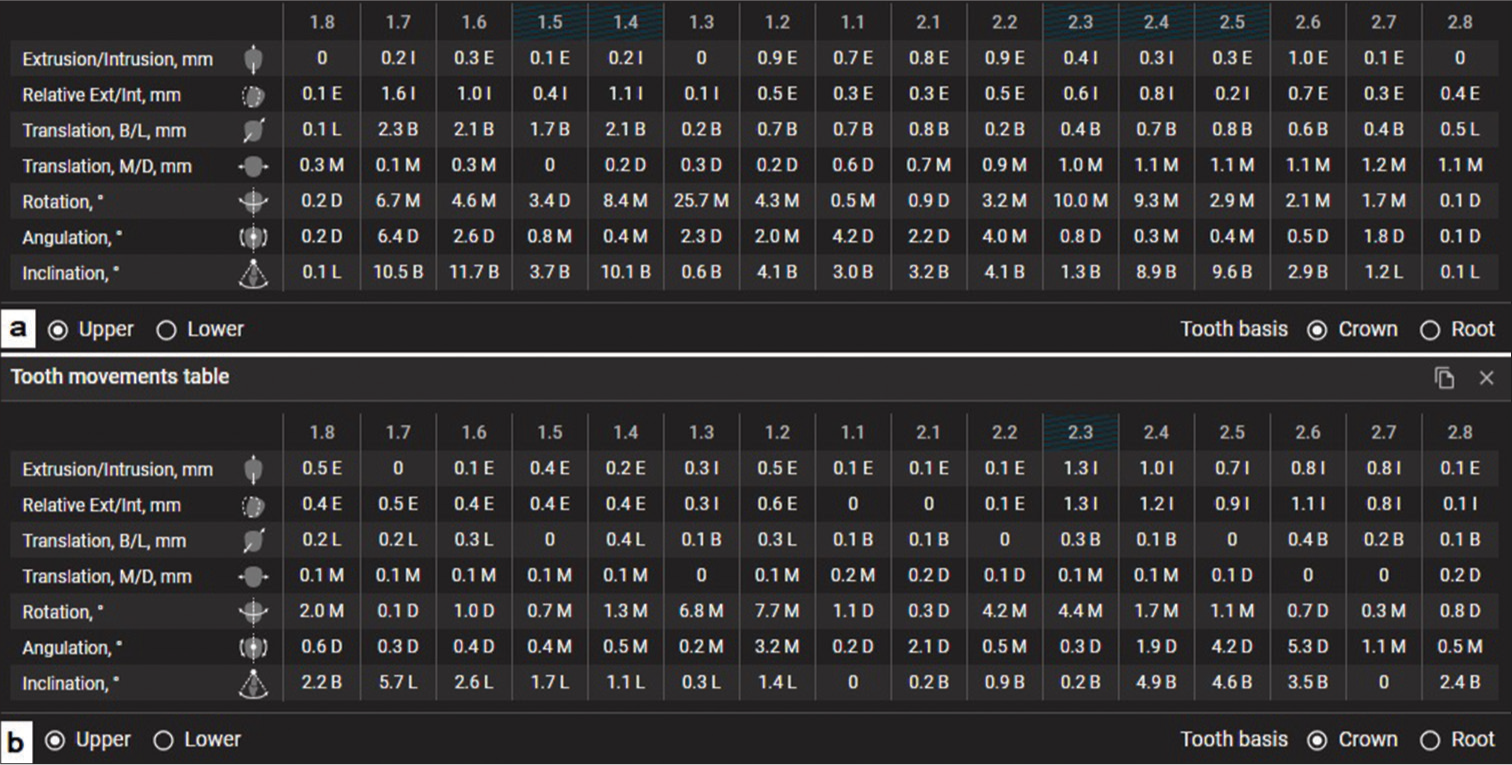
Therapeutic interventionBefore orthodontic treatment began, the patient was referred to a surgeon to extract the lower left third molar. The treatment consisted of two phases where virtual setup in both occlusion and occlusal views and the tooth movement tables are shown in [Figures 3 and 4]. The virtual setup of ClinCheck Pro 6.0 software in the first phase assumed 42 aligners per arch, where 38 aligners were used for lower molar distalization and upper molar mesialization. In the lower arch, sequential distalization of the left lower teeth and sequential mesialization of the left upper teeth were planned to correct the lower midline deviation and achieve a class I molar relationship and optimal overbite. It was planned to place optimized attachments on most teeth, with vertical 3-mm rectangular ones on the lower left molars and the left upper first molar, to achieve body movements and avoid tipping. The attachments were placed on the labial surfaces of the teeth (upper attachments: #14, #13, #12, #11, #21, #22, #23, #24, #25, #26; lower attachments: #37, #36, #35, #34, #33, #32, #43, #47). 0.2 mm interproximal enamel stripping of the anterior incisors was applied. Metal buttons were placed on the upper teeth (palatally: #16, #15, #14, buccally: #26) and on the buccal surface of the lower teeth (#46, #45, #44) [Figure 3].
Export to PPT
Export to PPT
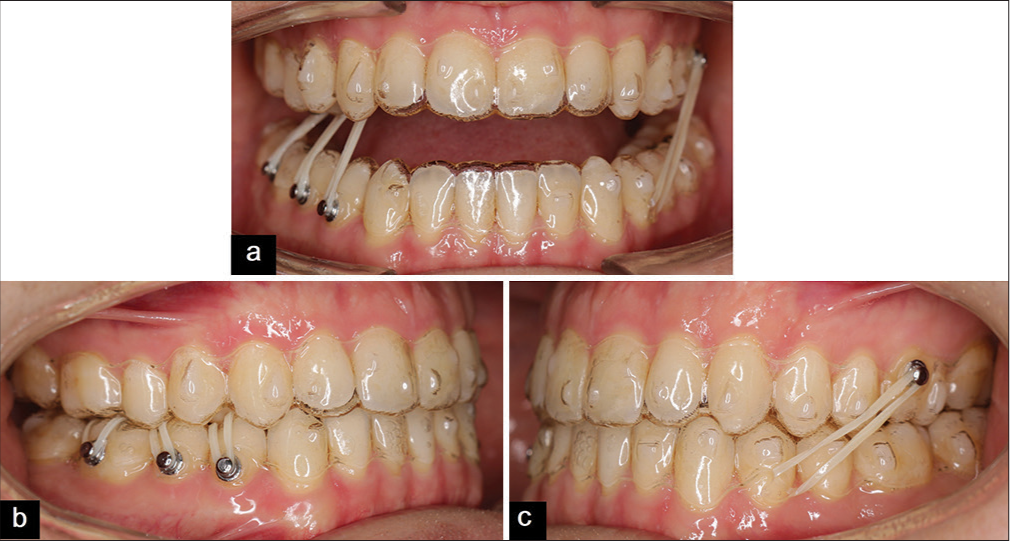
Cross-elastics (1/8 inch, medium force 4.5 oz) were used between each upper tooth (#16, #15, #14) and its corresponding lower tooth (#46, #45, #44) to correct the crossbite. In addition, class III elastics (3/16-inch, medium force 4.5 oz) were applied from a hook on the left lower canine to a button on the buccal surface of the left upper first molar to assist sequential distalization and mesialization movements [Figure 5]. Extraoral and intraoral photographs at the end of the first phase are shown in [Figure 6]. Twenty-two aligners were used in the second phase, where only 8 attachments were placed on the labial surfaces of the teeth (upper attachments: #13, #12, #24; lower attachments: #37, #36, #35, #34, #33) [Figure 3]. Two mini-screws (8 mm × 1.4 mm) were placed between the upper left canine and first premolar buccally and between the upper left first and second premolar palatally, and the patient was asked to apply 1/4 inch, medium force 4.5 oz elastic between the mini-screws to correct the occlusal canting on the left side [Figure 7]. Starting from the 14th aligners, all attachments were removed except for #12, and metal buttons were added to the labial surfaces of the teeth (upper: #17, #16, #14, #24, #25, #26; lower: #37, #36, #35, #34, #44, #46, 47) and only one button was added on the palatal surface of the tooth #27. Vertical elastics (1/8 inch, medium force 4.5 oz) were used between each upper tooth (#17, #16, #14, #24, #25, #26) and its corresponding lower tooth (#36, #35, #34, #44, #46, 47) to settle the bite. In addition, cross-elastics (1/8 inch, medium force 4.5 oz) were used between the palatal button on #27 and the buccal button on #37 to correct the crossbite. The patient was asked to wear the aligners and elastics for 22 h a day and to replace the aligners weekly.
Export to PPT
Export to PPT

Export to PPT
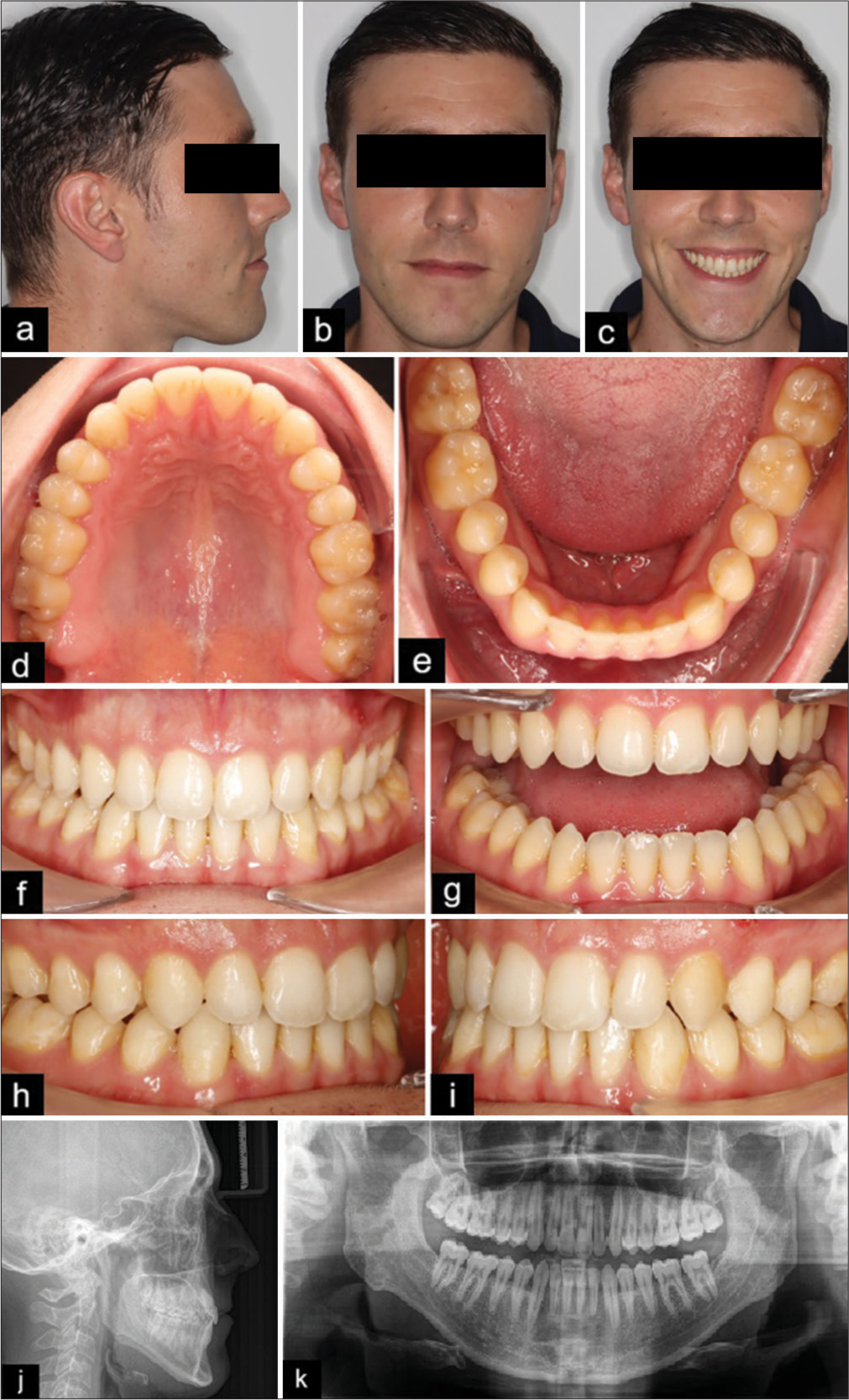
Treatment outcomes and follow-upsOverall, treatment time was 14.5 months of active treatment. The treatment was conducted in two phases. Records at the end of the treatment show that the desired objectives have been successfully achieved, as demonstrated in [Figure 8]. The unilateral expansion period was about 9.5 months and was achieved in the first phase, where 42 aligners were used as intended by ClinCheck. The patient’s smile was improved to achieve an ideal smile arc and reduced gingival exposure without occlusal canting. The intraoral records show that the upper and lower dental arches were aligned perfectly with class I relationship bilaterally and no crossbites. The overjet and overbite were satisfactory with coincident dental midlines.
Export to PPT
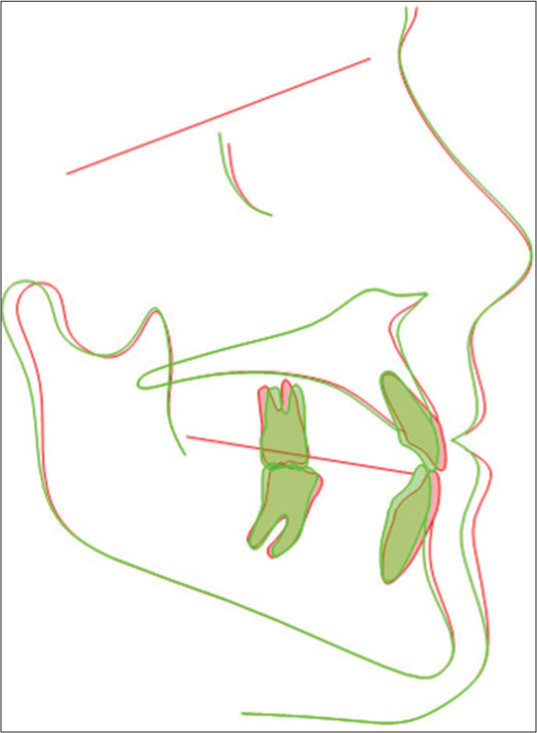
The panoramic radiograph at the end of the treatment indicated satisfactory parallelism of the roots without any noted resorption. Digital model and cephalometric superimpositions reveal the uprighting of the lower and upper molars with slight retraction of the lower incisors. There was distalization of the lower left molars with mild extrusion, mesialization of the upper left molars, lingual movements of the lower right posterior teeth, and buccal movement of the upper right posterior teeth due to the application of the cross elastics [Figures 9 and 10]. The patient did not experience or report any negative effects. The patient was very pleased with the result of the treatment and noted improved smile appearance and increased comfort while biting and chewing. The patient was provided with Vivera as removable retainers for retention, and [Figure 11] shows the follow-up intraoral records, which revealed stable treatment outcomes.
Export to PPT
Export to PPT

Export to PPT
DISCUSSIONThe current case report aims to explain the treatment of a “roll, pitch, and a yaw defect” that manifested in a unilateral crossbite, occlusal cant, and a reversed smile line. Intraorally, he presented with dental crowding in an adult patient who opted for clear aligners as an esthetic alternative treatment option to traditional braces. There is still a debate regarding the effectiveness of clear aligners in treating moderate and severe cases of malocclusion. In addition, the number of published papers on the effects of using clear aligners to perform dentoalveolar expansion is still low, as most scientific evidence is focused on the effect of traditional expanders or fixed appliances on the alveolar bone.[16-18]
In adult patients, there are numerous therapeutic techniques have been suggested in scholarly literature for treating crossbites.[10,11,16,17] CAT used for dentoalveolar expansion have been used either alone,[19] with auxiliaries such as intermaxillary elastics,[20] or in combination with some other appliances as a miniscrew-assisted rapid palatal expander.[21] Using intermaxillary elastics in conjunction with clear aligners enabled the correction of unilateral crossbite within a time frame comparable to that of the fixed appliances. This offered the patient an esthetic and comfortable treatment targeted alternative to fixed vestibular appliances.[22]
Clinical trials have shown that using clear aligners in expanding the upper dental arch created buccal tipping of the posterior teeth, extrusion, and lingual tipping of the incisors when expanding the upper dental arch.[10,23,24] The conclusions drawn by Grünheid et al. and Zhou and Guo reported that clear aligners could lead to an increase in interarch width, and the expansion was primarily accomplished through a combination of buccal bodily translation and tipping of the posterior teeth.[10,25] This report aims to underscore the importance of evaluating bone thickness before initiating expansion with clear aligners to prevent alveolar bone fenestrations and dehiscence, which can compromise periodontal health and reduce bony support. The use of CBCT integrated with ClinCheck Pro 6.0 is recommended to assess the feasibility of expansion with Invisalign aligners. In the present case, the buccal inclination of the upper right molars and first premolars ranged from 10° to 11.5°, which was optimal given the initial lingual angulation of these crowns. Conversely, the second upper premolar showed only a 3.7° buccal inclination, while the lower right first and second molars had minimal lingual inclinations of 4.2° and 1°, respectively. This highlights the critical need for pre-treatment adjustment of tooth tip and torque, based on the axis and position of the teeth, before starting orthodontic correction. Notably, no lingual inclination was observed in the upper incisors, likely due to the careful pre-planning of attachment geometry and torque compensation. Specifically, a buccal inclination of 3°–4° was incorporated into the upper incisors’ treatment plan.
According to Morales-Burruezo et al.’s study, dentoalveolar expansion was more effective in the premolar region compared to the second molar region.[20] However, in the current case, expansion proved effective in both the premolar and molar regions, with slightly greater expansion values observed in the second molar region (buccal translation: 2.3 mm, 2.1 mm, 1.7 mm, and 2.1 mm for #17, #16, #15, and #14, respectively) [Figure 2]. This observed variation can potentially be attributed to the fact that 90.4% of the patients included in the Morales-Burruezo et al.[20] study had already exhibited correct positioning of their second molars, rendering the necessity for expansion insignificant.
Distalization conducted in this case was 1.8 mm and 1.6 mm for the second and first lower left molars, respectively. These values are consistent with the average distalization measurements reported in a recent systematic review, which indicated that clear aligners were efficacious in distalizing lower molars by approximately 2–3 mm with high patient compliance rates.[26] Moreover, several articles have emphasized how staging improves the predictability of mesialization and distalization movements.[12,27-29] This strategy was also applied in a recent case to perform sequential mesialization and distalization using 38 aligners to achieve the most predictable movements. In addition, attachments were strategically placed on most teeth to improve movement control and axis alignment, enhancing the predictability of tooth movement. Various attachment designs and angulations were selected, including vertical attachments positioned on the mesial side of the lower left molars to control tipping, prevent mesial rotation, and facilitate bodily movement during distalization.
CONCLUSIONA comprehensive diagnosis is essential when determining the appropriate treatment for maxillary constriction. Evaluating the feasibility of both dentoalveolar and skeletal expansion before treatment is critical. Clear aligners, such as Invisalign, offer a viable option for addressing maxillary dentoalveolar constriction. The integration of CBCT with ClinCheck Pro 6.0 enhances diagnostic accuracy, aiding in precise treatment planning. In this case, the use of aligners demonstrated effective expansion through accurate attachment placement, auxiliary techniques, and careful staging of mesialization and distalization movements. This approach allows for the correction of complex orthodontic issues, including roll, pitch, and yaw deviations, with minimal unwanted tooth movements. Aligners with adjuncts, when smartly planned and staged, provide a predictable and efficient solution for correcting 3D non-skeletal conditions in a time frame that may be comparable to traditional braces. However, further research is necessary to refine our understanding of non-surgical expansion in non-growing adults and improve the predictability of outcomes across all three planes of space.
留言 (0)