
記住我






The pharynx is a critical structure in the human respiratory system that not only has a significant role in deglutition and respiration but also has a crucial role in the growth and development of bones of craniofacial regions.[1,2] Any abnormalities in the soft tissue and craniofacial skeleton can change the pharyngeal airway system as a result of the posterior position of the mandible or maxillary retrognathism not only induces airway insufficiency and mouth breathing but also results in downward rotation of mandible, tongue, and extension of the head.[3,4] Furthermore, an extended head position and lowered tongue posture increase the mandibular load due to stretching of facial musculature, resulting in upright incisors and narrow arches, and predominantly, such features are seen in hyperdivergent growth patterns.[5,6]
According to “soft tissue stretching hypothesis”[7,8] stated that alterations in the normal naso-respiratory processes due to stretching of soft tissues oro-pharyngeal area have an extreme impact on the craniofacial development, especially during the period of active growth when a patient approaches for orthodontic treatment.[6,9,10]
Previous studies showed that growing individuals with Class II malocclusion had a constricted pharyngeal area, mainly of the oropharynx and hypopharynx, in comparison to Class I malocclusion.[1-3,10] Furthermore, skeletal movements during orthognathic surgeries do have an effect on the surrounding structures, such as maxillo-mandibular advancement procedures that result in movement of the posterior of the tongue, soft palate, hyoid bone, and frontal pharyngeal structures anteriorly. Similarly, any mandibular setback surgeries are also associated with the narrowing of the pharyngeal space. [11,12]
Recent advancements in the field of technologies and healthcare systems, like the use of cone-beam computed tomography (CBCT), have overtaken the previous 2-D methods or procedures. These CBCT multiplanar reconstructions (MPRs) and 3D evaluations provide data that are more accurate and reduce radiation dose.[13-15]
Considering the significance of determining the morphology of the pharyngeal airway in different facial skeletal patterns and its effect on treatment planning, this study was carried out to evaluate and correlate pharyngeal airway space, mandibular morphology, and tongue volume in individuals with various skeletal classes and facial patterns.
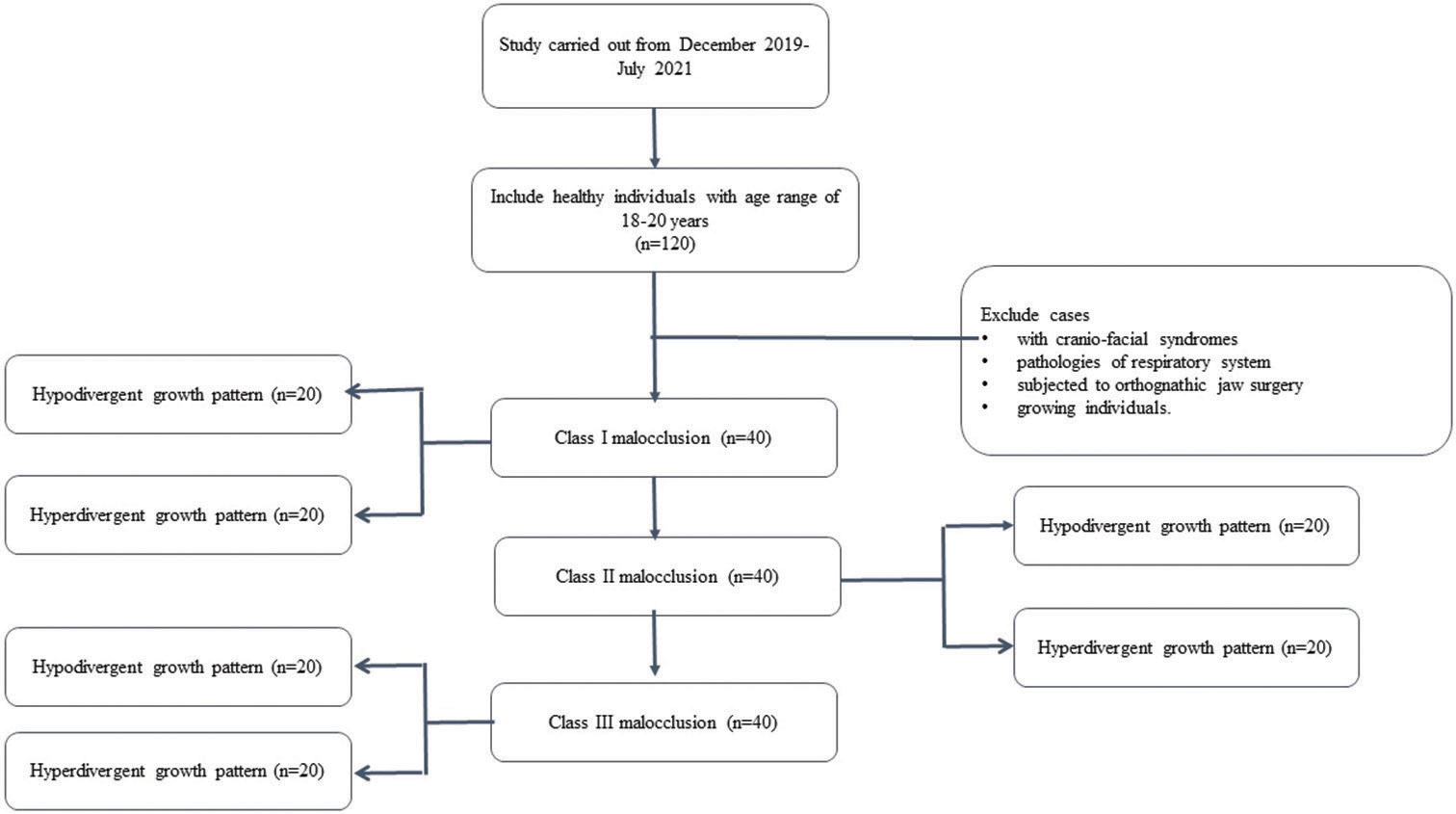
MATERIAL AND METHODS Study designA study was performed on 120 patients whose CBCT images were recruited from the Department of Orthodontics and Dentofacial Orthopaedics. The Ethical Clearance Board, Al-Badar Rural Dental College, Kalaburagi, has approved this study, with certificate number (No. IEC/2019-20/03). The study was conducted from a period between December 2019 and July 2021. With a 95% confidence level and a margin of error of ±5%, a sample size of 120 subjects was allowed in the study. The power of sample size was analyzed by the formula n = f (α/2, β) × 2 × σ2/(µ1−µ2)2 where µ1 and µ2 are mean outcomes and σ is the standard deviation allowed in the study.
Inclusion criteriaThe individuals were selected based on the inclusion criteria, i.e., healthy individuals in an age range of 18–20 years before orthodontic treatment or orthognathic surgery. The samples were classified into 3 skeletal classes: Class I, Class II, and Class III (40/group). Each class was further subdivided into two subgroups (20/subgroup) as hyperdivergent and hypodivergent, respectively as shown in Flowchart 1 below.
Export to PPT
Exclusion criteriaIndividuals of growing age or younger than 18 years
Individuals with craniofacial syndromes
Individuals subjected to orthognathic surgery and pathologies of the respiratory system like the history of enlarged adenoids or ear-throat infections and obstructive sleep apnea (OSA) (exclusion of OSA patients was on the history of the presence of at least one of the symptoms such as snoring, daytime sleepiness, choking, and nocturnal awakening and a diagnostic criterion as described by the International Classification of Sleep Disorders for OSA)[16]
ProcedureCBCT volumes were captured (Kavo 3D Pro imaging system, Palodex group OY, Finland) at 120 kV, 10mA, field of view of 13 × 15 cm, voxel size of 0.4 mm, and scanning time of 40 s. The CBCT images were acquired with every individual seated in the upright position and with the eyeear plane parallel to the floor and the teeth of the patients in the maximal intercuspal position. The pre-treatment digital lateral cephalometric images were collected (CS IMAGING TECHNIQUE CS 8100 Rochester, NY USA). Digital Images (DICOM format) were exported to FACAD software (Version 3.10.1 Swedish Company, Ilexis AB Linkoping, SWEDEN) to classify into various classes and facial patterns.
The skeletal class was determined based on ANB, SNA, and SNB angle, while the facial pattern was differentiated as hypodivergent and hyperdivergent groups by calculating the VERT index of Rickets.[17]
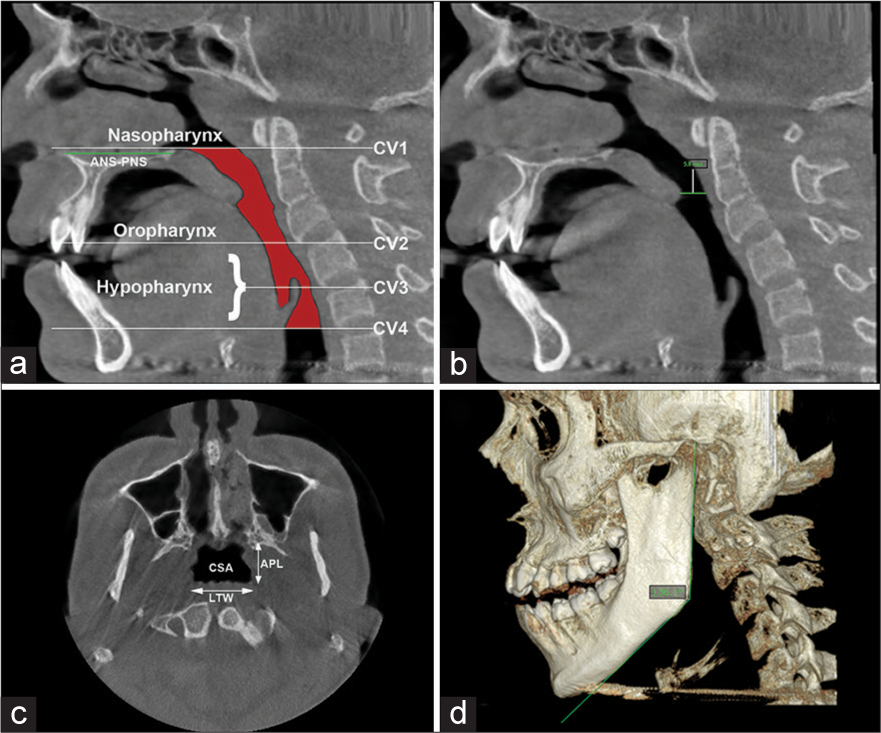
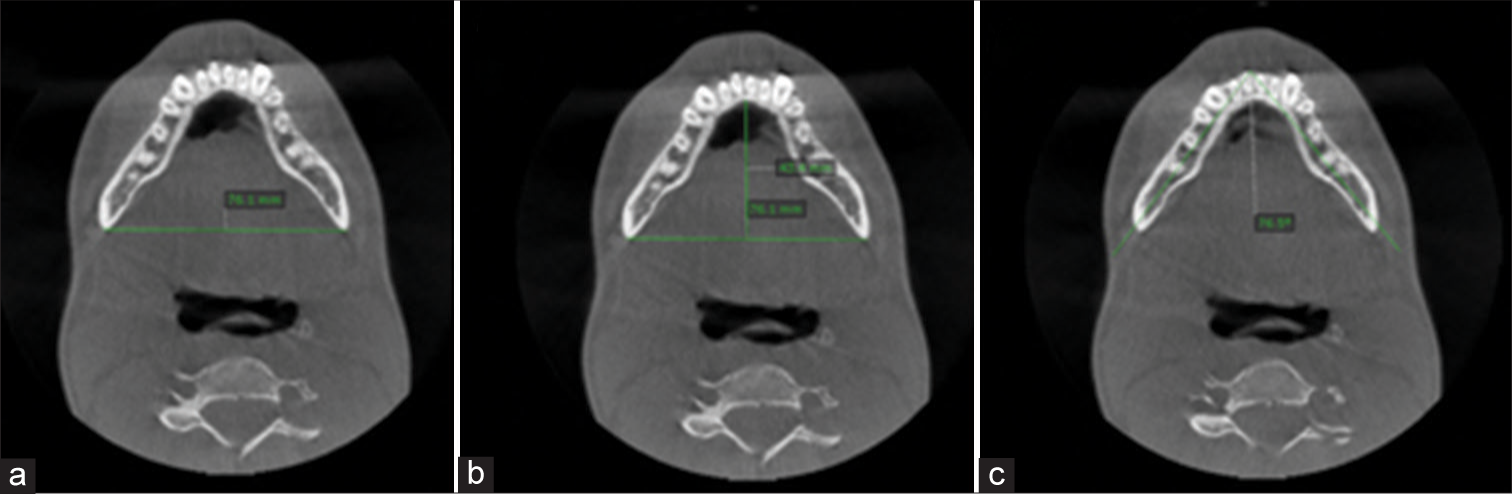
The CBCT DICOM files were transferred to on-demand 3D software (version 1.0.10.746; CybeMed, Seoul, South Korea) for conversion to volumetric 3D MPR. For pharyngeal airway analysis, the reference line vertically was placed in the median sagittal plane, and the horizontal reference line was placed from the anterior nasal spine (ANS) to the posterior nasal spine (PNS) to reconstruct in axial and sagittal planes. Considering the mandible, the horizontal reference line was placed tangent to the lower border of the mandible for reconstruction in the sagittal plane and then extended to the genial tubercle in the superior direction [Figure 1a-d].[1]
Export to PPT
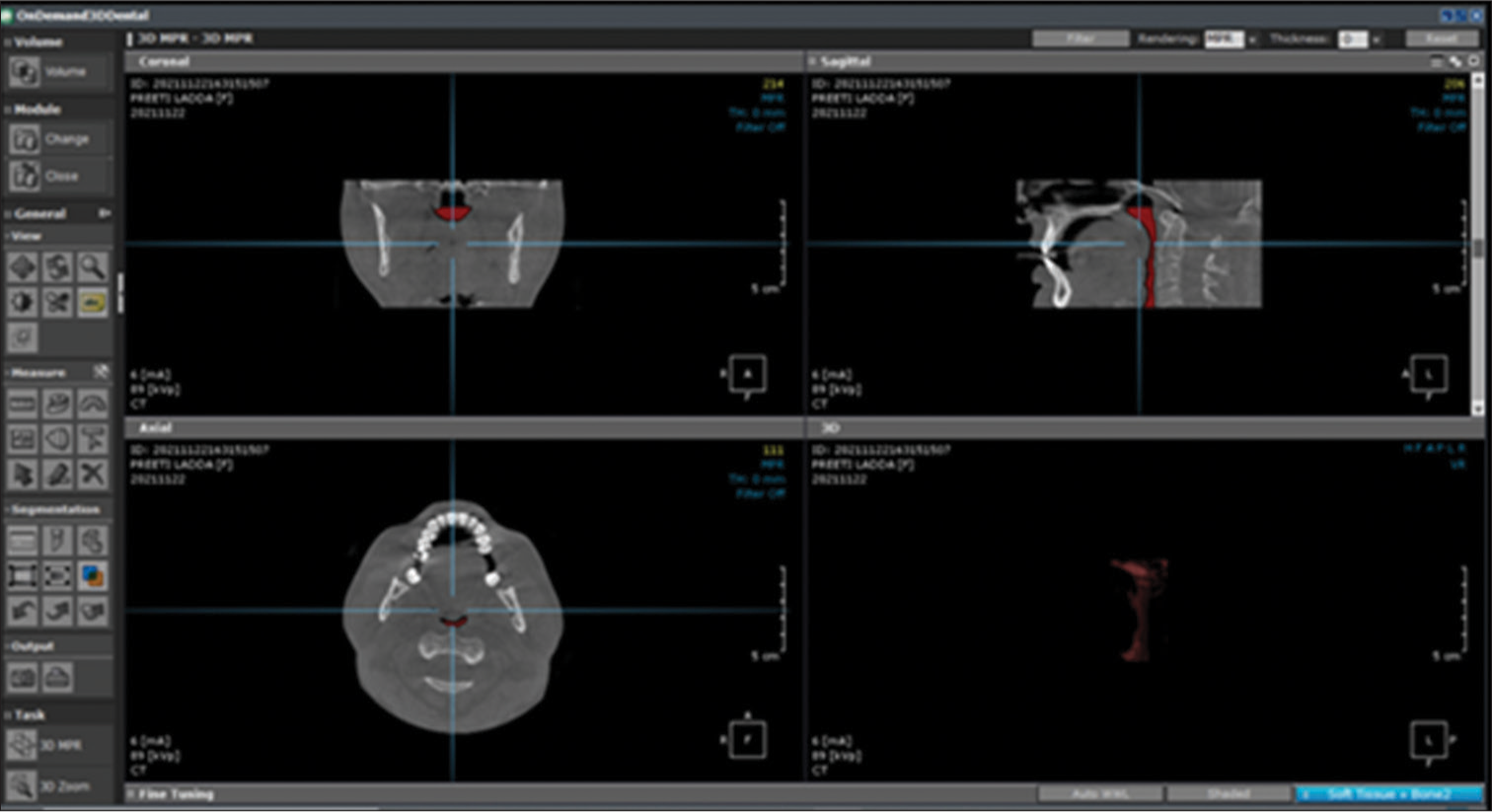
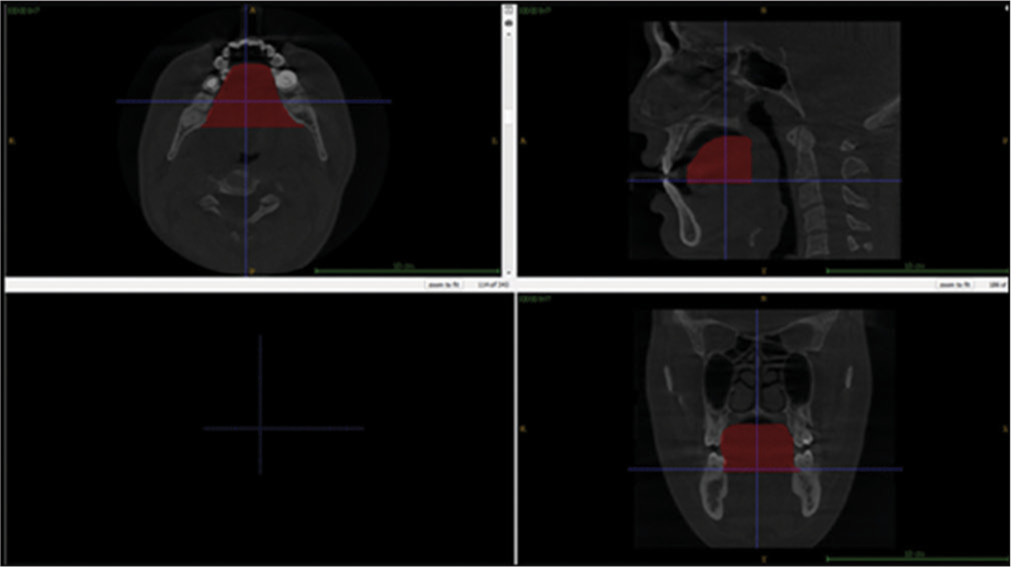
The analysis of the pharyngeal space volume (PSV) was accomplished from a 3D model. From the reconstructed 3D model, PVS was measured in mm3. PSV was evaluated by exporting the CBCT DICOM files to the ITK-SNAP software (version 3.8.0; Cognitica, Philadelphia, Pa; www.itksnap.org). From the MPR of images, the 3D models of the volume of the oropharynx and hypopharynx were reconstructed by utilizing the semi-automated segmented mode of the ITK-SNAP software.
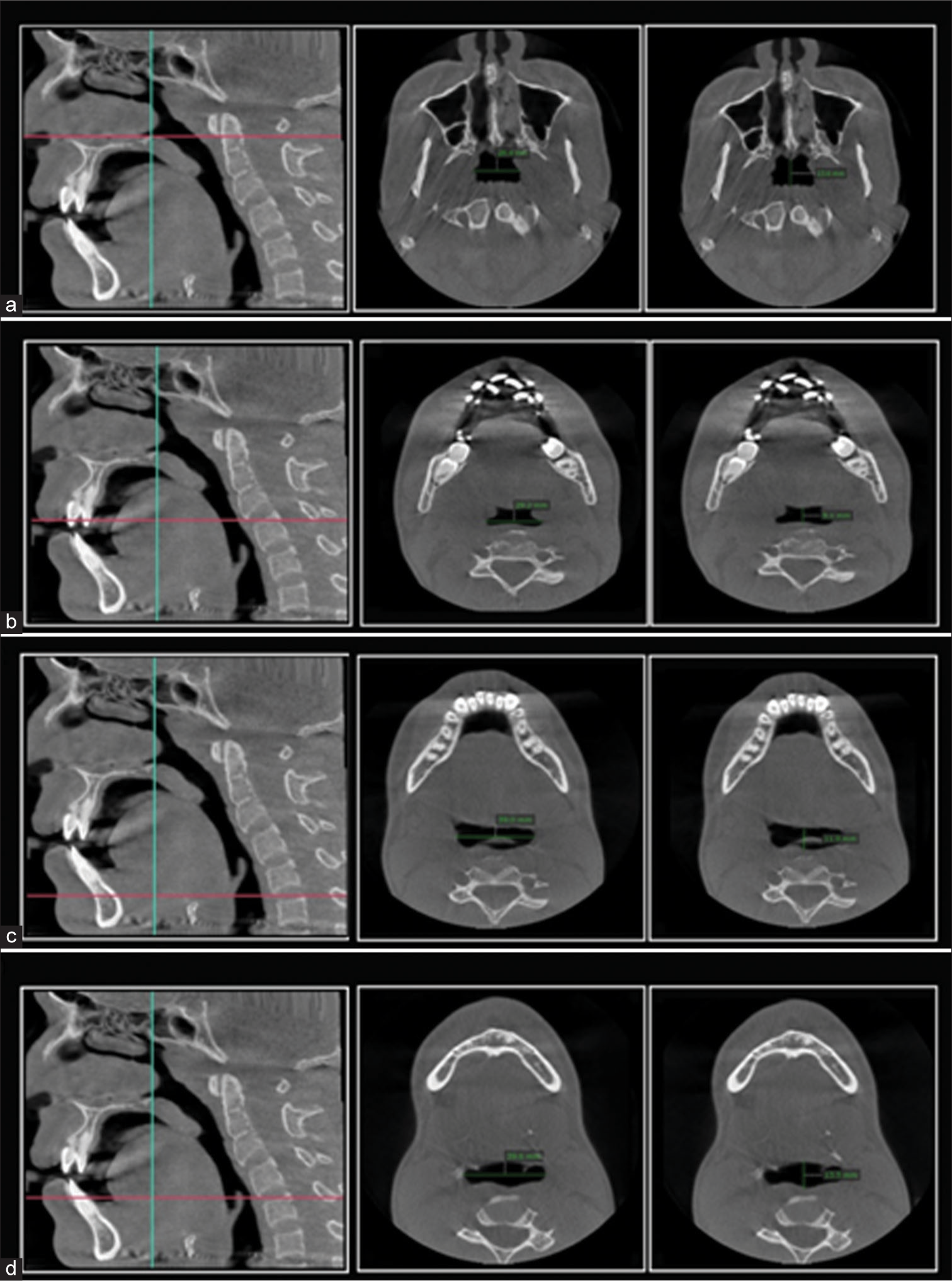
The PSV in this research relates to the fusion between the oropharynx and the hypopharynx. Thus, we established the anatomic borderline according to Park et al.,[1,18] i.e., superiorly by taking a reference line at the right angle to midsagittal plane traced from the posterior-most point of the palatal plane (ANS-PNS) to the inferior most point of the C1 (first cervical vertebra) as CV1 plane and the anterior-inferior most point of the C2 (2nd cervical vertebra) as CV2 plane, similarly, CV3 plane and CV4 plane.[1] Based on these reference planes, the upper airway is divided into the oropharynx (between the CV1 and CV2 planes) and the hypopharynx (between the CV2 and CV4 planes) [Figure 1a]. Assessments of the anatomical parameters of the upper airway were measured as the largest transverse width, anteroposterior length, and cross-sectional area on the axial plane as shown in [Figures 1c, 2 and 3]. Parametres for measurement of mandibular morphology was shown in [Figure 4].
Export to PPT
Export to PPT
Export to PPT
Boundaries to measure tongue volume were identified as the cementoenamel junction of posterior teeth (first molar and premolars) parallel to the X-axis plane both sagittally and axially, defining the ventral aspect of the tongue for segmentation. A plane at the right angle from the PNS in the axial orientation is defined to form the posterior aspect of the tongue for segmentation on the axial view. The occlusal plane was defined from the central cusps of the lower first molar to the incisal edge of the incisors for volume analysis, as shown in [Figure 5].
Export to PPT
As the tongue is a soft tissue, for each patient, Hounsfield values (−650–200 HU) were set to calculate the maximum amount of voxel. According to the Hounsfield values chosen initially, the above-defined borders for the tongue were then added to form a three-dimensional mask of the volume of the tongue.
Volumetric analysis of the tongue was determined by utilizing the voxel volume from the scan and the number of voxels taken for a specific mask. To rule out inter-investigator variance, the same investigator determined all the parameters 2 times with a 1-week interval. To determine the reproducibility of the measured parameters, the intra-class correlation coefficient was calculated.[19]
The parameters analyzed are represented in [Tables 1 and 2].
Table 1: Parameters for pharyngeal airway analysis.
Parameters Definition of Parameters Reconstructed plane Pharyngeal space dimensions ANS to PNS distance [Figure 1a] Linear distance from the anterior most to posterior most point on the palatal plane. Sagittal Constricted distance [Figure 2b] Linear distance from the narrowest area of pharyngeal space horizontally Sagittal Intrerspace at C1 (lateral to lateral [LLC1]) [Figure 2a] Linear distance horizontally from the greatest lateral to lateral measurement of pharyngeal space situated at the lowermost point at C1 Axial Interspace at C1 anterioposteriorly (APC1)[Figure 2a] Linear distance vertically from the greatest measurement anterioposteriorly of pharyngeal space situated at the lowermost point at C1 Axial Interspace at C2 (lateral to lateral [LLC2]) [Figure 2b] Linear distance in horizontal direction from the greatest laterallateral measurement of pharyngeal space situated at the lowermost point at C2 Axial Interspace at C2 anterioposteriorly (APC2) [Figure 2b] Linear distance vertically from the greatest measurement anterioposteriorly of pharyngeal space situated at the lowermost point at C2 Axial Interspace at C3 (lateral to lateral [LLC3]) [Figure 2c] Linear distance horizontally from the greatest lateral to lateral measurement of pharyngeal space situated at the lowermost point at C3 Axial Interspace at C3 anterioposteriorly [APC3][Figure 2c] Linear distance vertically from the greatest measurement anterioposteriorly of pharyngeal space situated at the lowermost point at C3 Axial Interspace at epiglottis (lateral to lateral [Epiglotiss-LL]) [Figure 2d] Linear distance horizontally from the greatest lateral to lateral measurement of pharyngeal space situated at the point of maximum concavity of the stalk of the epiglottis. Axial Interspace at epiglottisanterioposteriorly (Epiglottis-AP) [Figure 2d] Linear distance vertically from the greatest measurement anterioposteriorly of pharyngeal space situated at the point of maximum concavity of stalk of the epiglottis. AxialTable 2: Parameters for mandibular morphology and tongue volume analysis.
Gonial angle [Figure 1d] Angular measurement between the line from condylion to gonion and the line tangent to lower border of the mandible. Sagittal Interdistance of mandible (LL) [Figure 4a] Linear distance from the point of one gonion to the point of contralateral gonion. Axial Sagittal distance of mandible (AP) [Figure 4b] Vertical line from the anterior most point on the lingual aspect of the mandibular symphysis to a line between both sides of the gonion points Axial Transverse mandibular angle. [Figure 4c] Angular measurement between the anterior most point on the mental protuberance and the gonion point on both sides of the mandible. Axial Tongue volume (mm3) [Figure 5] Segmentation of the tongue on the ventral aspect: e cervical margin of mandibular posterior teeth will be rotated on the sagittal view in such a manner that the above plane will be parallel to the xaxis planeThe Statistical software IBM Statistical Package for the Social Sciences 20.0 (IBM Corporation, Armonk, NY, USA) was utilized for data analysis. Analysis of variance, unpaired t-test, and Tukey test were used to evaluate and comparison of facial patterns and skeletal classes. Pearson correlation test was done to determine the correlations between the PSV and the other variables. The level of significance was kept at 0.05.
RESULTSThe intra-examiner intraclass correlation showed values between 0.76 and 0.97 for the angular measurements. The distribution of skeletal Classes is shown in [Table 3]. There were statistically significant differences in all the measured variables (P < 0.001) except for the gonial angle of the mandible, which showed statistically insignificant with P = 0.675.
Table 3: Comparison of different variables in terms of (Mean±[SD]) among skeletal classes using ANOVA test.
Variables Class I (n=40) Class II (n=40) Class III (n=40) P-value ANS_PNS 46.250±2.0142 47.100±2.0295 44.835±1.8556 <0.001** Constricted distance 6.485±1.6084 5.660±0.9432 7.315±1.3975 <0.001** C1-LL 24.700±3.5141 20.090±3.6382 27.355±1.5457 <0.001** C1-AP 8.995±3.0739 7.275±1.9390 10.925±2.1857 <0.001** C2-LL 22.655±5.2095 19.420±3.5395 28.485±2.0807 <0.001** C2-AP 7.065±1.9128 7.485±1.1360 9.940±1.9701 <0.001** C3-LL 26.850±3.1011 23.740±1.5602 30.190±1.4293 <0.001** C3-AP 9.130±1.9620 7.955±1.5377 10.370±1.5881 <0.001** Epiglottis-LL 27.300±1.8453 24.765±1.2475 33.015±3.4038 <0.001** Epiglottis-AP 10.195±1.3062 8.380±1.4162 11.545±1.5536 <0.001** Airway volume 8119.6600±561.20097 5991.2075±1689.89360 11140.0700±1386.48827 <0.001** Gonial angle 124.800±8.8729 125.650±8.5472 126.550±9.0155 0.675 Transverse mandibular angle 62.585±0.7701 63.010±0.9703 61.660±1.2868 <0.001** Inter-distance of mandible 82.375±1.0655 83.455±0.3336 84.400±0.6854 <0.001** AP-mandible distance 57.365±0.7866 58.000±0.4961 60.620±1.5119 <0.001** Tongue volume 42962.235±926.5525 39251.695±1996.3261 50073.750±1609.6806 <0.001**The distribution of variables in different facial types, which showed highly significant differences (P < 0.001) while tongue volume showed a statistically significant difference at P < 0.05 whereas ANS-PNS, C1-LL distance, C1-AP distance, LL distance of mandible, and AP distance of mandible showed no statistically significant differences (P < 0.05) with P = 0.223, 0.067, 0.123, 0.475, and 0.37, respectively is showed in [Table 4].
Table 4: Comparison of different variables in terms of (Mean±[SD]) between both facial types using unpaired t-test.
Variables Hypodivergent (n=60) Hyperdivergent (n=60) P-value ANS_PNS 46.303±2.1762 45.820±2.1450 0.223 Constricted distance 7.323±1.4480 5.650±0.9986 <0.001** C1-LL 24.763±5.1156 23.333±3.0994 0.067 C1-AP 9.467±3.0788 8.663±2.5696 0.123 C2-LL 25.317±4.4267 21.723±5.6159 <0.001** C2-AP 8.780±2.3715 7.547±1.6461 <0.001** C3-LL 27.933±3.2024 25.920±3.3330 <0.001** C3-AP 10.053±1.8063 8.250±1.6840 <0.001** Epiglottis-LL 29.973±4.6182 26.747±2.9208 <0.001** Epiglottis-AP 10.760±1.9557 9.320±1.6094 <0.001** Airway volume 9417.8640±2163.30421 7416.0943±2392.86501 <0.001** Gonial angle 117.433±3.1642 133.900±2.6852 <0.001** Transverse mandibular angle 61.710±0.9360 63.127±0.9264 <0.001** Inter-distance of mandible 83.483±0.9603 83.337±1.2624 0.475 AP-mandible distance 58.800±1.9162 58.523±1.5520 0.387 Tongue volume (mm3) 44969.263±4677.6871 43222.523±4742.3647 0.044*As shown in [Table 5], a significant correlation was found between the PSV and the measured variables. In both facial types, the correlation between the parameter’s airway volume and ANS-PNS shows a negative correlation and is statistically significant for P < 0.001 for the hypodivergent pattern (−0.456).
Table 5: Correlation between airway volume and all other variables, segmented in groups (facial types or skeletal classes).
Airway volume Total Class I Class II Class III Hypo divergent Hyper divergent ANSPNS Pearson correlation −0.289** −0.080 0.338* 0.103 −0.456** −0.287* Sig. (2-tailed) 0.001 0.622 0.033 0.528 0.000 0.026 n 120 40 40 40 60 60 Constricted t distance Pearson correlation 0.583** 0.248 0.382* 0.726** 0.585** 0.349** Sig. (2-tailed) 0.000 0.123 0.015 0.000 0.000 0.006 n 120 40 40 40 60 60 C1LL Pearson correlation 0.645** 0.214 0.093 0.474** 0.545** 0.852** Sig. (2-tailed) 0.000 0.185 0.569 0.002 0.000 0.000 n 120 40 40 40 60 60 C1AP Pearson correlation 0.526** 0.188 0.381* 0.039 0.405** 0.650** Sig. (2-tailed) 0.000 0.245 0.015 0.811 0.001 0.000 n 120 40 40 40 60 60 C2LL Pearson correlation 0.726** 0.579** 0.658** −0.179 0.468** 0.843** Sig. (2-tailed) 0.000 0.000 0.000 0.268 0.000 0.000 n 120 40 40 40 60 60 C2AP Pearson correlation 0.557** 0.411** 0.009 0.560** 0.682** 0.299* Sig. (2tailed) 0.000 0.009 0.955 0.000 0.000 0.020 n 120 40 40 40 60 60 C3LL Pearson correlation 0.764** 0.331* 0.618** 0.231 0.614** 0.845** Sig. (2-tailed) 0.000 0.037 0.000 0.151 0.000 0.000 n 120 40 40 40 60 60 C3AP Pearson correlation 0.623** 0.584** 0.397* 0.545** 0.492** 0.587** Sig. (2-tailed) 0.000 0.000 0.011 0.000 0.000 0.000 n 120 40 40 40 60 60 EpiglottisLL Pearson correlation 0.897** 0.663** 0.471** 0.939** 0.959** 0.843** Sig. (2-tailed) 0.000 0.000 0.002 0.000 0.000 0.000 n 120 40 40 40 60 60 EpiglottisLL Pearson correlation 0.740** 0.449** 0.407** 0.556** 0.643** 0.764** Sig. (2-tailed) 0.000 0.004 0.009 0.000 0.000 0.000 n 120 40 40 40 60 60 Gonial angle Pearson correlation −0.356** −0.560** −0.912** −0.839** 0.040 0.130 Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.762 0.322 n 120 40 40 40 60 60 Transverse angle of mandible Pearson correlation −0.696** −0.409** −0.771** −0.605** −0.706** −0.542** Sig. (2-tailed) 0.000 0.009 0.000 0.000 0.000 0.000 n 120 40 40 40 60 60 Interdistance of mandible Pearson correlation 0.351** 0.180 0.082 −0.157 0.519** 0.244 Sig. (2-tailed) 0.000 0.266 0.614 0.333 0.000 0.060 N 120 40 40 40 60 60 AP distance of mandible Pearson correlation 0.586** 0.070 −0.399* 0.250 0.781** 0.429** Sig. (2-tailed) 0.000 0.670 0.011 0.120 0.000 0.001 N 120 40 40 40 60 60 Tongue volume Pearson correlation 0.948** 0.027 0.921** 0.931** 0.984** 0.964** Sig. (2-tailed) 0.000 0.869 0.000 0.000 0.000 0.000 n 120 40 40 40 60 60In class III hypodivergent, the correlation between the airway volume and shortest distance (0.726, 0.585, respectively) shows a very good positive correlation and is significant with a P < 0.001. Correlation between the airway volume and transverse angle of the mandible shows excellent negative correlation (−0.409, −0.771, −0.605, −0.706, −0.542, respectively) for class II and class III skeletal classes and both facial types and is statistically significant for P < 0.001.
The correlation between the parameters airway volume and tongue volume (0.921, 0.931, 0.984, and 0.964, respectively) shows an excellent positive correlation and is significant with a P < 0.001 for class II and class III skeletal pattern and in both facial types.
The results of the intergroup comparison of skeletal classes with hypodivergent growth pattern are shown in [Table 6], and all variables showed statistically significant differences (P < 0.001), the following variables showed significantly higher values for the shortest/constricted distance (8.420 ± 0.5307), C1-LL (28.130 ± 0.7935), C1-AP (10.960 ± 1.5581), C2-LL (27.980 ± 1.9509), C2-AP (10.960 ± 2.0423), C3-LL (30.450 ± 1.0566), C3-AP (11.080 ± 1.7392), epiglottis-LL (35.550 ± 3.0050), epiglottis-AP (12.390 ± 1.5), airway volume (12310.140 ± 858.6), gonial angle (118.0 ± 2.15), inter-distance of the mandible (84.320 ± 0.69), and tongue volume (51271.300 ± 1104.7) in Class III in comparison with class I and class II.
Table 6: The measured variables of hypodivergent skeletal pattern (Class I, Class II, Class III) using one-way ANOVA.
Variables Class I Class II Class III Intergroup comparison** Mean SD Mean SD Mean SD ANS_PNS 46.000 2.4675 47.800 1.7205 45.110 1.3054 Class II>Class I>Class III Constricted distance 7.400 1.6053 6.150 0.9649 8.420 0.5307 Class III>Class I>Class II C1-LL 25.900 4.5229 20.260 5.0534 28.130 0.7935 Class III>Class I>Class II C1-AP 9.690 3.8850 7.750 2.5320 10.960 1.5581 Class III>Class I>Class II C2-LL 26.650 4.4595 21.320 3.317 27.980 1.9509 Class III>Class I>Class II C2-AP 8.020 1.8266 7.360 1.4912 10.960 2.0423 Class III>Class I>Class II C3-LL 28.610 3.4153 24.740 1.0870 30.450 1.0566 Class III>Class I>Class II C3-AP 10.330 1.3479 8.750 1.5206 11.080 1.7392 Class III>Class I>Class II Epiglottis-LL 28.930 0.6914 25.440 1.0976 35.550 3.0050 Class III>Class I>Class II Epiglottis-AP 10.810 1.2736 9.080 1.4215 12.390 1.5697 Class III>Class I>Class II Airway volume 8443.9700 98.21981 7499.4820 327.84472 12310.1400 858.68245 Class III>Class I>Class II Gonial angle 116.700 4.4260 117.600 2.4366 118.000 2.1521 Class III>Class II>Class I Transverse mandibular angle 62.030 0.4256 62.300 0.7211 60.800 0.8208 Class II>Class I>Class III Inter-distance mandible 87.680 0.9243 83.450 0.3753 84.320 0.6971 Class I>Class III>Class II AP-distance mandible 57.440 0.8586 57.820 0.6254 61.040 1.5198 Class III>Class II>Class I Tongue volume 42674.700 1057.3285 40961.790 1163.5743 51271.300 1104.7493 Class III>Class I>Class IIANS-PNS (47.8 ± 1.7205) and transverse mandibular angle (62.300 ± 0.7211) showed significantly higher values in Class II compared to Class I and Class III in the hypodivergent growth pattern. Interdistance of the mandible (87.680 ± 0.92) showed significantly higher values for class I compared to class II and class III hypodivergent patterns.
As shown in [Table 7], comparison of skeletal classes with hyperdivergent growth pattern showed statistically higher values for shortest distance, C1-LL, C1-AP, C2-LL, C2-AP, C3-LL, C3-AP, epiglottis-LL, epiglottis-AP, airway volume, and tongue volume in class III compared to class I and class II. ANS-PNS, transverse mandibular angle, and AP mandibular distance showed significantly higher values in class II in comparison with class I and class III. AP-mandible distance showed significantly higher values for class I in comparison with class III and class II.
Table 7: The measured variables of hyperdivergent skeletal pattern (Class I, Class II, Class III) using one-way ANOVA.
Variables Class I Class II Class III Intergroup comparison** Mean SD Mean SD Mean SD ANS_PNS 46.400 1.4517 46.500 2.1126 44.560 2.2814 Class II>Class I>Class III Constricted distance 5.570 0.9852 5.170 0.6242 6.210 1.7355 Class III>Class I>Class II C1-LL 23.500 1.3634 19.920 1.2539 26.580 1.7350 Class III>Class I>Class II C1-AP 8.300 108122 6.800 0.9119 10.890 2.7198 Class III>Class I>Class II C2-LL 18.660 1.4898 17.520 2.6667 28.990 2.1317 Class III>Class I>Class II C2-AP 6.110 1.5012 7.610 0.6265 8.920 1.2672 Class III>Class II>Class I C3-LL 25.090 1.2468 22.740 1.3076 29.930 1.7131 Class III>Class I>Class II C3-AP 7.930 1.7472 7.160 1.1004 9.660 1.0445 Class III>Class I>Class II Epiglottis-LL 25.670 0.9581 24.090 1.0151 30.480 1.1058 Class III>Class I>Class II Epiglottis-AP 9.580 1.0411 7.680 1.0319 10.700 0.9937 Class III>Class I>Class II Airway volume 7795.3500 644.51288 4482.9330 982.37185 9970.0000 571.22730 Class III>Class I>Class II Gonial angle 132.900 1.9708 133.700 2.7549 135.100 2.8819 Class III>Class II>Class I Transverse mandibular angle 63.140 0.6227 63.720 0.5926 62.520 1.0807 Class II>Class I>Class III Inter-distance Mandible 82.707 1.1314 83.460 0.3500 84.480 0.6818 Class III>Class II>Class I AP-distance Mandible 87.190 0.6843 58.180 0.2142 60.200 1.4179 Class I>Class III>Class II Tongue volume 43249.770 685.6996 37541.600 818.4130 48876.200 1038.6684 Class III>Class I>Class II The simple linear regression equation resulted in the formulaPSV = 67.362 + (23.5 × LLC2) - (14.2 × constricted distance) - (21 × APC3) + (65.4 × inter-distance of mandible) - (38.8 × LLC1) + (20.8 × LL epiglottis) + (35.2 × APC1) + (9.391 × ANS-PNS distance) - (34.164 × LLC3).
The addition of further variables, namely age, sex, skeletal class, or facial pattern, did not refine the equation as shown in [Table 8].
Table 8: The best (analysis of variance, F=187.195; P<0.0001) linear regression equation for airway volume.
Variables Unstandardized coefficients Standardized Coefficients t Sig. B Std. Error Beta (Constant) 67.362 5555.303 0.012 0.990 ANS_PNS 9.391 27.043 0.008 0.347 0.729 Constricted distance −14.288 52.319 −0.009 −0.273 0.785 C1-LL −38.892 19.113 −0.067 −2.035 0.044 C1-AP 35.269 26.046 0.041 1.354 0.179 C2-LL 23.518 15.765 0.051 1.492 0.139 C3-LL −34.164 26.301 −0.047 −1.299 0.197 C3-AP −21.003 53.789 −0.017 −0.390 0.697 Epiglottis-LL 20.898 33.177 0.035 0.630 0.530 Inter-distance of mandible 65.459 58.830 0.046 1.113 0.268 DISCUSSIONThe influence of respiration on the growth of craniofacial structure and its significance in treatment planning has been a controversial topic in the field of orthodontics.[2,7,20] Previous studies have stated that abnormal development of the maxilla-mandibular structures can result in modification of the pharyngeal airway volume, which could lead to changes in soft and hard tissue structures like hyoid bone.[21-23]
Previous study has reported that pharyngeal tissues exhibit growth till the age of 13 years.[10] Most of the longitudinal studies have reported that the muscular palate increases in height and depth between 20 and 50 years. [10,24] Many investigators have utilized lateral cephalometric analysis to evaluate the pharyngeal airway space, identifying the definite hard and soft-tissue landmarks. A major disadvantage is that it lacks accurate description and characteristics of pharyngeal airway space. In this study, we used 3D CBCT imaging technology, which helped us to understand and visualize the 3D airway volume in a better way.[25] Previous studies have reported adaptations in the PSV, such as extended or forwarded head posture, skeletal classes, and facial patterns[26-28], while few authors have assessed the pharyngeal volume in different skeletal classes, although the consequence was questionable.[
留言 (0)