
記住我
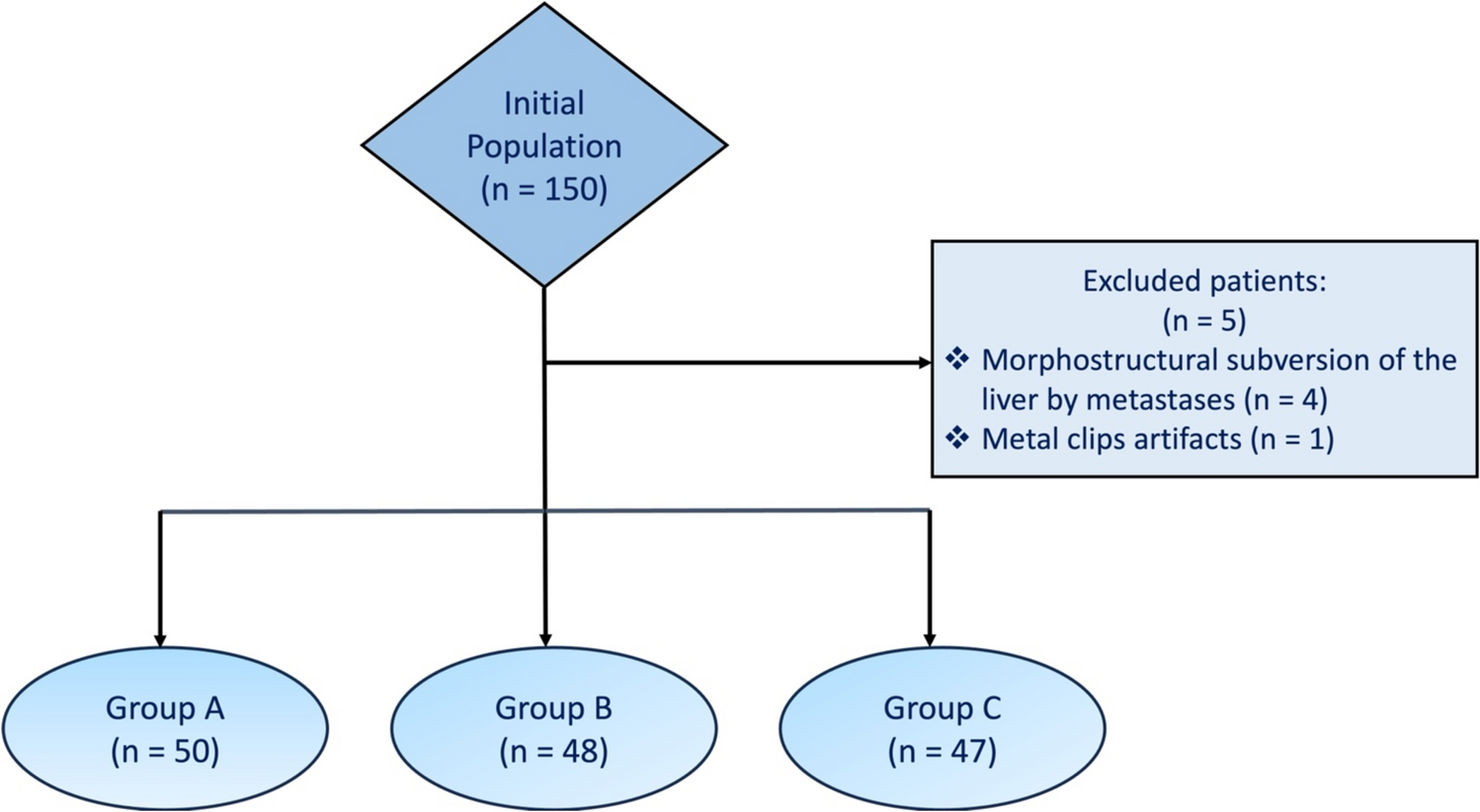





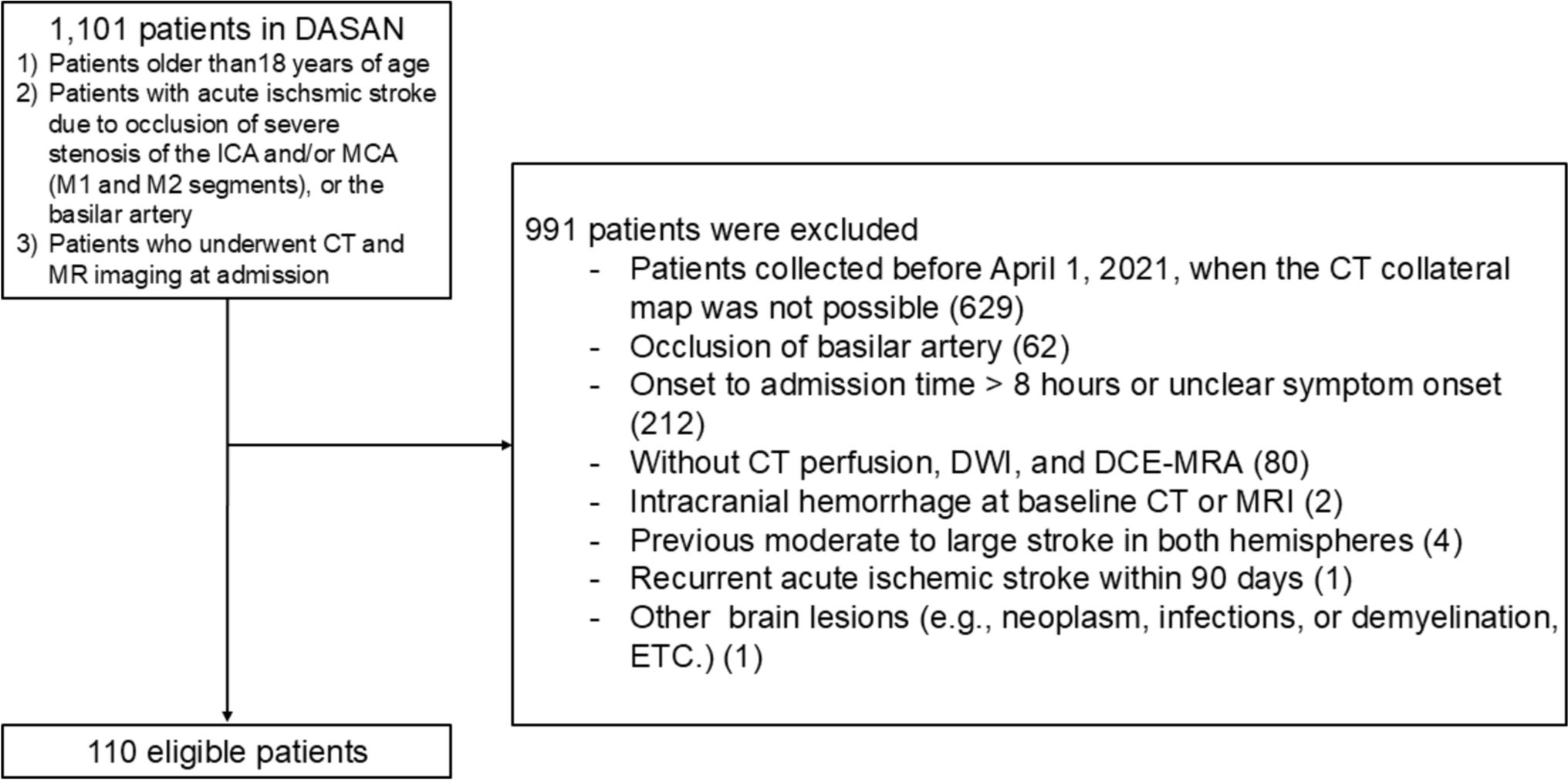
From the 68 patients enrolled in the clinical trial, 28 (41.2%) did not have target lesions separate from lesions treated by locoregional therapies and 3 (4.4%) had no follow-up CT or MRI available. A total of 37 patients were included (7 females, 30 males). A flowchart of the study is presented in Fig. 1. 28/37 (75.7%) patients were diagnosed with hepatocellular carcinoma and 9/37 (24.3%) patients with biliary cancer (8 cholangiocarcinoma, 1 ampullary carcinoma). The median age was 64 years (IQR 56–68). 22/37 (59.5%) patients had extrahepatic disease. All patients received tremelimumab, and 6/37 (16.2%) received durvalumab. Locoregional treatment included cryoablations (7/37, 18.9%), microwave ablations (10/37, 27%), radiofrequency ablations (7/37, 18.9%), transarterial chemoembolization (11/37, 29.7%), and combinations of ablation and transarterial chemoembolization (2/37, 5.4%).
Fig. 1
34/37 (91.9%) patients underwent multiphase CT scans with contrast injection. 3/37 (8.1%) patients had renal insufficiency or failure and underwent enhanced MRI. Tumors were segmented in the phase in which they were subjectively perceived to be most visible by the reviewing radiologist. For most of the patients (30/37, 81.1%), tumors were segmented on portal-phase imaging, but for 7/37 (18.9%) patients, tumors were segmented on arterial phase images.
All patients together, median PFS according to RECIST 1.1 was 147 days (IQR 98–230). In the subgroup of patients with HCC, median PFS was 238 days (IQR 142–314 days). In the subgroup of patients with biliary cancer, median PFS was 100 days (IQR 84-NA). All patients together, median OS was 301 days (IQR 221–525). In the subgroup of patients with HCC, median OS was 329 days (IQR 286–561). In the subgroup of patients with biliary cancer, median survival was 231 days (IQR 183-NA). The patient characteristics are presented in Table 1. Out of the 37 patients, 3 patients did not have a 6-month follow-up CT (2 had died, 1 was out of the study and did not have an imaging).
Table 1 Patient characteristicsConventional response evaluationAt the 6-month follow-up, according to RECIST 1.1, 18/34 (52.9%) patients had a progressive disease, 15/34 (44.1%) had a stable disease and 1/34 (2.9%) patient had a partial response. According to iRECIST, 13/34 (38.2%) had progressive disease, 5/34 (1.5%) had unconfirmed progressive disease, 15/34 (44.1%) had stable disease and 1/34 (2.9%) had a partial response. Disease control at 6-month follow-up according to RECIST 1.1 was associated with better survival (p = 0.01). Inter-reader agreement with a second reading for RECIST 1.1 was considered substantial (Cohen’s Kappa = 0.61).
Shape analysisSegmented target tumors at baseline included liver tumors (25/37, 67.6%), lymphadenopathy (7/37, 18.9%), adrenal metastasis (1/37, 2.7%), lung metastasis (1/37, 2.7%), peritoneal nodule (1/37, 2.7%), spleen metastasis (1/37, 2.7%) and bone metastasis (1/37, 2.7%). One hundred one tumor segmentations were analyzed (37 at baseline, 31 at 3-month follow-up and 33 at 6-month follow-up). Figure 2 presents examples of tumor shapes, with different circularity and solidity. Median circularity was 0.835 (IQR 0.751–0.877) at baseline, 0.828 (IQR 0.775–0.867) at 3-month follow-up and 0.815 (IQR 0.697–0.853) at 6-month follow-up. Median solidity was 0.958 (IQR 0.936–0.969) at baseline, 0.957 (IQR 0.943–0.969) at 3-month follow-up and 0.955 (IQR 0.918–0.969) at 6-month follow-up. Circularity changed over time (p = 0.04), but there was no difference in solidity over time (p = 0.16). Figure 3 presents four representative cases of shape evolution from baseline to 6-month follow-up.
Fig. 2
Example tumors with varying degrees of circularity and solidity. Tumor shapes were manually segmented on axial CT images (red line). Circularity \(\left( }} \right)}^\)) and solidity (area/convex hull area of tumor) were calculated using ImageJ
Fig. 3
Four representatives cases showing the evolution of tumor shape between baseline (left) and 6-month follow-up (right). Tumors were manually segmented on axial CT images (red line). The two upper cases, (A–D) are tumors with stable or increasing solidity and circularity. The two lower cases, (E–H) are tumors with decreasing solidity and circularity (becoming more irregular and less circular tumors). Hepatocellular carcinoma (A, B) solidity: 0.96 then 0.97, and circularity 0.88 then 0.86. Adrenal metastasis of a hepatocellular carcinoma (C, D) solidity: 0.98 then 0.99 and circularity: 0.86 then 0.93. Cholangiocarcinoma (E, F) solidity: 0.95 then 0.82 and circularity: 0.76 then 0.58. Cholangiocarcinoma (G, H) solidity: 0.93 then 0.91 and circularity 0.80 then 0.64.
Shape variation according to RECIST 1.1No correlation was found between RECIST 1.1 status at 6-month follow-up and circularity variation (p = 0.27) or solidity variation (p = 0.25), or between RECIST 1.1 status at 6-month follow-up and circularity (p = 0.15) or solidity (p = 0.07) at 6-month follow-up. Waterfall plot for target solidity variations, according to RECIST 1.1 status at 6-month follow-up is presented in Fig. 4. No correlation was found between size variation at 6-month follow-up and circularity variation (p = 0.44) or solidity variation (p = 0.30); or between size variation at 6-month follow-up and circularity (p = 0.84) or solidity (p = 0.57) at 6-month follow -up.
Fig. 4
Waterfall plot for target lesion solidity variation according to RECIST 1.1 status at 6-month follow-up. No correlation between circularity variation and RECIST 1.1 status was found
Survival analysisPatients with low solidity tumors at 6-month follow-up showed poorer prognosis compared with patients with high solidity tumors at 6-month follow-up (p = 0.01). Figure 5 illustrates the survival analysis according to solidity at 6-month follow-up. The optimal threshold for solidity according to maximally selected rank statistics at 6-month follow-up was a solidity of < 0.956. Median survival was 304 days (95% CI 230–403) for patients with low solidity tumors at 6-month follow-up and 525 days (95% CI 269-NA) for patients with high solidity tumors at 6-month follow-up.
Fig. 5
Survival analysis according to solidity of target at 6-month follow-up
Solidity variation analysis confirmed that a decrease of tumor solidity (increasing irregularity) at 6-month follow-up was associated with poorer prognosis (p = 0.01). Figure 6 shows Kaplan–Meier curves according to solidity variation at 6-month follow-up.
Fig. 6
Survival analysis according to target solidity variation between baseline and 6-month follow-up. Patient with tumor becoming more irregular, or having a decreasing solidity, between baseline and 6-month follow-up, showed poorer prognosis than patients with tumor becoming more regular, or having an increasing solidity (p = 0.01)
No association was found between shape features at baseline and overall survival, or between shape features at 3-month follow-up and overall survival (solidity, p = 0.3; circularity, p = 0.15). No association was found between circularity at 6-month follow-up and overall survival (p = 0.18).
Patients with irregular tumor, or low solidity, at 6-month follow-up have poorer prognosis than patients with more regular tumor, or higher solidity at 6-month follow-up (p = 0.01).
留言 (0)