
記住我








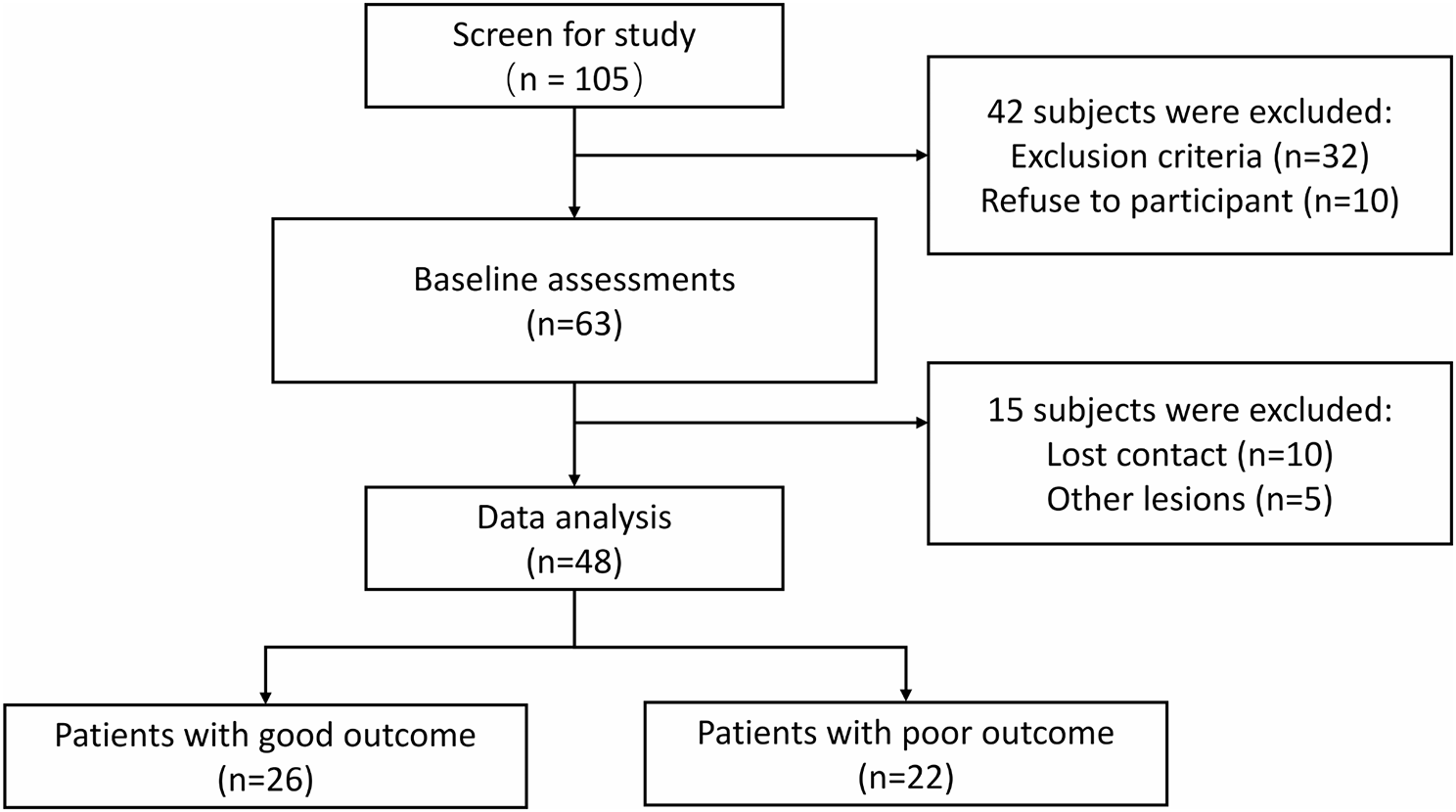
Of the 105 stroke patients, we excluded 42 patients and enrolled 63 patients. Among the 63 patients, 10 lost contacts after discharge, and another 5 had other lesions in MRI data (e.g. small vessel disease signs, meningioma, or ventricular enlargement). We therefore included 48 patients (77%) in the outcome analysis, comprising 37 men and 11 women with a mean age of 59.3 ± 12.4 years (Fig. 1). Among them, 26 patients showed improved motor function (MRS ≤ 2, good-recovery), while 22 exhibited no significant change (MRS > 2, poor-recovery) (Fig. 1).
Fig. 1
Flowchart for patient inclusion and exclusion
Table 1 presents an overview of the clinical characteristics of enrolled patients. Among them, 40 had ischemic stroke, while 8 had hemorrhagic stroke. The total follow-up period ranged from 30 to 45 days, with an average of 36.8 days (± 7.1). All EEG recordings were obtained within 6 weeks, with a mean time of 24.3 days (± 14.5) post-stroke onset.
Upon admission, the NIHSS score for neurological impairment was 5.1 (± 2.4) across all patients. Remarkably, significant variations in NIHSS scores were observed among different prognostic groups (p = 0.000). Similar intergroup disparities were noted in cognitive function (MMSE and MoCA) and self-care ability (p = 0.012, p = 0.002, p = 0.000, respectively). Nevertheless, no significant differences were detected between the groups in age, gender, lesion location, lesion volume, cerebrovascular disease risk factors, or lifestyle.
Working memory performanceOne-way ANOVA revealed a significant group effect on reaction time (F2, 69 = 6.04, P = 0.004). Post-hoc comparisons indicated longer reaction time in patients of poor-recovery (Mean = 899.29) compared to those of good-recovery (Mean = 749.84, Pcorrected = 0.034), and to healthy controls (Mean = 703.68, Pcorrected = 0.004) (Fig. 2b). There was no difference in reaction time between patients of good-recovery and healthy controls (Pcorrected > 0.5).
Fig. 2
Working memory task and performances. a) An example of non-target and target stimulus. b) Results of reaction time. Patients with poor recovery had longer reaction time compared to those with good recovery and healthy controls. There was no difference between patients with good-recovery and healthy controls. c). Results of d prime sensitivity. Healthy controls had higher d prime sensitivity compared to patients with good recovery and to those with poor recovery. There was no difference between patients with good recovery and with poor recovery (Pcorrected > 0.5). * denotes p < 0.05, ** denotes p < 0.01
In terms of d prime sensitivity, One-way ANOVA also revealed a significant group effect (F2, 69 = 4.68, P = 0.012). Post-hoc comparisons indicated higher d prime sensitivity in healthy controls (Mean = 189.56) compared to patients of good-recovery (Mean = 120.22, Pcorrected = 0.048) and to those of poor-recovery (Mean = 107.89, Pcorrected = 0.020) (Fig. 2c). There was no difference in d prime sensitivity between patients of good-recovery and of poor-recovery (Pcorrected > 0.5).
EEG oscillationIn the three datasets, the number of channels was rejected were 2.43 ± 0.53 (poor-recovery), 2.25 ± 0.46 (good-recovery), and 2.17 ± 0.45 (healthy control), respectively. The number of epochs were 76.95 ± 2.68 (poor-recovery), 76.50 ± 3.13 (good-recovery), and 76.79 ± 3.59 (healthy control), respectively.
Cluster-based permutation tests revealed a beta inhibition in the central regions in each group compared to baseline (healthy controls: Pcorrected = 0.004, time range = 0.17–0.73 s; good-recovery: Pcorrected = 0.003, time range = 0.22–0.81 s; poor-recovery: Pcorrected = 0.000, time range = 0.20–0.97 s) (Fig. 3a-c). A list of significant electrodes was listed here. healthy controls: C4, CP1, CP2, CP6, P3; good-recovery: FC1, FC2, C3, C4, CP5, CP1, CP2; poor-recovery: FC5, FC1, C3, C4, CP5, CP1, CP6, P3, P4.
Fig. 3
Event-related changes from baseline. a-c) All three groups demonstrated a decrease in beta power in the central regions (healthy controls: Pcorrected = 0.004, time range = 0.17–0.73 s; good-recovery: Pcorrected = 0.003, time range = 0.22–0.81 s; poor-recovery: Pcorrected = 0.000, time range = 0.20–0.97 s). There was also an increased late beta power in the frontal and parieto-occipital regions in the healthy controls and patients of good-recovery (healthy controls: Pcorrected = 0.000, time range = 0.88–1.80 s; good-recovery: Pcorrected = 0.014, time range = 1.33–1.78 s). This pattern of beta oscillation was not significant in patients with poor recovery (Pcorrected > 0.05). Tagged electrodes in each topolot indicated the significant channels revealed by cluster statistics. The time-frequency representations were plotted with the significant electrodes in the topoplot of (c), or the shared significant electrodes in the two topoplots in (a, b). X denotes p < 0.05. * denotes p < 0.01, dB = decibel
In addition to beta inhibition, there was also a beta rebound in the frontal and parieto-occipital regions only in the healthy controls and patients of good-recovery relative to baseline (healthy controls: Pcorrected = 0.000, time range = 0.88–1.80 s; good-recovery: Pcorrected = 0.014, time range = 1.33–1.78 s). This beta increase was not significant in patients of poor recovery (Pcorrected > 0.5) (Fig. 3a-c). A list of significant electrodes was listed here. healthy controls: AF3, F7, F8, F4, FC6, T7, T8, P7, P3, P8, PO3, PO4, O1, O2; good-recovery: AF3, AF4, F7, F3, F4, FC2, T7, CP5, P7, P3, P4, P8, PO3, PO4, O1, O2.
One-way ANOVAs also revealed group differences in beta oscillations. Specifically, patients of poor recovery demonstrated a larger beta inhibition in the frontal and parieto-occipital regions compared to healthy controls and to those of good recovery (healthy controls: Pcorrected = 0.010, time range = 0.72–1.10 s, Electrodes = F3, F8, FC1, FC6, T8, PO4, P8, O2; good-recovery: Pcorrected = 0.021, time range = 0.70–0.87 s, Electrodes = AF3, AF4, F8, F3, CP6, P7, P3, P4, P8, PO3, PO4, O1, O2) (Fig. 4a-b).
Fig. 4
Group comparisons EEG oscillations. a-b) Patients of poor-recovery demonstrated a larger decrease in early beta power in the frontal and parieto-occipital regions compared to healthy controls and to those of good-recovery (healthy controls: Pcorrected = 0.010, time range = 0.72–1.10 s; good-recovery: Pcorrected = 0.021, time range = 0.70–0.87 s). c-d) Healthy controls demonstrated a larger increase in late beta power in the frontal and parieto-occipital regions compared to patients of good-recovery and to those of poor-recovery (good-recovery: Pcorrected = 0.010, time range = 0.90–1.70 s; poor-recovery: Pcorrected = 0.003, time range = 0.81–1.78 s). Tagged electrodes in each topolot indicated the significant channels revealed by cluster statistics. The time-frequency representations were plotted with the significant electrodes in the topoplot. X denotes p < 0.05. * denotes p < 0.01, dB = decibel
In addition, healthy controls demonstrated a larger beta rebound in the frontal and parieto-occipital regions compared to patients of good recovery and to those of poor recovery (good-recovery: Pcorrected = 0.010, time range = 0.90–1.70 s, Electrodes = AF3, F8, FC6, T8, P8, PO3, PO4, O1, O2; poor-recovery: Pcorrected = 0.003, time range = 0.81–1.78 s, Electrodes = AF3, F7, F8, FC5, FC1, FC6, T7, T8, C3, CP6, P8, PO4, O2) (Fig. 4c-d). Patients of good recovery and those of poor recovery were not different in the late beta power (no cluster survived p < 0.05).
Correlation resultsBeta rebound in the healthy controls and patients of good-recovery was associated with faster reaction (Fig. 5a), as well as with higher d prime sensitivity (Fig. 5b). Meanwhile, patients of poor-recovery were not included in this correlation as there was not significant beta rebound in the event-related oscillations. In contrast, beta inhibition was not associated with either reaction time or d prime sensitivity (all P > 0.05) (Fig. 5c-d).
Fig. 5
Correlation results. a-b) Increased beta power in the healthy controls and patients of good-recovery was associated with the faster reaction, as well as with higher d prime sensitivity. In contrast, decreased beta power in the early phase was not associated with either reaction time or d prime sensitivity. All EEG signals were extracted from the significant clusters in the event-related analysis
EEG connectivityAs beta rebound in the frontal and parieto-occipital regions was associated with both reaction time and d prime sensitivity, EEG connectivity was mainly analysed in this increased beta cluster. In line with event-related oscillations, in healthy controls EEG connectivity data demonstrated increased beta band WPLI compared to baseline (Pcorrected = 0.048) between the frontal regions (F4, F8) and parieto-occipital regions (P7, O1) (Fig. 6a). In the pooled dataset of healthy controls and good-recovery, EEG connectivity data indicated increased beta band WPLI (Pcorrected = 0.013) between the frontal regions (AF3, FP1, FP2, F8) and parieto-occipital regions (O1, PO3), as well as interactions between parietal and occipital regions (P3, P7, PO3, O1) (Fig. 6b). We also extended the analysis to other frequency band and the results were not significant (Pcorrected > 0.05).
Fig. 6
EEG connectivity analysis. a) In healthy controls, EEG connectivity data demonstrated increased beta band WPLI (Pcorrected = 0.048) between the frontal regions (F4, F8) and parieto-occipital regions (P7, O1). b) In the pooled dataset of healthy controls and good-recovery, EEG connectivity data indicated increased beta band WPLI (Pcorrected = 0.013) between the frontal regions (AF3, FP1, FP2, F8) and parieto-occipital regions (O1, PO3), as well as increased interactions between parietal and occipital regions (P3, P7, PO3, O1). L and R denote left and right hemispheres respectively
留言 (0)