
記住我
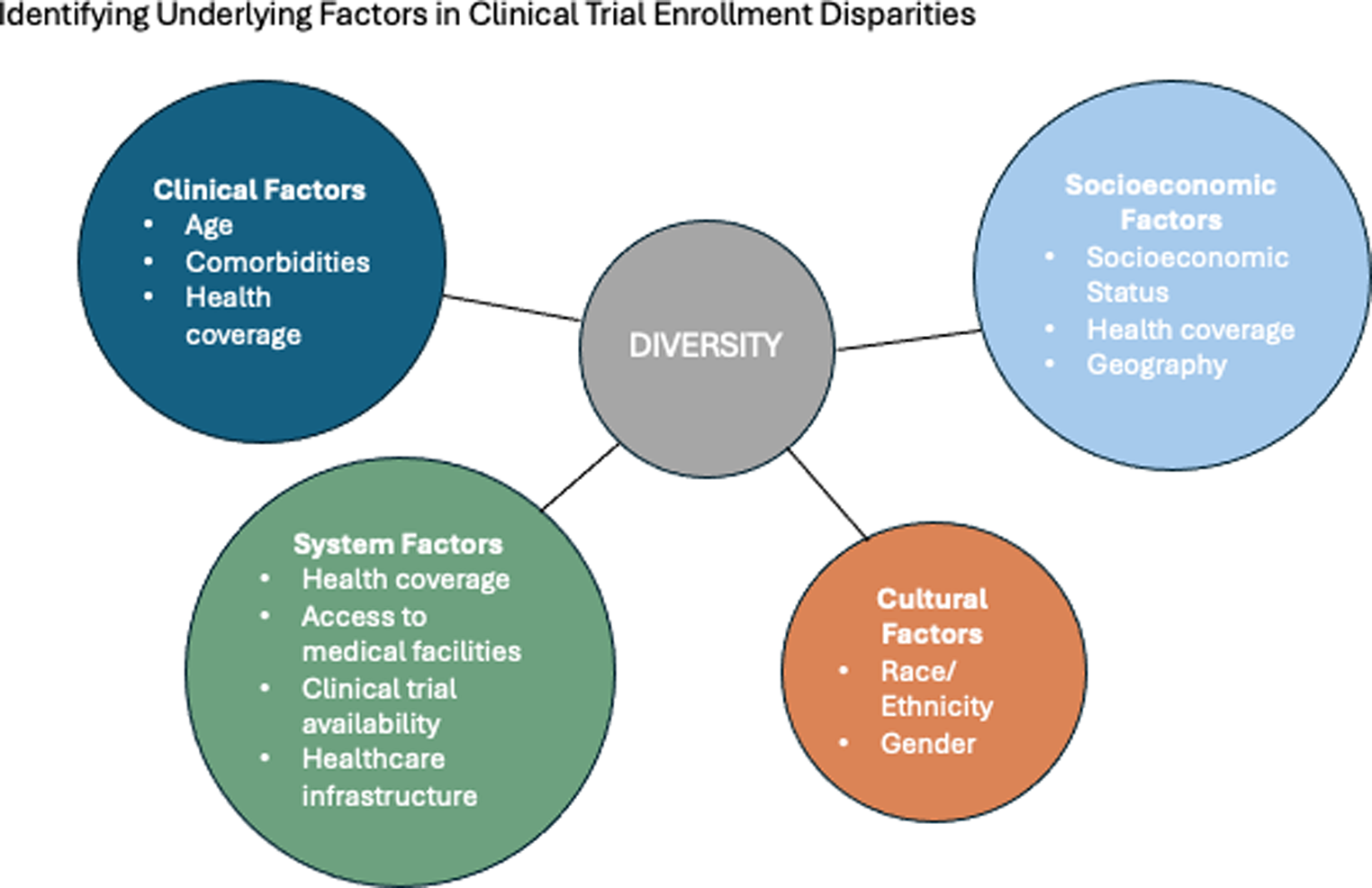





Diversity is an overarching term which includes the demographic features of an individual and other differences between patient populations. Understanding the lack of diversity in lymphoma trials largely comes from research on other types of cancer. Numerous studies have investigated the issue of disparities in clinical trial enrollment, focusing on factors such as age, race/ethnicity, gender, comorbidities, SES, health coverage, and geography (Fig. 1, Table 1). The advent of high cost, medically complex treatments such as CAR-T cell therapy for lymphoma has highlighted the need to closely examine and address factors associated with disparities in access; clinical trial enrollment being one of the surrogates for access to quality cancer care.
Fig. 1
Categories of factors that contribute to disparities in clinical trial enrollment
Table 1 Disparities in race/ethnicity and socioeconomic factors in clinical trials of lymphoid malignancies and barriers to car-t/bispecific trial enrollmentAgeAge disparities in clinical trials challenge the generalizability of research findings, as older adults are often underrepresented in studies despite being the largest consumers of healthcare services [11]. Exclusion of elderly individuals from trial enrollment is due to various factors including stringent eligibility criteria, functional impairments and comorbidities, systemic factors such as lack of resources and funding, physician factors, and patient factors [12]. This lack of representation can lead to extrapolation of efficacy and safety of treatments in older populations, resulting in less effective treatment outcomes for this population [12]. To effectively include older adults in cancer clinical trials, strategies can include designing trials specifically for this population/ broadening eligibility criteria, modifying designs for better data collection, conducting cohort studies, enhancing post-marketing surveillance, evaluating biological age, running differential dosing trials,, and advancing regulatory and policy efforts [12]. Addressing these disparities is crucial to ensure that clinical guidelines and medical interventions are applicable to all age groups.
Race and EthnicityIn trials sponsored by the National Cancer Institute evaluating a variety of cancers including breast, colorectal, lung, and prostate between 2000 and 2022, lower enrollment fractions were noted in Hispanics (odds ratio [OR] vs. whites of 0.72; 95% CI 0.68–0.77) and black individuals (OR 0.71; 95% 0.68–0.74) [1]. Between 1996 and 2002, the proportion of trial participants who were not white declined. A similar pattern was seen from a more modern nationwide cohort between 2017 and 2022 from approximately 800 sites of care from US cancer clinics [13]. The problem becomes more complex when assessing individual cancers. For example, Black individuals have lower enrollment in breast, lung, and colorectal cancer clinical trials, but similar enrollment in prostate cancer trials when compared to whites, indicating that equitable participation is achievable. The recruitment methods used for prostate cancer trials could be helpful in addressing the disparities seen in trials for other types of cancer [1]. When examining disparities among patients with hematologic cancers, Hispanic and Black individuals were 40-50% less likely to participate in clinical trials compared to whites [14]. A review of clinical trials conducted by Blood and Marrow Transplant Clinical Trials Network (BMTCTN) from 2014 to 2021 showed that the major barrier from underrepresented groups to enroll was being able to access HCT as a therapy [15]. Patients from underrepresented groups were less likely to be enrolled in BMT trials than other groups across all trials except the trial for haploidentical transplants where the proportion of enrolled minority patient was substantial [15].
Lack of representation is similarly evident in trials of CAR-T cell therapy for lymphoma, myeloma and acute lymphoblastic leukemia. Using the Vizient Clinical Database to examine pattern of racial/ethnic distribution of CAR-T cell therapy recipients, Black individuals were less likely than any other racial or ethnic group to receive CAR-T cell therapy, composing only 1% of the patients enrolled on multiple myeloma CAR-T trials vs. 16.6% in the non-CAR-T group [16, 17]. This underrepresentation is particularly notable in landmark phase 3 trials of CAR T-cell therapy in the United States, where a significant majority of participants are white, with Hispanic and Black representation below 10% [8,9,10]. Given the potential benefits of CAR T-cell therapy for chemotherapy-resistant high-risk patients, accessibility for individuals of diverse ethnic backgrounds is needed.
GenderWomen have historically faced underrepresentation and undertreatment in medicine, particularly evident in clinical trials. A study examining nearly 20,000 clinical trials conducted between 2000 and 2020 found that women were enrolled in fewer oncology trials compared to their actual burden of disease [43]. Despite comprising 46.5% of the burden of disease, women accounted for only 42.9% of clinical trial participants [44]. This disparity raises concerns about the generalizability of trial results and the effectiveness of treatments for women [44].
Furthermore, funding allocation in trial research tends to favor men over women in a significant majority of cases. Approximately 75% of the time, funding is skewed towards research involving male participants with men overrepresented in cost allocation [44]. This funding bias perpetuates the underrepresentation of women in clinical research, limiting opportunities to understand gender-specific responses to treatments and potentially leading to suboptimal healthcare outcomes for women.
ComorbiditiesHaving one or more comorbidities also contributes to decreased clinical trial participation as trials set inclusion/ exclusion criteria which prohibit those individuals from enrolling. This is complicated by a lack of empirically based standards for participant selection [18]. For example, one single-institution study of 235 Black American cancer patients found that only 20 patients (8.5%) being eligible based on inclusion criteria; most were excluded for co-existing comorbidities [19]. Although some comorbidities are understandably prohibitive of receipt of clinical trial therapy some may be too restrictive.
Additionally, the influence of comorbidities on trial participation is an important consideration. In a study from the Health Information National Trends Survey SEER which included approximately 1000 patients, only about 15% reported trial discussion and 8% reported being enrolled. Having one or more comorbidities was significantly associated with lower trial discussion [20].
Socioeconomic Status and GeographySocioeconomic factors perhaps play the most significant role in widening disparities in trial enrollment [21,22,23,24]. Individuals from lower socioeconomic backgrounds face additional barriers to accessing clinical trials, including financial constraints, lack of insurance coverage, and geographic or logistical challenges [17, 22,23,24,25,26]. In trials of hematologic malignancies, the racial and ethnic disparities are often attributed to social factors (e.g. community practice, vehicle ownership, limited English proficiency [14]. Compared to patients living in higher SES neighborhoods, patients with diffuse large B-cell lymphoma (DLBCL) living in lower SES neighborhoods had 34% and 24% higher mortality rate from all causes and lymphoma, respectively. The magnitude of mortality disparities was marked in younger patients (i.e. not eligible for Medicare) [27]. Coverage of trial-related expenses comes from a combination of the study sponsor, a patient’s insurance plan, and out-of-pocket expenses. Although insurance and the sponsor often pay for doctor visits and standard treatments, study drugs and additional tests are often not covered by insurance [28]. As some costs of a trial are reliant on insurance, patients with no insurance or with one that does not cover anticipated costs may limit their capacity to join [11]. total of 103 participants were enrolled in the study. Twenty-five were health care providers, 18 were clinic patients, and 60 were community participants; 24% lived in rural communities with populations less than 10,000. Patients and community participants ranged in age from 50 to 80 and were mostly female (81%),
Geographic location has become a more prominent variable in widening disparities after the introduction of CAR-T and bispecific antibodies. These therapies are often administered in specialized treatment centers which are not as widespread as community treatment centers, limiting access to individuals [29]. One study showed that patients from rural and Health Professional Shortage Area locations are less likely to receive immune effector cell therapies and demonstrate similar demographics to trial enrollment which indicates these populations enroll less in clinical trials [30]. Another study analyzed treatment sites that had CAR-T and bispecific antibody trials for diffuse large B-cell lymphoma across the US, and found that 20 states had no open trials, and that only a third of the Black population lived in a county with access to CAR-T or bispecific trial [31].
These disparities underscore the multifaceted nature of inequities within clinical trial enrollment, necessitating comprehensive strategies to address barriers and promote inclusivity in research participation. Table 1 summarizes these demographic and socioeconomic factors that contribute to the disparities seen in lymphoma clinical trials and treatment outcomes.
Challenges in Increasing Diversity in Trials of Lymphoid MalignanciesTable 2 summarizes the recent research on the barriers to increasing diverse lymphoma clinical trial participation. Lymphoma and CAR-T cell clinical trials predominantly feature male, white participants residing in urban, more affluent areas and receiving care in academic medical centers [1, 17, 23]. Overrepresentation of these individuals threatens the external validity of the results and reduces the ability to generalize them to different racial, socioeconomic, geographic, and gender groups. These populations also have better overall survival rates, particularly in allogeneic hematopoietic cell transplantation trials.
Table 2 Barriers to CAR-T/bispecific trial enrollmentStrategies for Improving DiversityTo enhance diversity in clinical trial enrollment, multifaceted interventions at trial recruitment, enrollment, and continued participation are imperative to address various complex barriers encountered by underrepresented populations (Fig. 2). An example is the Minority Accrual Plan developed and implemented by the University of Texas health center [32].
Fig. 2
Factors contributing to disparities and strategies for improvement
Improving Minority RecruitmentEnrollment to clinical trials starts with defining the eligibility of participants. Creating stringent inclusion and exclusion criteria such as restricting age, comorbidities, and disease spectrums excludes diverse participants and reduces the application of clinical trials to diverse individuals [33]. A potential strategy to ensure inclusion of diverse populations is creating a diversity axis which considers different factors and sets a predetermined number of participants per diversity category. Enrollment would remain open until all categories are saturated. The Minority Accrual Plan implements a similar strategy by requiring all new clinical trials to include projections for minority participation and strategies to overcome enrollment barriers and including a template and toolbox to guide these efforts [32]. Included resources are bilingual support, translated materials, and media outreach, all integrated into the trial approval process with the idea of increasing the quality and relevance of clinical trial data [32]. This approach presents several potential challenges, including the risk of bias in defining diversity, difficulty in recruiting patients for specific categories, and prolongation of the recruitment phase in clinical trials. For example, studies could enforce certain thresholds of demographics like black patients’ enrollment before granting FDA approval for products [34]. While standardizing diversity offers certain advantages, it also involves balancing the risk of exploiting minority groups for research purposes with the need to address diversity-related concerns.
Outreach programs targeting minority communities through various channels such as media outlets, churches, and health fairs can enhance the visibility of clinical trials [35]. Initiatives to educate individuals about the benefits of participation, dispel misconceptions/ firmly rooted cultural biases, and provide educational resources that empower patients to make informed decisions can further improve enrollment [36, 37]. Creating an informed consent process that is inclusive necessitates the use of simple language and culturally appropriate messages [37]. Any specific training curricula should also be developed to recognize and address race/ethnic cultural barriers [35]. Additionally, exploring minority participation fraction as a measure for institutional racial diversity can provide valuable insights into addressing disparities in correlative science participation [38].
Prospective studies are imperative for a comprehensive understanding and addressing of these disparities, with current literature predominantly emphasizing retrospective descriptive and qualitative studies [38]. Transparent reporting of demographic data in medical journals is crucial for advancing understanding and addressing disparities within the field [34]. From the staff level, efforts to increase the representation of under-represented clinicians, researchers and research staff are essential to promote diversity and inclusivity in medical research [39].
Improving AccessAs clinical trials necessitate numerous visits, it is important to consider the barriers related to the longitudinal nature of completing trials. Offering alternatives for trial communication and study visits, such as Telehealth, can improve continued accessibility, although technology-driven substitutes may not be as effective among underrepresented groups [37]. Transportation barriers are also cited as a major barrier for trial participation, thus including questions about travel concerns, monetary compensation for travel, or providing travel services could be considered [37]. Establishing partnerships between CAR-T centers and external hospitals can improve provider familiarity, facilitate patient referrals, and enhance overall access to CAR-T clinical trials [40]. Expanding CAR-T therapy to community hospitals and axillary buildings such as specialized cancer treatment centers offer the potential to reduce travel time and financial toxicity [23]. Periodic diversity surveys can be another way to assess progress towards improving access through continuous feedback from patients, investigators and community partners throughout a trial. Monitoring the diversity of patients enrolled in trials through recording sex, race and ethnicity could help to ensure that minority populations are represented.
Accounting for Biologic DifferencesFrom a biological standpoint, it is vital to recognize and account for racial differences in lab values to prevent the exclusion of potential participants based on normal variations related to race [35]. For instance, benign ethnic neutropenia is commonly observed in African Americans and can lead to exclusion from clinical trials due to Absolute Neutrophil Count (ANC) values below 1.0, despite this being a normal variant in this population [41]. This condition can result in unnecessary exclusion of African Americans from clinical trials and treatments that use ANC as a criterion, possible skewing research outcomes and treatment efficacy across different racial groups [41]. Increasing representation in biobanking is also essential to prevent the misdirection of drug development and promote pharmacogenomic advancements [42]. Pharmacogenomics investigating genetic variations, both heritable and somatic, influence drug responses and are underrepresented in minority populations [36]. For instance, Black patients with lymphoma were less likely to receive standard chemoimmunotherapy compared to White patients, despite its recommendation as the standard of care [34]. Promoting studies that no not require HLA matching in clinical trials can be one avenue to promote participation among diverse populations.
Addressing the Patient-Clinician RelationshipAs individuals may have any combination of barriers to enrollment, adopting a patient-centered approach through patient navigation models can support participants throughout the trial process [43]. Beyond physical obstacles, addressing emotional needs and promoting mental health resources are vital components of ensuring participant well-being. Building stronger patient-physician relationships, approaching patients with cultural sensitivity in mind, and ensuring self-explanatory information are essential for fostering trust and engagement [37].
Contributing to Culture Change/ Community Outreach and EngagementPolicy changes are imperative to address disparities in clinical trial enrollment. Organizations, such as the American Society of Clinical Oncology (ASCO), have established committees and policies to tackle cancer care disparities and promote health equity. Community involvement is also crucial for enhancing access to trials among minority groups, necessitating collaboration with community hospitals, clinics, and agencies focused on serving underrepresented populations [35, 37]. Hospital systems can enhance community engagement by creating dedicated staff positions to identify local health needs and collaborate with community partners. Such Community Outreach and Engagement (COE) initiatives at various cancer centers can help improve access and outcomes for vulnerable populations. These roles can include participation in leadership boards and special projects, helping to stay connected with community needs and address enrollment disparities. Creating government incentives or funds for implementing trials in community hospitals can help apply these ideas. Utilizing telemedicine methods can broaden hospital eligibility for participation in research and Principal Investigator involvement. One example of COE is the Community Clinical Oncology Program funded by the NCI that aimed to increase community-based physicians’ familiarity with clinical trials to increase quality and accessibility of community-based care [44]. Another example is the Abramson Cancer Center’s COE program that creates culturally tailored marketing strategies in collaboration with faith-based organizations serving black communities with the goal of increasing enrollment of black patients into cancer clinical trials [44]. Implementing programs like these to advocate for minority populations and encourage their involvement in trials is integral for increasing access and improving diversity in clinical trials.
留言 (0)