Data source and study population
Using cross-sectional data from the EU LGBTI Survey II allowed the exploration of a wide range of dimensions of LGBTI (LGBT and intersex) lives, surveyed in 2019, in 30 European countries: sexual orientation, gender identity, sex characteristics, trends, and responses to LGBTI-phobias in the country, discrimination, safety, physical/sexual attacks, social context, and sociodemographic information. Overall, 139,735 LGBTI people were reached via the internet, of minimum age 15 years old, including 20,282 trans people. The methodology of the survey was fully described in the technical report by the European Union Agency for Fundamental Rights [31].
Sexual orientation
Participants were asked “In terms of sexual orientation, we can only use a limited number of categories for our analysis. So, we would like to ask you which group best matches your sexual orientation. Select the answer that best matches your sexual orientation.” Proposed answers were “Lesbian”, “Gay”, “Bisexual”, “Heterosexual/Straight”, “Other, please specify” and “Don’t know”. Respondents who identified as heterosexual/straight, as long as they did not identify as trans and/or intersex, were excluded from the analyses (n = 64 people).
Gender identity
Participants were asked “How would you describe yourself today?” Response options were “Woman/girl”, “Man/boy”, “Trans woman/girl”, “Trans man/boy”, “Nonbinary or genderqueer or agender or polygender or gender-fluid”, or “Do not identify as male, female, trans or nonbinary”. Following recommendations from the European Union Agency for Fundamental Rights questionnaire, we considered the third, fourth and fifth answers to identify trans people. Another question asked “Are/were you a trans person? The term trans is used in this survey as a broad umbrella term that includes all those who are transgender, nonbinary, gender variant, polygender, agender, gender-fluid, cross dressers, transsexual, or men and women with a transsexual past, and other terms.” Answers offered may be “Yes” or “No”. Following the questionnaire, we considered the “Yes” option as an identifier for trans people. All nontrans people were considered cis people.
Sex assigned at birth
Participants were asked “What sex were you assigned at birth?” with the following instructions: “Sex assignment at birth is the classification of people as male, female, intersex or another sex assigned at birth often based on physical anatomy. The sex assigned at birth is recorded in your birth certificate when you were born”. Possible answers were “Female”, “Male”, and “Other, specify”. Since the present paper aimed to investigate the ratio between AFAB and AMAB people, we excluded the option “Other, specify” (n = 1,207 people) from the analyses. Note that most intersex people in our sample were assigned male or female at birth.
Self-perception, identity-sharing, and “rapid-onset identity-sharing”
One descriptive element in Littman’s account of ROGD is that AFAB trans youth subjected to rapid-onset gender dysphoria do not display signs of gender non-conformity before puberty. We aimed to identify and quantify those people, in both AMAB and AFAB, for trans youth but also cis youth.
Lesbian, gay or bisexual participants were asked the following questions: “How old were you when you realized for the first time you are [respondent category – only L, G or B]?” and “How old were you when you first told somebody you are [respondent category – only L, G or B]?” We considered the response to the former question as the age corresponding to one’s self-perception of identity questioning (LGBT self-perception) and the response to the latter as the age corresponding to LGBT identity-sharing. We withdrew individuals who had not yet shared their LGBTI identity from further analyses (n = 7871 people).
Trans participants were asked the following questions: “At what age did you first realize that your feelings about your gender did not match the gender assigned to you at birth?” and “How old were you when you first told someone about this?”. As above, we withdrew respondents who had not yet shared their trans identity from the analyses (n = 2637).
For all LGBT people, we considered people who declared sharing their identity at an age prior to the age of self-perception as an inconsistent response (n = 975 people) and discarded those results. For trans people who were also lesbian, gay or bisexual, we considered their identity-sharing age as the age they shared their trans identity, not their lesbian gay or bisexual identity. We observed the same rule for their age of self-perception.
The rapidity or suddenness at which the “gender dysphoria” of someone appears to another one is highly subjective. We sought to describe such rapidity of development by distinguishing two categories of people: those who shared their identity during adolescence (defined as 12–17 years old) and had their self-perception at the same age of their identity-sharing age (“rapid-onset identity-sharing”) and those who shared their identity during adolescence but had their self-perception strictly before their age of identity-sharing, i.e., “slow-onset identity-sharing”. We generalized this definition to all LGBT people, regardless of their gender modality (cis or trans) [32].
The above definition being arbitrary as regards the pubertal onset age (12 years old) and of what is considered “rapid” (here, when identity-sharing is done within a year from self-perception), we defined for sensitivity analyses rapid-onset vs. slow-onset identity-sharing for k varying degrees of delay between ages of self-perception and identity-sharing, and for p varying ages of pubertal onset. With isa the age of identity-sharing, and spa the age of self-perception, we note:
$$\begin} = \hfill \\\left\}}\,}\,\,spa \geqslant isa - k\,\,and\,\,\,isa \geqslant p\,\,and\,\,isa < 18} \\ }\,\,spa < isa - k\,\,and\,\,isa \geqslant p\,\,and\,\,isa < 18} \end} \right. \hfill \\ \end$$
$$}\,}\,:spa \le isa;k \in \left[\kern-0.15em\left[ \right]\kern-0.15em\right]; p \in \left[\kern-0.15em\left[ \right]\kern-0.15em\right]$$
LGBTI national laws and policies
The ILGA-Europe’s Rainbow Index [30] reflects the legal and policy human rights situation of LGBTI people in Europe, scoring each country on a scale from 0% (“gross violation of human rights, discrimination”) to 100% (“respect of human right, full equality”). In 2019, it scored and ranked 49 European countries, by evaluating in each one 69 dichotomous measures from 6 dimensions: “Equality and non-discrimination”; “Family”; “Hate crime & hate speech”; “Legal gender recognition & Bodily integrity”; “Civil society space”; “Asylum”. We used that scale to capture the quality of national laws and policies regarding LGBTI people.
ROGD hypothesis-related variables
Since the EU LGBTI Survey II is not a clinical sample, very few variables explore health, and fewer explore the mental health dimension, hypothesized to be influenced negatively by the ROGD. Participants were asked “How is your health in general?” and answers offered were classified from 1 to 5 points as follows: “Very bad”, “Bad”, “Fair”, “Good”, “Very good”. Another question investigated the presence of long-standing illness: “Do you have any long-standing illness or health problem?” The survey gave the following instructions: “Long-standing means illness or health problems or which have lasted, or are expected to last, for 6 months or more.” Answers were coded 0 for “No” and 1 for “Yes”. A question approached more directly the mental health dimension: “Have you been feeling downhearted or depressed over the last two weeks?”, and possible answers were coded reversely from 1 to 6 as follows: “At no time”, “Some of the time”, “Less than half of the time”, “More than half of the time”, “Most of the time”, and “All the time”.
Regarding social media use, we used the fact that the participants who were reached by social media (the most effective way of reaching participants in the survey) had to answer the following question: “How often do you visit online this page or group you follow on Facebook, Instagram, Twitter, etc.?”. The “page or group” mentioned refers to the social group in which the invitation to the survey was posted. This is a proxy to measure the connectedness of the participants to social media serving as platforms for LGBTI content. Answers were coded from 1 to 7 points: “Never”, “Very few times a year”, “Once a month”, “Two or three times a month”, “Once a week”, “2–3 times a week”, “Every day”.
Sociodemographic variables
Age is a categorical variable containing 11 levels, starting from the 15–17 years old category, then the 18–24 years old, then 8 levels of 5 years of age intervals, until the last category (65 years old and more).
Education level was coded as follows. To the question “What is the highest level of education you have completed?”, respondents were coded “Primary or no education” when answering “No formal education” or “Primary education”; “Secondary education” when answering “Lower secondary education” or “Upper secondary education”; “Tertiary education” when answering “Post-secondary education other than college/university”, “Bachelor or equivalent”, “Master or equivalent”, or “Doctoral or equivalent”.
Living in an urban/rural area was coded according to answers to the question “Where do you currently live?”. Possible answers were “A big city”, “The suburbs or outskirts of a big city”, “A town or a small city”, “A village”, or “A farm or home in the countryside”, however the dataset only refers to “urban” and “rural” areas.
Belonging to a minority was coded according to answers to the question “In the country where you live, do you consider yourself to be part of any of the following, other than LGBTI?”. Possible answers include: “An ethnic minority (including of migrant background)”, “A religious minority”, “A minority in terms of disability”.
Easiness with income was coded following answers to the question “Thinking of your household’s total income, is your household able to make ends meet?”. Answers “Fairly easily”, “Easily”, and “Very easily” were coded as 1; “With great difficulty”, “With difficulty”, “With some difficulty” were coded as 0.
Statistical analyses
We performed all statistics under Stata 18 [33]. Overall, this study explores the whole sample and two subsamples. The whole sample serves to compute probabilities of identity-sharing at all ages, as well as constructing country-level sex differences in the capacity of identity-sharing. The subsample of respondents of any age who self-perceived before 18 allows us to investigate retrospectively how long it has taken for self-perceived LGBT children and adolescents to share their identity. The adolescent subsample (respondents aged 15, 16 or 17) allows us to define rapid and slow-onset identity-sharing young populations, questioned on their health and their social media use at these ages.
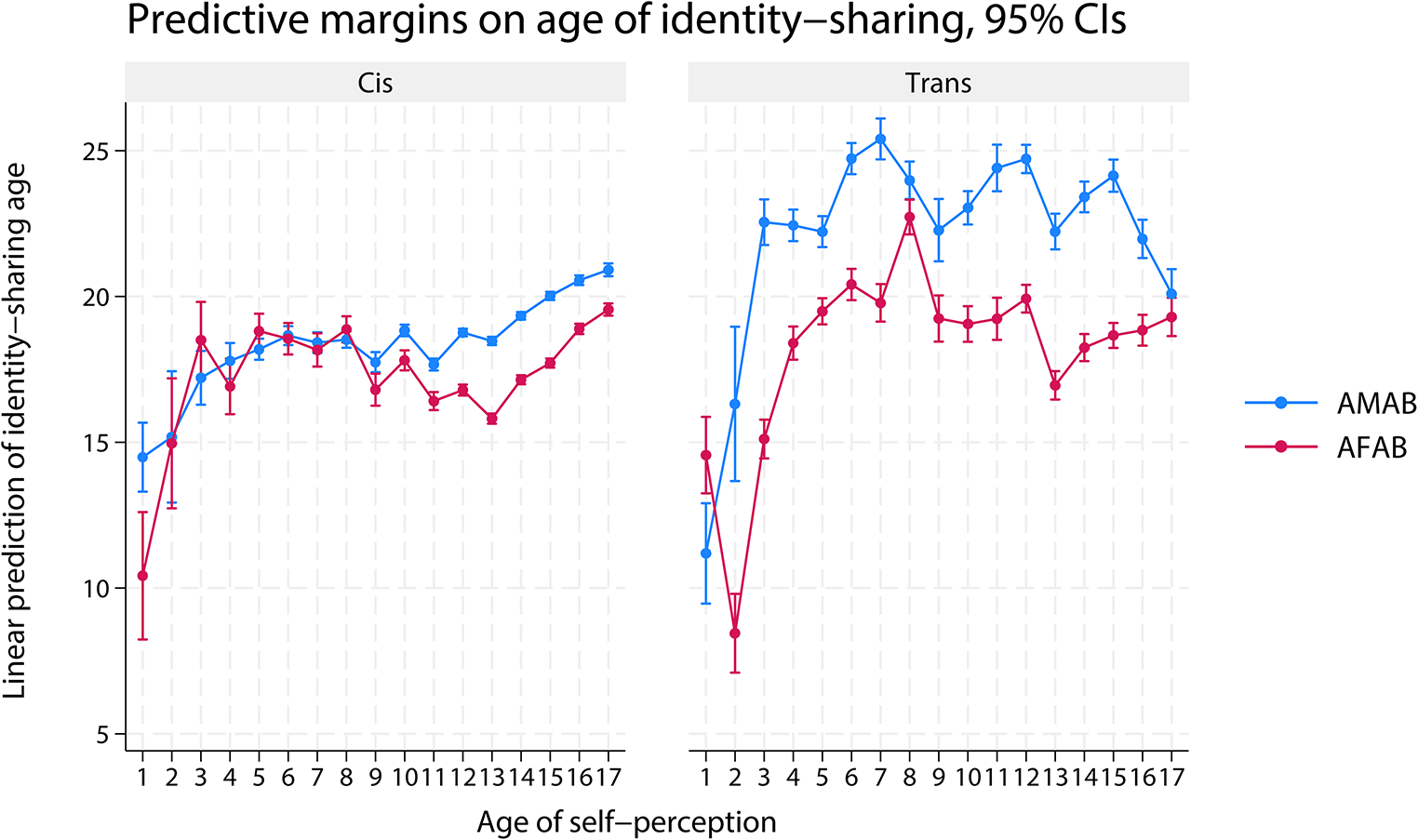
To appraise how cis LGB and trans youth, AFAB and AMAB youth, share their LGBT identity differently when given equal conditions of self-perception as LGBT, we ran a weighted least squares regression of the age of identity-sharing on all possible ages of self-perception prior to 18 years old, interacted with the category of people (cis or trans, AFAB or AMAB). Since we expected cultural influences to constrain the possibilities of sharing one’s LGBT identity, we controlled for country-fixed effects to capture these influences (see the method in Supplementary Materials).
To better appreciate the impact on a sex ratio that gaps in the chance of identity-sharing between AFAB and AMAB make, we estimate in the whole sample the probabilities of identity-sharing before the age of j, for those who have had already their self-perception by the age j, for AMAB, AFAB, cis and trans people, and hypothesizing equality of all population sizes. We compute \(\:_^\), \(\:_^\), \(\:_^\) and \(\:_^\) these probabilities, respectively for transmasculine people (i.e. AFAB trans people), transfeminine people (i.e. AMAB trans people), cis males and cis females. We then construct the sex ratio of people who shared their identity before the age of j, which we note \(\:_^\) and \(\:_^\) respectively for trans and cis people. We hypothesize that the AFAB and AMAB populations who self-perceived are equal in size (which we note n), both for trans and cis people, and write sex ratios as random variables:
$$\:_^\rightsquigarrow\:\frac_^)}_^\right)+Bin(n,_^)};\:_^\rightsquigarrow\:\frac_^)}_^\right)+Bin(n,_^)}$$
Given the hypothesized equality of sizes of AFAB and AMAB populations who self-perceived, we expect the sex ratio to converge towards 0.5 at the latest age. Any deviation from 0.5 in earlier ages would be the result of the differences in the distribution of probabilities of identity-sharing for AFAB and AMAB people who already self-perceived. We run the model 10,000 times with n fixed at 1,000.
To evaluate the macro-environmental factors that may influence someone’s capacity to share their LGBT identity, we investigated systematic differences between countries as regards the different chances AFAB and AMAB LGBT people may have in such countries to share their identity, holding equal their age of self-perception. Using weighted least squares, we regressed in the whole sample the age of identity-sharing on the assigned sex (AFAB or not) and the country, and their interaction, while controlling for the age of self-perception. Based on these estimates, we computed for each country the national LGBT contrasts (see method in Supplementary Materials), which are the national adjusted average differences in age of identity-sharing between AFAB and AMAB LGBT people. The ILGA-E’s index of 2019 was used as a measure of macro-environmental factors affecting LGBT people, and its correlation with the national LGBT contrasts was computed.
To test whether having had a rapid-onset identity-sharing may relate to poorer health or increased social media use among subcategories of the LGBT adolescent population, we used weighted least squares, on the subsample of adolescent respondents (aged 15, 16 or 17). We regressed each of our ROGD hypothesis-related variables (self-assessed health, long-standing illness, depressed feelings, social media use) on the category of people (trans or not, AFAB or not, having had a rapid-onset identity-sharing or a slow-onset identity-sharing). Country weights have been systematically implemented in regressions to address imbalances between national sample sizes. Country fixed effects have also systematically used to capture heterogeneity of health or social media responses due to national differences. Additionally, since sociodemographic variables are likely to influence health and social media use, we checked whether the regression results held with additional controls for education level, living in a rural/urban area, belonging to another minority group, and easiness with income.






留言 (0)