
記住我





This multicenter, randomized controlled, non-inferiority trial was conducted across nine hospitals in Taiwan following approval by the institutional review board or institutional ethics committee of each participating hospital. The trial was registered on the Clinical Trials Open Registry (http://clinicaltrials.gov, ID: NCT01477008). The protocol and subject-related documents were reviewed and approved by the Taiwan Food and Drug Administration (TFDA). These institutions also approved the 1-year blinding protocol. Microfracture surgery, being the most commonly utilized reparative approach, was selected as the control treatment. In a prior study, patients treated with microfracture surgery exhibited an increase in the International Knee Documentation Committee (IKDC) overall score from a pre-operative value of 41.1 ± 12.3 points to 70.2 ± 14.7 points, representing a 29.1-point improvement [24]. Sparingly, we established the non-inferiority margin at 12 points, approximately 60% of the effect seen with microfracture surgery, with the standard deviation of the IKDC score set at 20 points. Based on these assumptions, the calculated number of patients required to validate the non-inferiority of the investigational group to the control group, with a one-sided statistical significance level of 2.5% and a power of 80%, is 38 patients per group. To account for potential exclusions affecting 20% of the subjects in the final evaluation, we increased the sample size to include 46 patients in each group.
Every patient provided informed consent before participating in the study. Participants were thoroughly informed during the consent process that they would remain blinded to their treatment unless complications at the surgical site required reoperation on the chondral or osteochondral lesion. Even if a patient withdrew from the study for reasons unrelated to the surgical site, their treatment allocation would remain blinded for 1 year post-surgery. A data safety monitoring board (DSMB) comprising a medical doctor, an independent statistician, and a clinical trial expert was established to safeguard the participants' interests, assess intervention safety while maintaining the blinding, and oversee the trial’s conduct and integrity.
Patients with symptomatic chondral or osteochondral defects of the medial condyle, lateral condyle, or the trochlea of the distal femur were invited to participate if they met the following inclusion criteria: (1) age < 55 years with a single lesion diagnosed by arthroscopic examination and magnetic resonance imaging (MRI); (2) a lesion size of less than 23 mm × 12.5 mm; (3) a lesion of International Cartilage Repair Society (ICRS) grade 3–4, Outerbridge grade 4, or osteochondritis dissecans grade 3–4; (4) skeletally mature as determined by plain roentgenography, with closure or absence of the physeal plate at the distal femur and proximal tibia. Patients were excluded if they had other lesions > grade II on the articular surface of the tibia or patella, prior surgical treatment of the target lesion, a lesion requiring bone grafting, rheumatoid arthritis, another inflammatory arthritis, severe meniscal damage (defined as > 50% of the meniscus missing or a radial tear extending to the meniscal–synovial junction), knee stiffness (flexion contracture > 10° or flexion degree < 115°), body mass index (BMI) > 35.0, local or systemic infection (except for an asymptomatic urinary tract infection), pregnancy, or breastfeeding. Once the lesion size was confirmed intraoperatively by an arthroscopic procedure to meet the inclusion criteria, the patients were randomized to receive either BiCRI implantation or microfracture surgery.
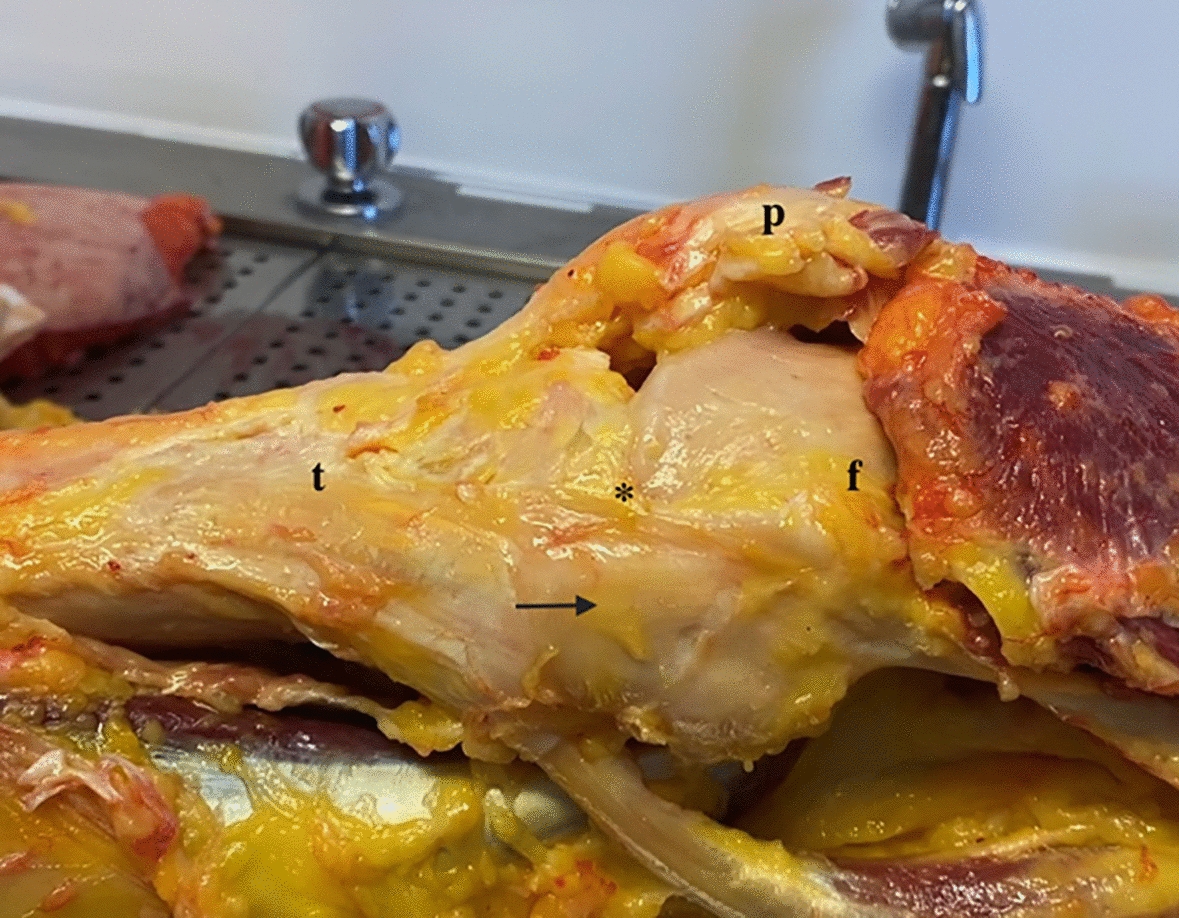
Biphasic cartilage repair implantThe biphasic construct was produced using a modified solvent-merging and particulate-leaching technique, as described previously [25]. This porous cylindrical structure comprised two distinct phases: a chondral phase and an osseous phase. The chondral phase, accounting for one-sixth of the total height, was composed of polylactic-co-glycolic acid (PLGA). The remaining portion constituted the osseous phase, made from a composite of PLGA and tricalcium phosphate (TCP) (Fig. 1).
Fig. 1
The biphasic osteochondral construct. The design features a barrel-and-plug structure, enabling easy insertion of minced cartilage through the opening on the osseous side. Once the cartilage graft is loaded, the plug is secured to enclose a flat chamber, positioning the graft between the plug and the chondral phase of the construct
A flat chamber, 6.5 mm in diameter and 1 mm in height, was positioned between the chondral and osseous phases, serving as a reservoir for the double-minced autologous cartilage graft. The final construct measured 8.5 mm in both diameter and height. All constructs used in this study were manufactured in a laboratory adhering to good manufacturing practice (GMP) standards. Preclinical evaluations, including toxicology testing and animal studies, had been conducted [26], and the construct's effectiveness in promoting cartilage regeneration was confirmed in a porcine model [20, 27].
Surgical procedures and postoperative protocolAll surgical procedures were performed by ten sports-fellowship-trained surgeons, each with over 10 years of experience at their respective hospitals. Prior to the study, these surgeons underwent specialized training on the implant and participated in simulated knee surgery using anatomical models to ensure consistency in surgical technique. Routine knee arthroscopy was performed first to locate the lesions. Depending on the lesion sites, a longitudinal mini-arthrotomy along the medial or lateral border of the patellar tendon was made to approach the defect. For the BiCRI group, the details of the surgical procedures were described previously [22, 23]. In brief, an 8-mm cylindrical hole was created with a cylinder punch to maximally cover the lesion. The cartilage of acceptable quality within the punched area was excised and collected as part of the autograft. Additional autograft was curette harvested from the non-articulating margin of the affected condyle to achieve a total volume of 0.15 cm3 cartilage. The cartilage was immersed immediately in sterile saline and morselized with a specially designed tissue pulverizer with a sieve to obtain particles smaller than 1000 μm. The particles were further dissociated with collagenase (Librase, Roche Diagnostics, Mannheim, Germany) at 37 °C for 20 min. After the removal of collagenase through copious rinses with saline, the cartilage graft was transferred to the flat chamber in the BiCRI. The prepared BiCRI was then pressed into the previously punched hole. The patients received either one plug (lesion size ≤ 12.5 mm × 12.5 mm) or two plugs (lesion size ≥ 12.5 mm × 12.5 mm and ≤ 12.5 mm × 23 mm). For the microfracture group, multiple holes were made using 1.5-mm-diameter awl to a depth of 5 mm at distances of 3 to 4 mm.
Postoperative visits were scheduled at 6 weeks, 3 months, 6 months, and 12 months after the surgery. The following evaluations were accomplished at each postoperative visit: IKDC 2000 Subjective Knee Evaluation Form score; Knee Injury and Osteoarthritis Outcome Score (KOOS); IKDC 2000 Knee Examination Form; IKDC 2000 Current Health Assessment Form; 100-mm visual analog scale (VAS) at sitting, standing, and squatting; and the assessment of adverse events. A trained study nurse interviewed the patients and assisted the patients to complete the above assessments. Plain roentgenography, MRI, and second-look arthroscopy (only for patients who agreed to the additional procedure) were done at 12 months postoperatively. T1-weighted spoiled gradient echo (GRE), T2-weighted fast spin-echo and proton density images were conducted for MRI evaluation. The cartilage regeneration status was evaluated and graded as (1) fully regenerated, (2) partially regenerated, or (3) not regenerated. The Outerbridge classification was used to grade repaired tissue during arthroscopic examination. The evaluators of the MRI and arthroscopic video were blinded to the treatment.
Rehabilitation protocolBoth patient groups underwent identical postoperative rehabilitation. For the first 6 weeks, patients used a knee brace with motion restricted to 0–90°. They were required to complete at least 500 passive knee flexion cycles daily and maintain partial weight bearing of up to 20 pounds (approximately the leg’s weight) using a heel–toe gait with two crutches. From week 6 to 8, patients gradually advanced to full weight bearing as tolerated.
Study endpointsThe primary endpoint was the change in IKDC 2000 Subjective Knee Evaluation Form score from baseline. The secondary endpoints included the grade distribution for each domain of the IKDC 2000 Knee Examination Form and the amount of improvement evaluated by IKDC 2000 Current Health Assessment Form, KOOS, pain visual analog scales (VASs), MRI findings, and arthroscopic findings at 12 months.
Statistical analysisThe patients were analyzed on an intention-to-treat (ITT) basis according to their randomization group. Missing data were accounted for by using the last observation carried forward method. For continuous variables, the number, mean, standard deviation, median, minimum, and maximum values were presented, and an analysis of variance (ANOVA), with treatment and study site as fixed effects, was performed to test the null hypothesis of prior-to-randomization comparability across treatment groups. For categorical variables, the numbers and percentages of subjects in each class were presented, and the Cochran–Mantel–Haenszel test adjusted for the study site was performed. The continuous efficacy outcomes were analyzed using an analysis of covariance (ANCOVA) with the baseline measure of that efficacy parameter as the covariate and effects of treatment and site as factors. Point estimates and 95% confidence intervals for the differences between the treatment groups were estimated. Summary statistics of the measured values, the percent changes, and the mean changes in the total IKDC-2000 Subjective Knee Evaluation Form score and other continuous efficacy outcomes were obtained for each group by observation time point, and their changes over time were also graphically presented.
留言 (0)