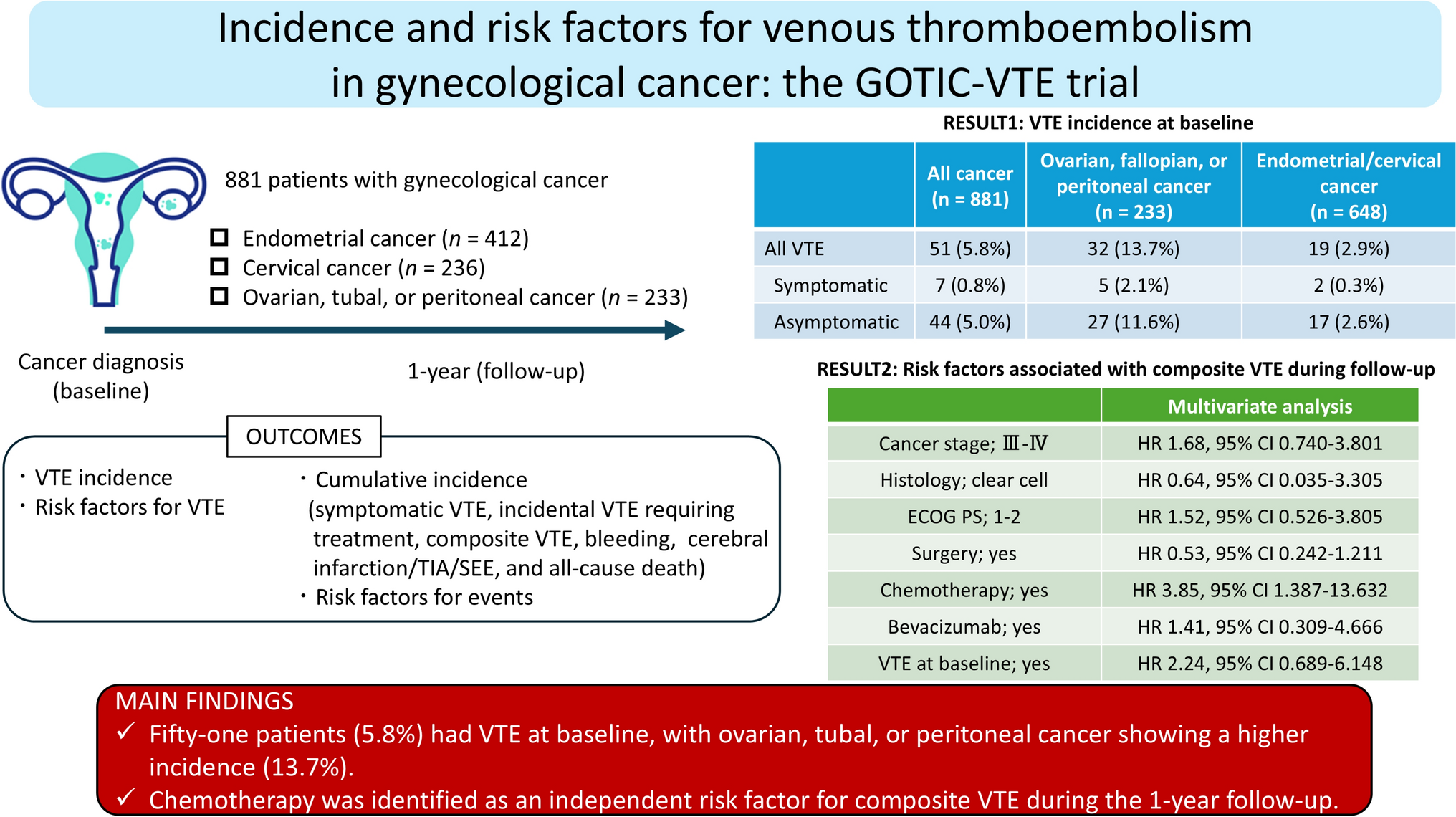
The GOTIC-VTE trial was the first large prospective observational study to evaluate VTE incidence in Japanese patients with gynecological cancer. The VTE incidence at the time of cancer diagnosis was 5.8%, with a particularly high rate of 13.7% in ovarian, tubal, or peritoneal cancer. During the 1-year follow-up, 0.9% of the patients had symptomatic VTE and 3.5% had composite VTE. The cumulative incidence of these events was significantly higher in the group with VTE at baseline than that in the group without VTE. In the multivariate analysis, chemotherapy was an independent risk factor for composite VTE during the 1-year follow-up.
In the Cancer-VTE Registry, a prospective study of VTE incidence in various cancer types in Japan, the incidence of VTE was 5.9% among 9630 patients at diagnosis (before treatment). Pancreatic cancer had the highest incidence (8.5%), followed by gastric (6.9%), colorectal (6.4%), gynecologic (5.8%) (data provided in this study), lung (5.0%), and breast (2.0%) cancers [14]. The incidence of cancer-associated thrombosis was higher in the more advanced stages [6, 22]. In total, 67.2% of patients with gynecologic cancers registered in the Cancer-VTE Registry were stage I; only 19.3% of those with lung cancer were stage I; and stage I was excluded from the registry in other cancer types. An analysis of VTE incidence by stage showed that the rate was 5.2% for gynecologic cancer stage II (vs. 3.8% overall), 10.4% for stage III (vs. 5.3% overall), and 17.1% for stage IV (vs. 11.2% overall), indicating that gynecologic cancer has higher VTE concomitant rates than other cancer types [13].
In this analysis of the GOTIC-VTE trial, ovarian, tubal, or peritoneal cancer had a higher rate of VTE than endometrial and cervical cancers (13.7% vs. 2.9%, p < 0.0001). In the United Kingdom, 4.8% of 397 patients with ovarian cancer had VTE at diagnosis [23], and in the USA, 3.1% of 843 patients with ovarian cancer had VTE [24]. In comparison, the higher rate of VTE (13.7%) in this study was probably due to the influence of clear cell carcinoma (CCC). Studies have reported that CCC releases many tissue factors and activates coagulation, leading to the development of VTE [25, 26]. In Europe and the USA, CCC is rare; only 5.3 and 7.7% of all cases had CCC, respectively [23, 24]. In contrast, in Japan, CCC is the second most common histological type of ovarian cancer [27] and accounted for 15.5% of all ovarian cancers enrolled in this study. Univariate analysis of associated factors for VTE at baseline revealed no statistically significant differences in VTE incidence for CCC compared with other histologic findings (11.1% vs. 5.6%) but showed an odds ratio (OR) of 2.12 (95% CI: 0.31–5.63). In a retrospective analysis of 470 patients with ovarian cancer reported from Japan, the OR of VTE in CCC versus non-CCC significantly increased to 1.41 (95% CI: 1.04–1.93) [10]. Consistently, a meta-analysis of 6324 ovarian cancers showed a significantly increased OR of 2.11 (95% CI: 1.55–2.89) for CCC [28]. Therefore, Japanese patients with gynecologic cancers, especially ovarian cancer, should be considered at high risk for VTE.
Multivariate analysis showed that chemotherapy was an independent risk factor for composite VTE during the 1-year follow-up (HR: 3.85, 95% CI: 1.387–13.632). Among 26,863 Korean patients with ovarian cancer, chemotherapy was associated with the highest rate of VTE (306 per 10,000 women) compared to surgery and radiation therapy [29]. Regarding the risk of VTE with platinum agents, a key drug for gynecological cancers, a meta-analysis reported increased risk, with a relative risk (RR) of 1.67 (95% CI: 1.25–2.23) [30]. Conversely, bevacizumab was not a risk factor for composite VTE (HR: 1.41, 95% CI: 0.309–4.666). Bevacizumab is currently approved in Japan for cervical and ovarian cancer treatment. In the randomized control trial (RCT) of bevacizumab combined with chemotherapy in cervical cancer (GOG-240), thromboembolic events were significantly higher with bevacizumab (8% vs. 1%, p = 0.001) [31]. In contrast, the RCT of bevacizumab in ovarian cancer (GOG-218) showed no difference in the incidence of venous and arterial thromboembolic events [32]. Two meta-analyses showed an increased risk (RR: 1.29, 95% CI: 1.12–1.47 [33] and RR: 1.33, 95% CI: 1.13–1.56 [34]), and another two meta-analyses showed no increased risk (RR: 0.89, 95% CI: 0.66–1.20 [35] and OR: 1.14, 95% CI: 0.96–1.35 [36]). Therefore, the findings are controversial [37]. In the present study, bevacizumab was not a risk factor for VTE (HR: 1.41, 94% CI: 0.309–4.666). However, bevacizumab significantly increased the thrombotic response in a mouse model [38]; thus, caution is recommended for VTE with bevacizumab use.
In this study, univariate analysis of associated factors for VTE at baseline identified the following factors: clinical stages III–IV, cancer type (ovarian, tubal, or peritoneal), ECOG PS 1–2, history of VTE, platelet count ≥ 350 × 109/L, Hb < 10 g/dL, WBC count ≥ 11 × 109/L, and D-dimer > 1.2 µg/mL. Univariate analysis identified the following associated factors for composite VTE during the 1-year follow-up: age > 65 years, clinical stages III–IV, chemotherapy, and VTE incidence at baseline. The Khorana score was proposed in 2008 as a predictive model for VTE in a prospective study of outpatients with cancer receiving chemotherapy [39]. The Khorana score was calculated from the primary site, platelet count, Hb, WBC count, and body mass index (BMI). However, a study to validate the Khorana score for various cancer types reported that the score failed to stratify the risk of gynecologic cancers [40]. The BMI threshold used in the Khorana score is 35 kg/m2, but it is questionable whether this score can be a reasonable cutoff value for the Japanese population, considering their small stature compared with that of foreigners. Based on these findings, it is aimed to develop an original score that can predict the risk of VTE in Japanese patients with gynecologic cancer.
This study had several limitations. First, follow-up was limited to 1 year. Second, the patient selection was biased. This study excluded patients with PS ≥ 3 and life expectancy < 6 months, which prevents generalization to patients with a poor condition. Third, imaging was not performed in all patients at enrollment and was not routinely requested during follow-up unless symptoms of suspected VTE were present, which may have affected the accuracy of asymptomatic VTE detection. Finally, this was an observational study, and anticoagulation for any VTE was performed at the discretion of the physician.





留言 (0)