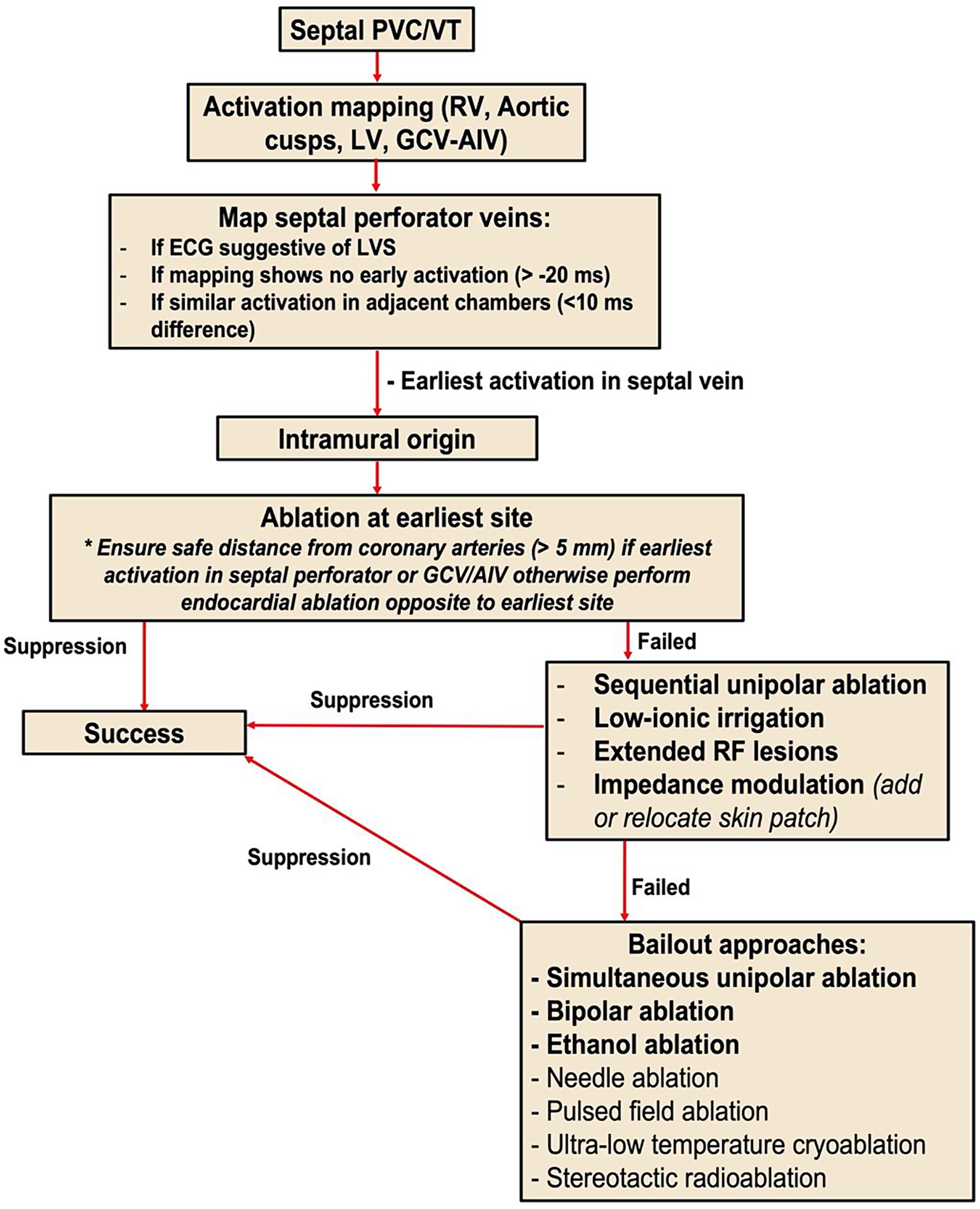
In many cases, intramural VAs can be successfully eliminated by conventional radiofrequency (RF) ablation delivered from the closest endocardial site, but prolonged lesions (up to 5 min) or ablation from multiple sites may be necessary. Typical unipolar ablation generates a lesion depth of 5.7 ± 0.4 mm under standard conditions in an ex vivo model [6]. As the myocardium can be > 10 mm thick in many areas including the septum and LV ostium, transmurality is often difficult to achieve. The use of low-ionic irrigant solutions, such as half-normal saline (HNS; 0.45% NaCl) and 5% dextrose in water (D5W), may also enhance current delivery to the tissue [7] and result in increased lesion depth and size [6, 8]. In a study of 94 patients with VAs refractory to standard catheter ablation, irrigation with HNS resulted in acute arrhythmia suppression in 84% of cases with one year VT-free survival of 89.4% [7].
When standard ablation fails or results only in transient arrhythmia suppression, several bailout ablation strategies can be considered:
Simultaneous Unipolar Ablation
Simultaneously approaching the area of interest from two vantage points may result in deeper lesion formation than sequential unipolar ablation. For simultaneous RF unipolar ablation, catheters are placed on adjacent structures and RF is delivered through both catheters at the same time. This technique requires two open-irrigated catheters attached to two generators, which can increase equipment cost.
Bipolar Ablation
Bipolar RF ablation is performed by placing ablation catheters at adjacent cardiac structures surrounding the VA focus (Fig. 3). Energy is delivered from one catheter while the second catheter is used as return electrode instead of the dispersive skin patch, with the size of the return catheter electrode modulating lesion characteristics [9]. Bipolar ablation has been shown in ex vivo models to generate deeper lesions when compared to unipolar ablation. Its use has been reported to target refractory VAs in the interventricular septum and LV ostium/LV summit [10,11,12]. Bipolar ablation may increase the risk of ablation related complications, though with careful power titration and close attention to ablation parameters serious complications can be avoided [10].
Ethanol Ablation
Ethanol ablation delivered into the coronary venous system is an established therapy for mitral annular flutter and atrial fibrillation (vein of Marshall ablation) and has been increasingly used also for VAs. Ethanol ablation targets for VAs include the septal perforator branches and the annular vein in the LV summit [13, 14]. When arrhythmia substrate is identified in a venous branch, occlusion using angioplasty balloons and infusion of ethanol distal to the balloon can result in dense scar in the myocardium drained by the vein (Fig. 3).
Pulsed Field Ablation
Pulsed field ablation is a nonthermal ablative modality that uses ultrashort, high-voltage electrical pulses to create microscopic pores in cell membranes leading to apoptotic cell death. An established therapy for the treatment of atrial fibrillation, there is increasing exploration of this technology for the treatment of VAs [15,16,17]. Preclinical work has demonstrated effective transmural lesion formation in ventricular tissue [18]. Ventricular lesions in a swine model were shown to reach a maximum depth of 9.4 mm [18]. Long-term efficacy and safety profile of this technology remain an area of active investigation.
Ultra-Low Temperature Cryoablation (ULTC)
This novel ablation strategy uses liquid nitrogen cooled catheters capable of reaching − 196 °C, and preclinical trials have demonstrated transmural lesion formation in atrial and ventricular tissue [19]. In the first in-human trial including 13 patients with monomorphic VT, ULTC resulted in acute arrhythmia non-inducibility in 91% of patients [20]. Long-term safety and efficacy of this technology needs further evaluation.
Needle Ablation
Needle ablation uses conventional RF in addition to intramyocardially delivered saline to increase conductive heating of tissue. A specialized catheter is positioned at the site of interest and an extendable needle is advanced up to 8 mm into the tissue [21]. This technique generates intramyocardial lesions with increased lesion size when compared to conventional RF [22]. Studies in patients refractory to conventional catheter ablation show 48% freedom from VAs at 6 months with a further 19% experiencing decreased burden [23]. The complication rate in this 31 patient case series was 23% including pericardial effusion, pulmonary embolism, and LV lead dislodgement [23], highlighting the need for ongoing study.
Stereotactic Radiation
Stereotactic radiotherapy has been explored as an ablation technique for patients with refractory ventricular tachycardia, unsuccessful catheter ablation with advanced techniques, and those that not candidates for catheter ablation [24, 25]. Typically delivered in a single dose of 25 Gy, it has been shown to be effective for decreasing the burden of VT taking between 1 and 7 weeks to reach full efficacy [24]. At present, the recurrence rate for this therapy remains high and it is reserved for patients refractory to catheter ablation or are unable to undergo ablation, and longer-term effects of the radiation are yet unknown [24, 25].
Procedural Endpoints
For PVC ablations, acute procedural success implies complete elimination of spontaneous or inducible PVCs after a waiting time of at least 30 min despite isoproterenol infusion.
For VT ablations, the ideal procedural endpoint is the non-inducibility of any sustained monomorphic VT at the end of the procedure with programmed electrical stimulation. Induction of a nonclinical VT is considered partial success and may be an acceptable outcome if the clinical VTs have been successfully targeted. When VT is not inducible at baseline, surrogate endpoints should be defined, such as elimination of late potentials, ablation of all local abnormal ventricular activities (LAVAs) or core isolation of the arrhythmogenic scar.









留言 (0)