
記住我



In the present work, we applied the Advanced Collapsed Cone Engine (ACE) [30, 31] integrated into the treatment planning system (TPS) Oncentra Brachy (version 4.6.2; Nucletron, Veenendaal, The Netherlands) as MBDCA. Corresponding dose calculations require knowledge about the tissue types and densities present within the anatomical region of interest (ROI). All respective organs and tissues (e.g., bone, lung, air, general soft tissue) therefore have to be contoured on an acquired CT scan and can subsequently be linked to one of the tissues included in a material table predefined by the TPS distributor, which in general refers to Table III of the TG-186 recommendation [24]. Dose calculation can then be performed assuming for each assigned material a uniform density, which is also taken from the aforementioned Table III. This way of dose calculation will be referred to as ACEuniform in the following.
As an alternative, the attenuation characteristics of the materials included in each CT voxel can be considered for dose calculation beyond the assumption of uniformity. For this purpose, the respective CT numbers have to be converted to electron densities as commonly performed for external beam radiation therapy (EBRT). In the used TPS, this conversion is conducted according to Knöös et al. [32]:
$$\begin\rho _=\left(A+\frac}}\right).10^\frac},\\[+2mm]\text\,\begin A=3.30\,\text\,B=\frac\,\text\,CT_}\leq 150\,\mathrm\\ A=3.65\,\text\,B=\frac\,\text\,CT_}> 150\,\mathrm \end \end$$
(1)
ρe and CTnumber refer to the electron density and the voxel’s CT number in Hounsfield units, respectively. A and B represent conversion parameters. The electron density obtained in this way is then directly related to the mass density of the examined tissue, following International Commission on Radiation Units and Measurements (ICRU) reports 44 [33] and 46 [34]. Based on this information, dose calculations considering the attenuation characteristics of each voxel can be performed, which will be referred to as ACECT# in the following.
Both calculations ACEuniform and ACECT# were performed using the Advanced Collapsed Cone Engine (ACE) integrated into our TPS as mentioned above. The description of the underlying algorithm was provided in detail earlier [30, 31, 35,36,37,38] and shall not be repeated here. In brief, it calculates the total dose to the local medium transported through the medium as sum of the dose deposited by primary photons (obtained by a ray tracing procedure) and the dose resulting from single and multiple scattered photons (obtained via a collapsed cone superposition convolution method). Based on this approach, we investigated the suitability of model-based dose calculation on CBCT scans as follows.
CT scanners and CT number phantom examinationsFollowing Eq. 1, a high CT number accuracy is important for the intended model-based dose calculations. In this work, we analyzed the feasibility of achieving this requirement with modern state-of-the-art CBCT compared to conventional CT. As CBCT device, the mobile 3‑in‑1 X‑ray system ImagingRing m (medPhoton, Salzburg, Austria) characterized in detail previously [28, 29] was utilized. Due to its mobility, the device is well-suited for on-site imaging on the brachytherapy ward and was used to acquire control CBCT scans as outlined in section ‘Patient workflow and anthropomorphic phantom study’. For conventional CT imaging, a SOMATOM go.Open Pro scanner (Siemens, Forchheim, Germany) referring to our default system for the acquisition of planning CTs was applied.
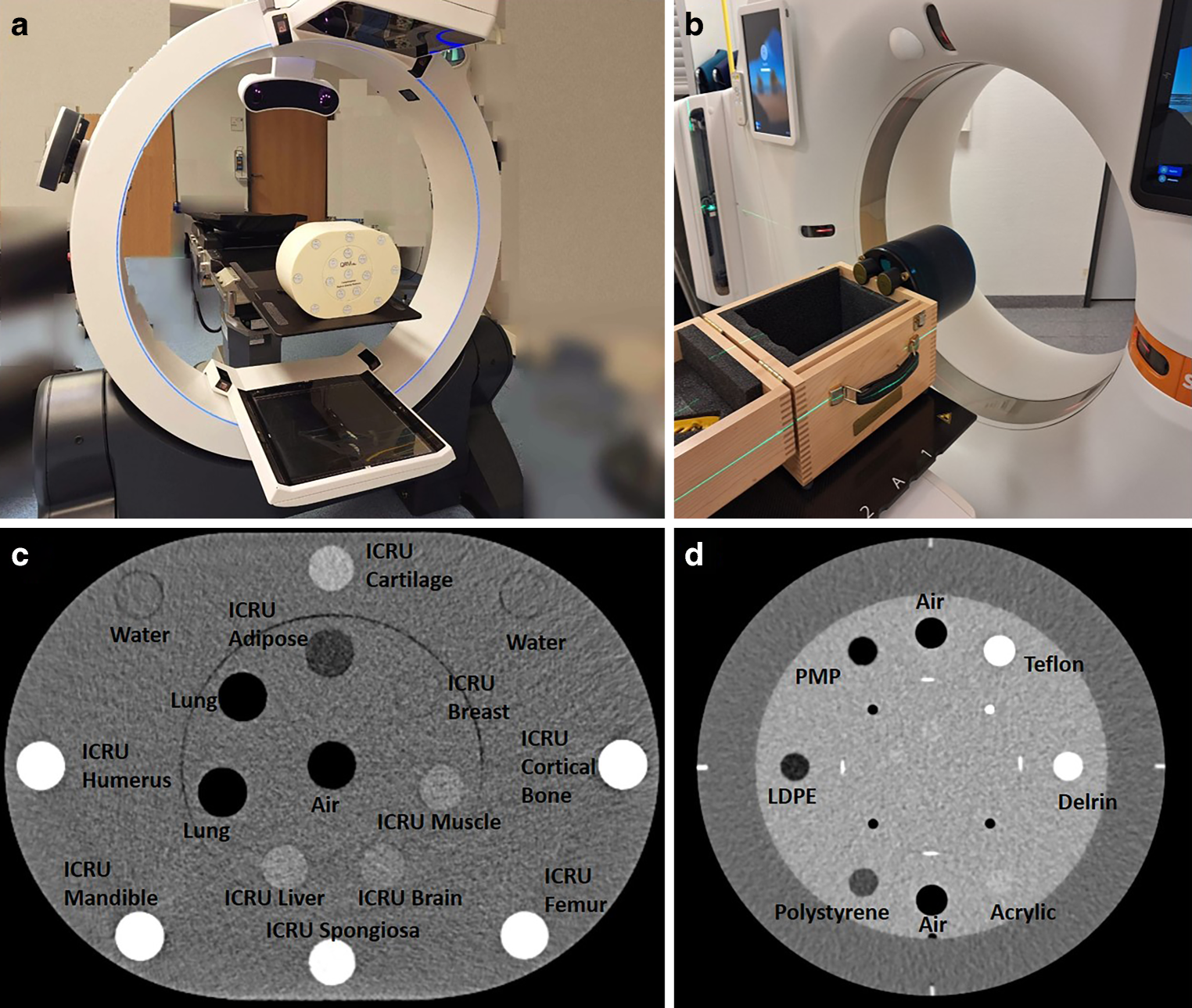
To evaluate CT number accuracy for both machines, phantom studies considering the CatPhan 504 (The Phantom Laboratory, Salem, USA) as well as the Comprehensive Electron Density Phantom (QRM, Möhrendorf, Germany) were conducted first. Both phantoms contain inserts of various materials with different electron densities (provided by the manufacturers) that represented the broad CT number spectrum of a typical human body (Fig. 1). The CatPhan was used since it is a widespread standard quality assurance (QA) phantom in radiotherapy, but comprises only materials with an effective atomic number of approximately seven [39], meaning that bony tissue is not sufficiently represented. To account for this drawback, the Comprehensive Electron Density Phantom was also examined. This is specifically designed [40] to mimic human tissue (including bony structures) regarding electron density according to ICRU report 44 [33] and 46 [34].
Fig. 1
CBCT scanner ImagingRing m (a) and the conventional CT scanner Somatom go.Open Pro (b), with the examined phantoms being exemplarily placed within the gantry. The inserts contained in the Comprehensive Electron Density Phantom (c) and the CatPhan 504 (d) are labeled in each case and represented a broad human body like CT number spectrum. ICRU International Commission on Radiation Units and Measurements
As illustrated in Fig. 1, the two phantoms were placed isocentrically in the CT and CBCT devices and scanned five times each. Scan parameters of the SOMATOM go.Open Pro CT scanner included 120 kV tube voltage, automatic tube–current modulation, continuous radiation output, 0.5 s gantry rotation time, 0.4 × 0.4 × 2 mm3 voxel size, 64 × 0.6 mm collimation, smooth Br40 kernel, and spiral-scanning mode. Scan parameters of the ImagingRing CBCT included 120 kV tube voltage, automatic tube–current modulation, pulsed radiation output with 30 Hz frame rate, 20 s gantry rotation time, 0.4 × 0.4 × 2 mm3 voxel size, 300 μm detector pixel pitch, Shepp–Logan kernel, and circular-scanning mode. No user-selectable artifact reductions were applied for both the CT and CBCT system. It should be noted that based on previous reports [28, 29], the ImagingRing features only heuristic scatter corrections. On the central slice of the acquired images, a circular ROI (10 and 18 mm diameter for the CatPhan and the Comprehensive Electron Density Phantom, respectively, which was about 2 mm smaller than the inserts’ diameter to reduce the impact of CT number fluctuations at their edges) was placed centered within each insert by using an adapted version of the software QAMaster [41] to determine the respective mean CT number. CT numbers and associated electron densities (resulting from Eq. 1) were then compared between the two scanners to estimate the CT number inaccuracies occurring with modern CBCT imaging.
Patient workflow and anthropomorphic phantom studyTo evaluate the impact of CT number uncertainties on model-based dose calculation, we examined 18 cervical and 8 breast cancer patients as well as an anthropomorphic upper torso phantom (Radiology Support Devices, Gardena, CA, USA). Our clinical workflows and the phantom setup are described in the following. All dose calculations performed during treatment planning were based on TG-43 as well as considering an 192Ir radiation source (microSelectron mHDR-v2r source for pulsed dose rate (PDR) treatments; Flexisource 192-Ir source for high dose rate (HDR) treatments; both provided by Nucletron). All image acquisitions were performed as part of our default workflow. No IRB approval or similar was required for the present work.
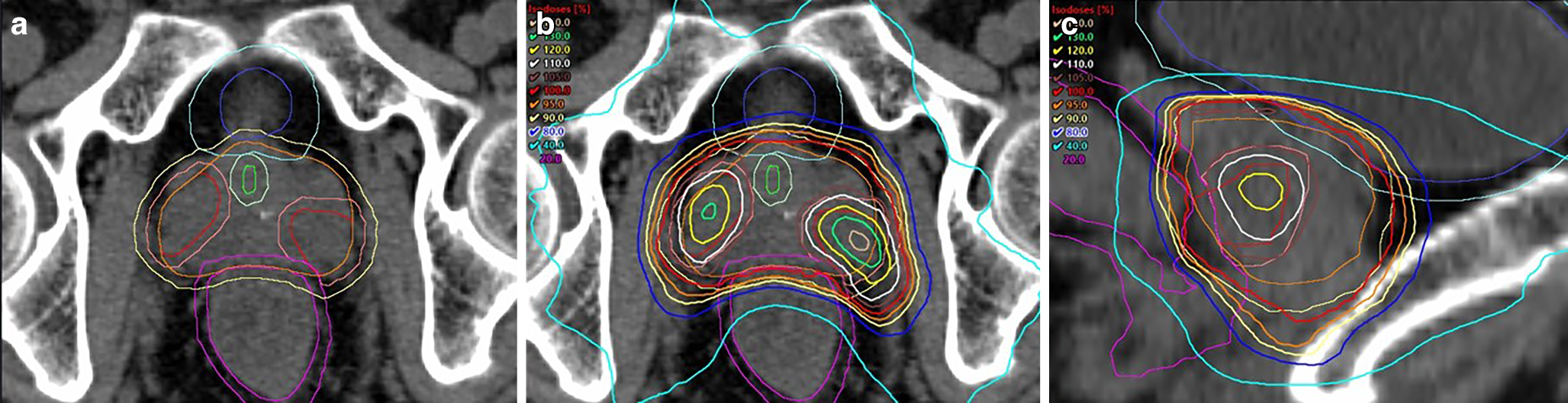
The considered cervical cancer patients received PDR brachytherapy with single doses of 0.6 Gy every hour for 24 h per day up to a total dose of 40–45 Gy as boost following EBRT. For this purpose, a Fletcher applicator was implanted based on intraoperative ultrasound-guidance, accompanied by an interstitial insertion of additional plastic needles in 10 of the 18 cases. Afterwards, high-risk clinical target volume (HR-CTV) as well as organs at risk (OARs; bladder, rectum) were contoured on an acquired planning CT following GEC-ESTRO guidelines [42]. Treatment planning aimed to achieve a HR-CTV D90 (dose the most exposed 90% of the structure volume receive) of ≥ 100% of the prescribed dose, while keeping \(\mathrm_^}}\) (EQD2) of bladder and rectum below 85 and 75 Gy, respectively (including EBRT exposure). A typical case and planned dose distribution is shown in Fig. 2a, b. At about halfway through the brachytherapy course, a control CBCT was acquired to assess potential geometric implant variations as described previously [10].
Fig. 2
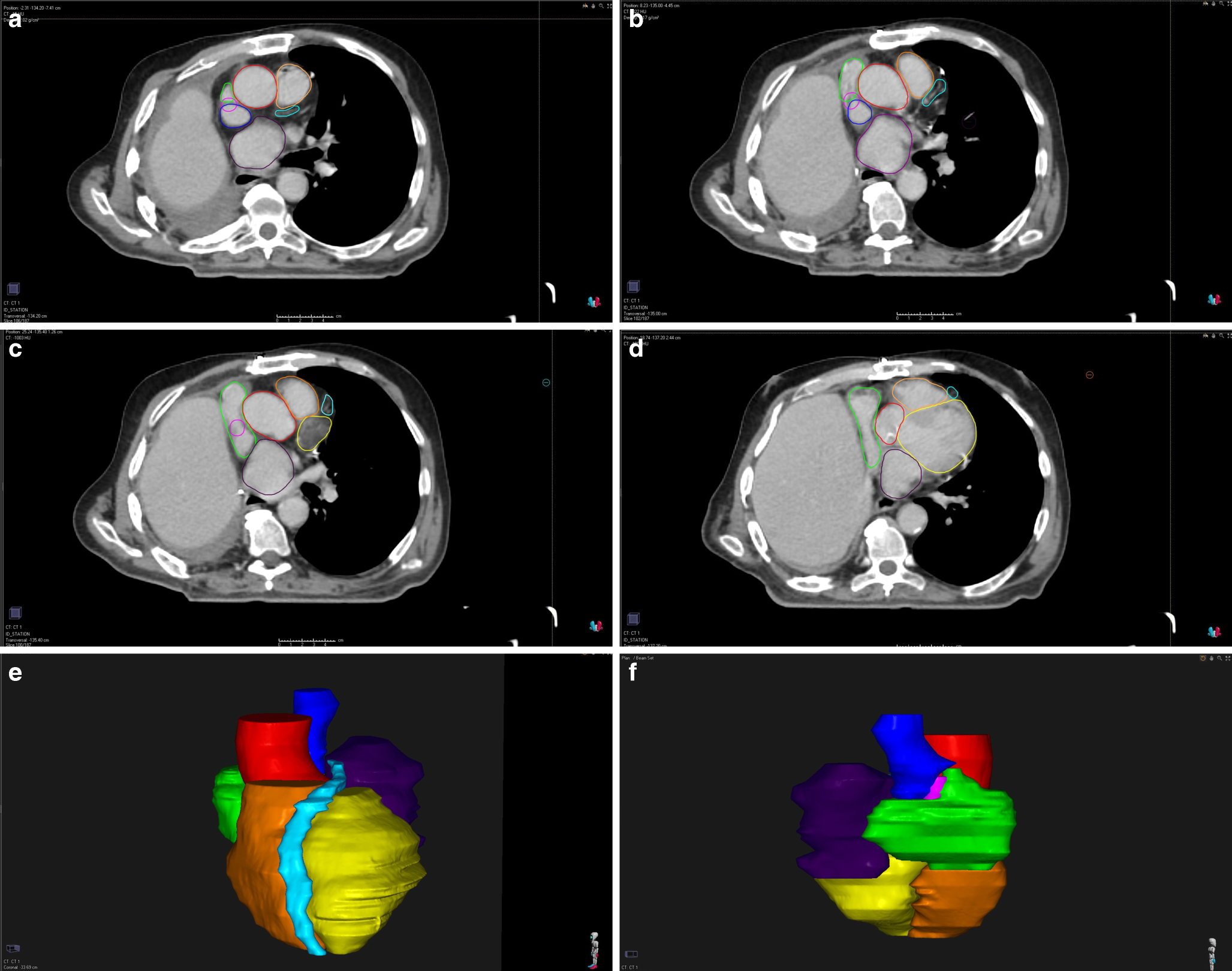
Three-dimensional representations of a typical cervix (a), breast (c), and phantom surface (e) case with reconstructed applicators (blue) and target volumes (red) to provide an impression of the dose distributions examined in the present work. For the cervix case, bladder and rectum are additionally shown in yellow and green, respectively. The dose distributions planned for the cervix (b), breast (d), and phantom (f) case are shown as well. Here, the red, yellow, cyan, blue, and green lines refer to the 100, 120, 150, 200, and 70% isodose curves, respectively. The corresponding target volume is shown as filled red contour
The examined breast patients received HDR multicatheter brachytherapy considering the recently reported workflow [8] and a fractionation of 9 × 3.8 Gy. The interstitial insertion of plastic catheters into the breast (which were fixed with plastic buttons at the skin to avoid slippage) was followed by a planning CT acquisition, on which planning target volume (PTV) and OARs (ribs, skin) were delineated according to GEC-ESTRO guidelines [43]. Treatment planning aimed to achieve a PTV D90 ≥ 100% of the prescribed dose. Ribs \(\mathrm_^}}\) and \(\mathrm_^}}\) as well as skin \(\mathrm_^}}\) and \(\mathrm_^}}\) should receive < 80% and < 90% as well as < 90% and < 100% of the prescribed dose, respectively. A typical patient case is exemplarily shown in Fig. 2c, d. After the fourth irradiation fraction, a control CBCT was acquired to detect implant variations as described previously [8].
Furthermore, since we currently acquire no control CBCTs of our patients suffering from superficial tumors, the aforementioned upper torso phantom was utilized. The phantom simulates a human thorax and comprises, next to Rando plastic simulating soft tissue, particularly artificial ribs and lung. On top of the phantom chest (Fig. 2e, f), we fixed in succession six different Freiburg flaps (Elekta, Veenendaal, The Netherlands) of sizes 5 × 10 cm2 to 9 × 20 cm2 using tape to avoid slippage. A planning CT was acquired in each case to contour a 1–2 mm deep PTV with the planar dimension of the respective flap right underneath this flap. No OARs were considered following our clinical workflow of treating corresponding patients. Afterwards, a treatment plan with PTV D90 ≥ 100% for a PDR treatment with 100 pulses of 0.5 Gy (irradiated every hour) up to a total dose of 50 Gy was created. Moreover, we acquired for each fixed flap a corresponding CBCT scan to assess CBCT-based dose calculations for these superficial treatments as well.
Analysis of dosimetric implant alterationsTo analyze dosimetric variations during the treatment course for each entity and patient, the respective OARs were recontoured on the control CBCT and the target volume was transferred to the latter from the planning CT. For cervix patients, this was based on a rigid registration of the Fletcher applicator within Oncentra Brachy. For breast patients, the target volume transfer was performed by means of a deformable image registration within RayStation (RaySearch, Stockholm, Sweden) [6], after which the image and associated structure data sets were reimported in Oncentra Brachy for dose calculations. In each case, the goodness of these transfer procedures was evaluated by assigning the registration quality score described in the AAPM TG-132 report [44].
Subsequently, the treatment plan (i.e., the dwell positions and times of the source) was transferred to the applicator arrangement obtained on the control CBCT. The resulting dose distribution was then compared to the initial treatment plan considering the dose metrics mentioned in the section ‘Patient workflow and anthropomorphic phantom study’ as well as the volumes V100 and V150 enclosed by the 100 and 150% isodose surfaces, respectively. These clinical assessments and comparisons were conducted solely based on TG-43 dose calculations.
For the anthropomorphic phantom, no corresponding evaluation was performed due to the absence of implant variations in this case and in order to avoid a misinterpretation of the results with respect to clinical patients. Nevertheless, the respective target volume was transferred from the planning CT to the control CBCT by means of a rigid registration of the phantom surface within Oncentra Brachy for the following investigations (section ‘Comparison of dose calculation methods’). Registration quality was assessed as above.
Comparison of dose calculation methodsAs final step of the present work, to assess the suitability of Advanced Collapsed Cone Engine dose calculations based on CBCT images, we recalculated the TG-43 dose distributions created on both planning CTs and control CBCTs by means of ACEuniform and ACECT#. All ACE calculations were performed with the standard resolution setting of Oncentra Brachy being selected. For this purpose, following tissues/materials listed in Table III of the TG-186 recommendation [24] were manually contoured on the CTs and CBCTs as required according to section ‘Advanced collapsed cone engine dose calculation’:
For cervix cases: bones, air, and general female soft tissue;
For breast patients: bones, skin, air, lung, and general female soft tissue; and
For the phantom cases: bones, air, lung, and general female soft tissue.
All three dose distributions (TG-43, ACEuniform, ACECT#) were compared to each other on both planning CTs and control CBCTs considering the dose metrics mentioned above. In this respect, the comparison of TG-43 to ACEuniform enabled a quantification of the dosimetric impact of the varied dose calculation algorithm itself. The dosimetric effects of explicitly considering the CT numbers of each voxel were assessed by comparing ACEuniform to ACECT#. Statistical significance of found deviations was tested using a Wilcoxon signed-rank tests at 5% significance level. The comparison of the ACEuniform–ACECT# variations between planning CT and control CBCT served for evaluating the suitability of CT-number-based dose calculations on CBCT images compared to conventional CT. The differences in these variations were tested for statistical significance by means of Mann–Whitney U tests at the 5% significance level.
留言 (0)