
記住我





This prospective observational study included patients at our institution between January 2019 and December 2021 who had an elbow dislocation associated with fractures of the radial head and CP. The inclusion criteria for final statistical analysis were defined as follows: patients underwent repair of the CP, radial head, and LUCL with a minimum of 2 years of follow-up. Exclusion criteria were (1) a trans-olecranon fracture dislocation, (2) a Monteggia fracture, (3) an associated upper-limb fracture at the ipsilateral side, or (4) an open fracture. The following data were collected: patient characteristics, injury mechanisms, fracture types, and fixation methods used for radial head and CP fractures. This study was approved by the institutional review board of our institution (no. 2019-09-013AC) and conducted in accordance with the ethical principles of the 1964 Declaration of Helsinki.
Surgical protocolBefore surgery, computed tomography with three-dimensional reconstruction was universally performed to delineate the fracture pattern, comminution, and classification of the radial head and CP fracture. CP fractures were classified on the basis of the Regan–Morrey and O’Driscoll classification systems [23, 24], and radial head fractures were classified on the basis of the original Mason classification system because all such fractures would be classified as type IV in the Mason–Johnston system [25, 26]. In the original Mason classification system, type I indicates nondisplaced or small marginal radial head fractures, type II indicates partial articular fractures with > 2 mm of displacement, and type III indicates comminuted fractures involving the entire radial head.
Figure 1 depicts our standard surgical protocol for TTIE. To assess elbow stability, an examination under anesthesia (EUA) was performed for all patients. A dorsally directed force relative to the humerus was applied to the forearm with the forearm in neutral rotation. Elbow instability was defined as the occurrence of any posterior or posterolateral subluxation/dislocation within a 20–130° flexion–extension arc (Fig. 2) [9].
Fig. 1
Protocol for operative treatment of terrible triad injuries of the elbow. LUCL lateral ulnar collateral ligament, MCL medial collateral ligament
Fig. 2
An example of instability defined by examination under anesthesia. A preoperative radiograph revealed posterior subluxation of the ulnohumeral joint during a test in a patient with terrible triad injury of the elbow
For patients with a stable elbow, an isolated lateral Kocher approach was adopted for radial head repair or replacement and LUCL repair without CP fixation. By contrast, for those with an unstable elbow, a systematic CP repair was performed first through an anterior approach. Then, the radial head and LUCL were repaired by the Kocher approach. If instability persisted, the MCL was exposed through a medial incision and repaired. A hinged external fixator was used if patient had residual instability after MCL repair.
Surgical techniqueAll surgical procedures were performed by a single orthopedic trauma specialist. During the procedures, the patients were in the supine position and under general anesthesia. Our anterior approach for CP fixation is illustrated in Fig. 3. An S-shaped incision was made, starting from 2 cm proximal to the radial aspect of the elbow flexion crease, curving across the antecubital fossa, and ending at 2 cm distal to the ulnar side of the elbow crease. After subcutaneous blunt dissection, the cephalic vein, basilic vein, median cubital vein, and medial antebrachial cutaneous nerve were identified and retracted. Then, the pronator teres, biceps, and lacertus fibrosus were exposed. The lacertus fibrosus was transversely incised to reveal the brachial artery and median nerve. Unlike the traditional anterior approach, which involves the medial retraction of both the brachial artery and median nerve to disclose the brachialis, our approach involved creating an interval between the brachial artery and median nerve; this technique considerably reduced soft-tissue tension, further exposing the brachialis muscle. Our approach is theoretically safe because this space accommodates no neurovascular branches [27]. The brachial artery and biceps were laterally retracted, whereas the median nerve and pronator teres were medially retracted. A longitudinal incision was made at the brachialis and its tendon. The capsule was opened, exposing the entire CP fragment. After anatomic reduction under direct visualization, fixation with a 4.5-mm suture anchor was performed for a tip avulsion fracture, whereas a mini buttress plate, usually for a metacarpal or a 4.5-mm anteroposteriorly directed interfragment screw, was used for larger fragment. The lateral Kocher approach was used to address the radial head and LUCL. We preferred radial head fixation over replacement, even for Mason type III fractures. Ultimately, the LUCL was reattached to its anatomic origin on the lateral humeral epicondyle by using a 4.5-mm suture anchor. Figures 4 and 5 demonstrate a case in which our protocol and surgical technique for TTIE treatment was used.
Fig. 3
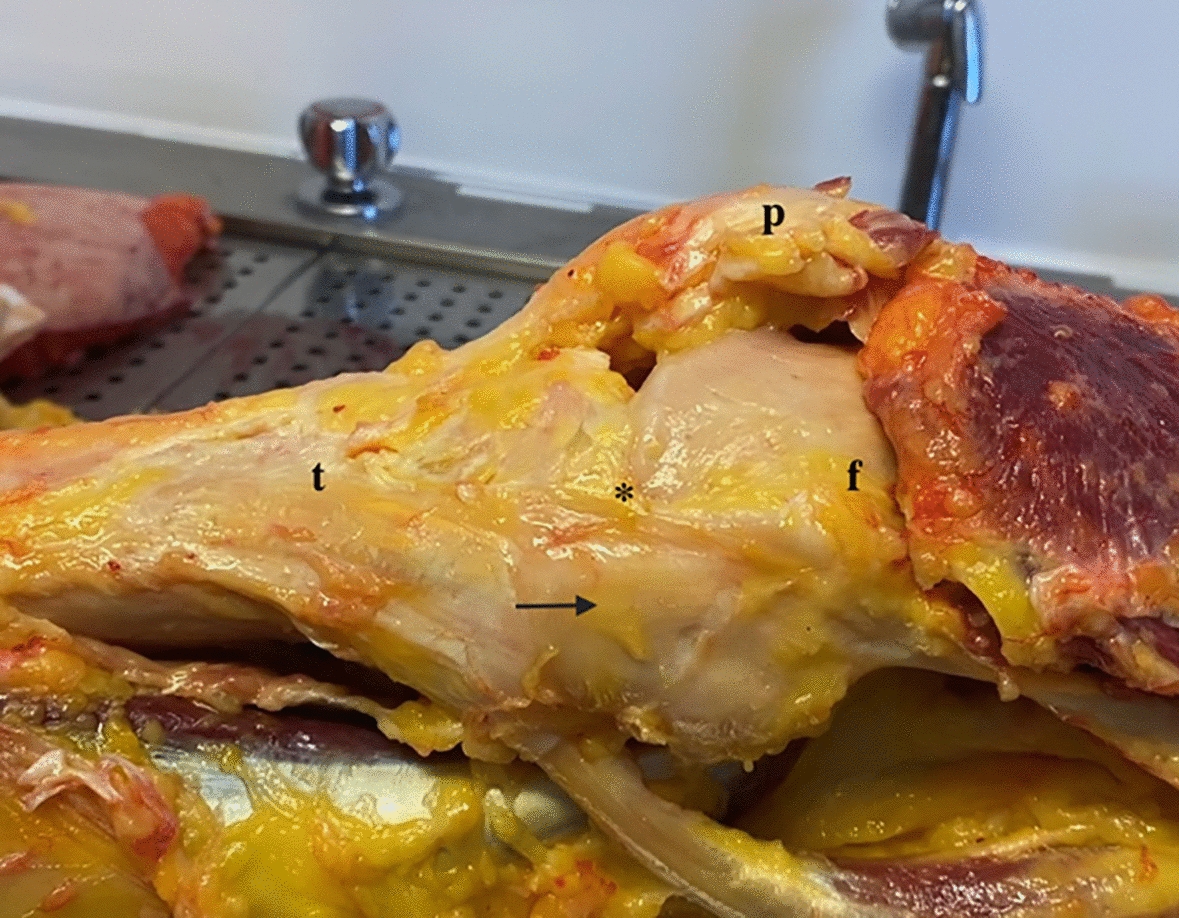
A cadaveric left elbow was utilized to illustrate our anterior approach for the coronoid process. A A curve incision (dotted yellow line) was made at the cubital fossa, starting from the proximoradial aspect of elbow flexion crease and extending to the distoulnar side of the elbow crease. After subcutaneous dissection, the bicep and its tendon, the pronator teres, and the lacertus fibrosus were exposed. B The lacertus fibrosus was transversely incised to reveal the underlying brachial artery and median nerve. C The interval between brachial artery and median nerve was created by mosquito forceps. D The brachial artery was retracted laterally, while the median nerve and pronator teres were retracted medially. The underlying brachialis was exposed. E The brachialis and its tendon was longitudinally incised. The capsule was opened and the whole coronoid process could be visualized. B biceps, Ba brachial artery, Br brachialis, BT biceps tendon, C coronoid process, Cau caudal, Cep cephalic, FCR flexor carpi radialis, H humerus, L lateral, LF lacertus fibrosus, M medial, Mn median nerve, PT pronator teres
Fig. 4
Case demonstration from our cohort. A, B Preoperative radiograph disclosed a 51-year-old patient with left terrible triad injury of the elbow; C–F computed tomography and three-dimensional reconstruction images revealed a Mason type II radial head fracture. The coronoid process fragment included the tip and anteromedial facet with less than 50% of the coronoid height (Regan–Morrey II) involved; G, H posterior subluxation of the ulnohumeral joint was observed during examination under anesthesia. I, J Radiograph at 2 years postoperatively. The patient first underwent coronoid process repair through an anterior approach. The radial head and lateral ulnar collateral ligament were addressed by the Kocher approach after coronoid process fixation
Fig. 5
The patient in Fig. 4 at the 2-year follow-up. A, B Surgical wounds for the anterior and lateral approaches. The anterior incision can be much smaller in experienced hands. Only the ulnar portion of the S-shaped incision in Fig. 3A is required for adequate coronoid process exposure. C–F Forearm supination
Postoperative managementPostoperatively, the patients received indomethacin (dosage: 25 mg thrice daily for 3 weeks) for heterotopic ossification prophylaxis. Celecoxib 200 mg once a day was given to relieve pain and allow early elbow rehabilitation. A supervised rehabilitation protocol was initiated at postoperative day 1 by our physical medicine and rehabilitation specialist. The patients performed functional exercises involving active elbow flexion and extension and forearm rotation. Active elbow flexion and extension and forearm rotation functional exercises lasting for 30 min were performed three times a day with a gradual range of motion increment. A hinged plaster splint was used for 8 weeks after the surgery. During the first 2 weeks, the elbow was immobilized at 90° flexion, with the forearm in neutral rotation outside the exercise period. For the next 6 weeks, the elbow flexion and extension parameters in the hinged splint were set as follows: 30–110° for 2 weeks, 20–120° for 2 weeks, and 10–130° for 2 weeks, followed by the full range of motion.
Follow-up radiographic and clinical assessmentThe patients underwent clinical and radiographic assessments at 1, 3, 6, 12, and 24 months postoperatively. Evidence of recurrent subluxation/dislocation, synostosis, heterotopic ossification, nonunion, implantation failure, and traumatic arthritis was documented from the follow-up radiograph. The elbow flexion and extension arc, range of forearm supination and pronation, and functional outcome as determined using the Mayo Elbow Performance Score (MEPS) and the Disabilities of Arm, Shoulder and Hand (DASH) score were assessed at the 3-, 6-, 12-, and 24-month follow-ups. The MEPS indicates elbow function based on measurements of pain, stability, movement, and daily activities. The total score is 100, and higher scores reflect better results, with greater than 90 being excellent, 75–89 good, 60–74 fair, and less than 60 poor. The DASH score (30 items rated on a scale of 1–5) rates the disability of the upper limb. Higher scores indicate poorer outcomes. In the current study, complications such as superficial and deep surgical wound infections and postoperative neuropathy were recorded at the follow-up visits. Stiffness was defined as the absence of a 30–130° flexion–extension arc and 100° of forearm rotation [28].
Statistical analysisThe patients’ range-of-motion angles and functional scores were expressed in terms of the mean ± standard deviation. Statistical analyses were performed using SPSS (version 22; SPSS Statistics, IBM, Armonk, NY, USA).
留言 (0)