
記住我
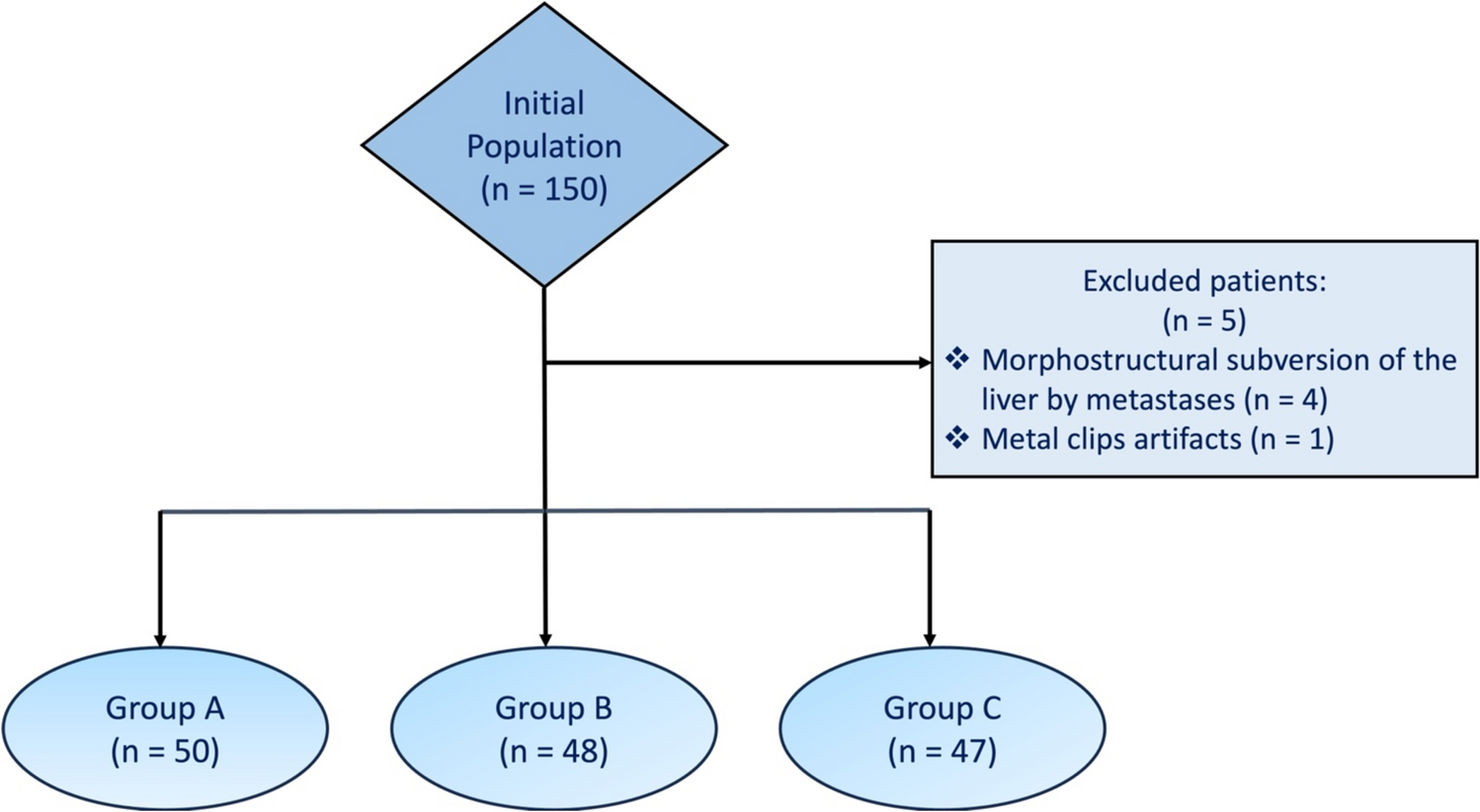





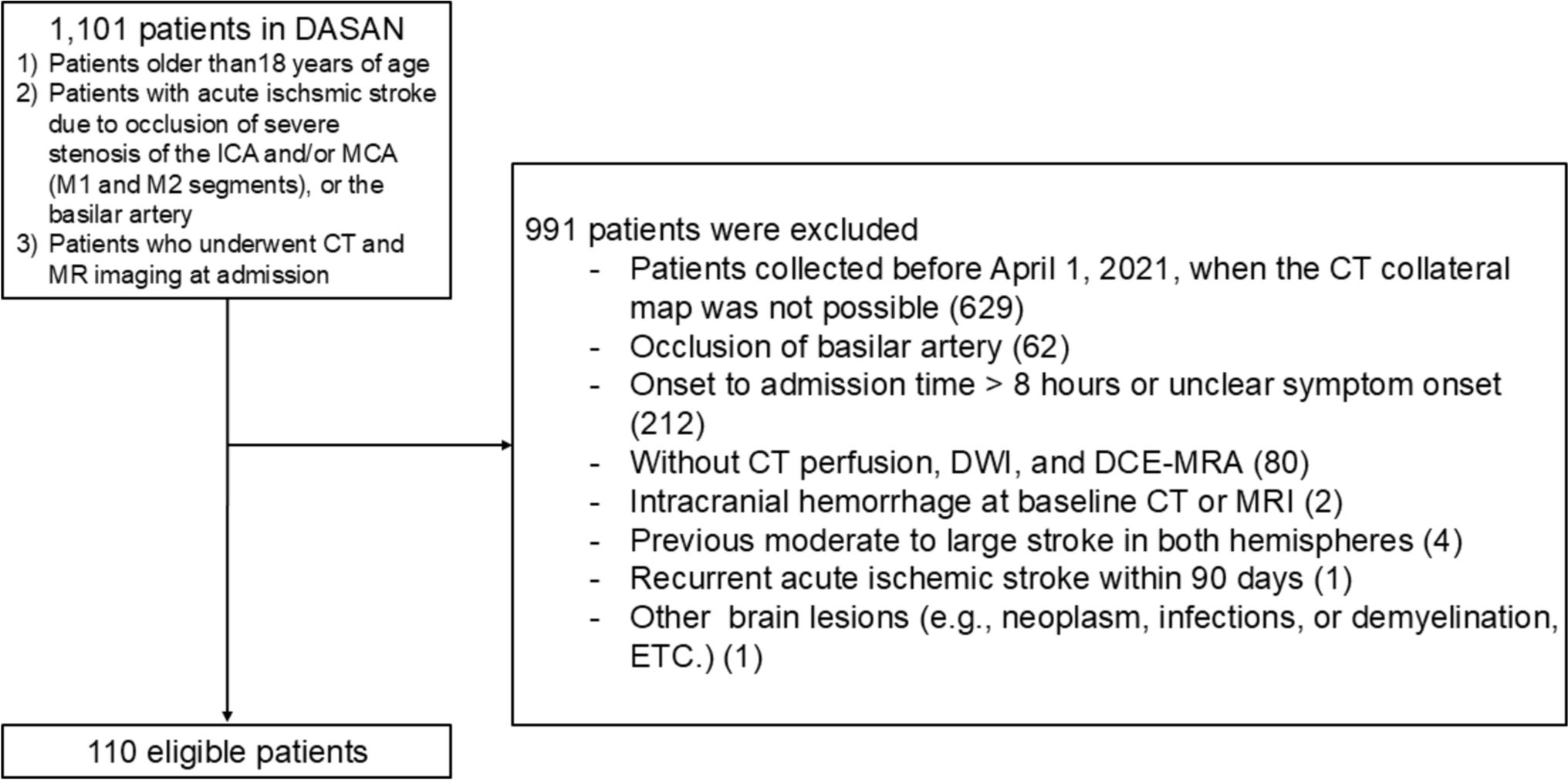
A total of 52 patients were included in this study (Fig. 2) with a mean age of 53.9 ± 19.6 [SD] years (range 7–83 years), comprising 41 males (78.8%) and 11 females (21.2%). Out of these patients, 12 (23.1%) had hereditary hemochromatosis (HH), while the remaining 40 (76.9%) were diagnosed with acquired hemochromatosis (AH). The most common underlying condition for AH was dysmetabolic iron overload syndrome (DIOS, n = 30, 75.0%), followed by myelodysplastic syndromes (n = 5, 12.5%), repeated blood transfusions (n = 4, 10.0%), and hemoglobinopathy (n = 1, 2.5%). All patients with HH had a type 1 HH (HFE-related) (4). Baseline characteristics and group comparison are shown in Table 2.
Fig. 2 Table 2 Baseline characteristics of the study populationBody fat composition and LIC
Table 2 Baseline characteristics of the study populationBody fat composition and LICThere was no statistically significant difference between the acquired R2* measurements from the ROI (172.9 ± 142.8 s⁻1 [SD], range 13.6–788.4 s⁻1) and from the whole liver volume (155.8 ± 92.3 s⁻1 [SD], range 31.3–484.9 s⁻1; p = 0.560).
IMF showed a positive correlation with R2* values measured in the ROI (p = 0.005, rs = 0.382) and for the entire segmented liver volume (p = 0.016, rs = 0.332) (Fig. 3). Conversely, VSF showed a negative correlation with R2* values from the ROI (p = < 0.001, rs = − 0.488) and from the entire segmented liver volume (p = < 0.001, rs = − 0.459). Additionally, a positive correlation was observed between IMF-to-VSF ratio and R2* of the ROI (p = 0.003, rs = 0.400) and the whole segmented liver (p = 0.008, rs = 0.364) (Fig. 4). SCF-to-VSF ratio exhibited a similar positive correlation with R2* values measured in the ROI (p = 0.04, rs = 0.394) and the whole liver (p = 0.06, rs = 0.376).
Fig. 3
Correlation between IMF and VSF to R2* values calculated from a ROI placed in the right lobe and form the whole segmented liver volume. IMF Intermuscular far, VSF Visceral fat, ROI Region of interest
Fig. 4
Correlation between ratios of IMF-to-VSF and SCF-to-IMF to R2* values calculated from a ROI placed in the right lobe and form the whole segmented liver volume. IMF Intermuscular far, VSF Visceral fat, ROI Region of interest
HH group had a stronger negative correlation between VSF and R2* values from the ROI (p = 0.011, rs = − 0.699) and whole liver (p < 0.001, rs = − 0.895) in comparison to AH group (ROI p = 0.003, rs = − 0.455, whole liver p = 0.024, rs = − 0.357). AH group had statistically significant correlation between IMF and R2* values from the ROI (p = 0.013, rs = 0.388) and whole liver (p = 0.038, rs = 0.330), while HH showed only a non-statistically significant positive correlation (ROI p = 0.471, rs = 0.231, whole liver p = 0.217, rs = 0.385). Complete results are shown in Tables 3 and 4.
Table 3 Body fat distribution percentages, R2* relaxation times and estimated LIC of the study populationTable 4 Results of the performed spearman correlation analysis between PDFF, R2* values, body fat composition and standard iron laboratory parameters Iron laboratory parametersA negative correlation was observed between VSF and ferritin values (p = 0.012, rs = − 0.349), while a positive correlation existed between transferrin values and TF (p < 0.001, rs = 0.457). Ferritin showed a positive correlation with R2* values calculated from ROI (p = 0.002, rs = 0.417) and the entire liver volume (p = 0.004, rs = 0.397). No significant correlation was observed between R2* values and serum iron, transferrin, or transferrin saturation. Complete results are shown in Tables 3 and 4.
Impact of hemochromatosis typeIn multiple linear regression after adjustment for confounding factor (hemochromatosis type) the associations were still significant between R2* ROI and VSF (β = − 0.39, 95% CI − 0.21 to − 0.04, p = 0.005) and IMF (β = 0.32, 95% CI 0.05 to 0.69, p = 0.024), whereas the association to SCF was without statistical significance (β = 0.27, 95% CI − 0.01 to 0.25, p = 0.052). Similarly, the association between R2* from the whole liver and SCF (β = 0.30, 95% CI 0.02 to 0.37, p = 0.031) and VSF remained significant (β = − 0.37, 95% CI − 0.28 to − 0.04, p = 0.008), while the association with IMF lost its statistical significance (β = − 0.26, 95% CI − 0.03 to 0.88, p = 0.064).
The association between VSF and ferritin remained statistically significant (β = − 0.35, 95% CI − 0.14 to 0.02, p = 0.012), same as between TF and transferrin (β = 0.48, 95% CI 26.57 to 15.78, p < 0.001). Additionally, the association between ferritin and R2* ROI (β = 0.59, 95% CI 0.48 to 1.10, p < 0.001) and R2* form the whole liver (β = 0.52, 95% CI 0.51 to 1.43, p < 0.001) remained statistically significant.
Liver steatosisBy visual assessment, liver steatosis was present in 32.07% (n = 17) of the patients, with no significant difference between the HH (33.33%, n = 4) and AH (32.50%, n = 13, p = 0.608). Lower signal intensity in the in-phase sequence was present in 12 patients (23.10%), with no difference between HH (33.33%, n = 4) and AH (20.00%, n = 8, p = 0.437). A statistically significant difference was observed between the PDFF measurements from the ROI (11.6 ± 10.7% [SD], range 0.2–37.3%) and the whole liver volume (15.4 ± 10.9% [SD], range 2.1–38.9%; p < 0.001).
A positive correlation was noted between the PDFF of the entire liver and TF (p = 0.024, rs = 0.313) and between BMI and PDFF from the ROI (p = 0.022, rs = 0.331). There was no statistically significant correlation between R2* values from the ROI and PDFF measured in the ROI (p = 0.580, rs = 0.079) or the entire liver volume (p = 0.775, rs = 0.041). Correlation between PDFF and laboratory iron parameters is shown in Table 4.
Liver morphologyThe ML liver diameter showed a positive correlation with VSF (p = 0.031, rs = 0.300), TF (p < 0.001, rs = 451), BMI (p < 0.001, rs = 0.649), and a negative correlation with the SCF-to-VSF ratio (p = 0.024, rs = − 0.313). BMI also showed a positive correlation with AP (p = 0.037, rs = 0.303) and CC (p = 0.045, rs = 0.291) liver sizes. R2* values from the ROI had a negative correlation with liver AP (p = 0.022, rs = − 0.316), ML (p = 0.043, rs = − 0.281), and CC diameters (p = 0.014, rs = − 0.339). Similar results were found for R2* values estimated from the whole liver regarding AP (p = 0.011, rs = − 0.351), ML (p = 0.071, rs = − 0.253), and CC liver diameter (p = 0.005, rs = − 0.339).
The liver surface was graded as smooth in 47 (90.4%) patients, slightly irregular in 4 patients (7.7%) and nodular in 1 patient (1.9%). The liver parenchyma was homogenous in 32 patients (61.5%), moderately inhomogeneous in 18 patients (34.6%), and strongly inhomogeneous in 2 patients (3.8%). There were no significant differences between groups regarding liver surface (p = 0.074) and parenchyma homogeneity (p = 0.329). Furthermore, there was no statistical significance regarding liver surface and R2* values (ROI p = 0.883, whole liver p = 0.356). Additionally, no statistical significance was observed for parenchymal homogeneity and R2* values (ROI p = 0.802, whole liver p = 0.584).
留言 (0)