
記住我






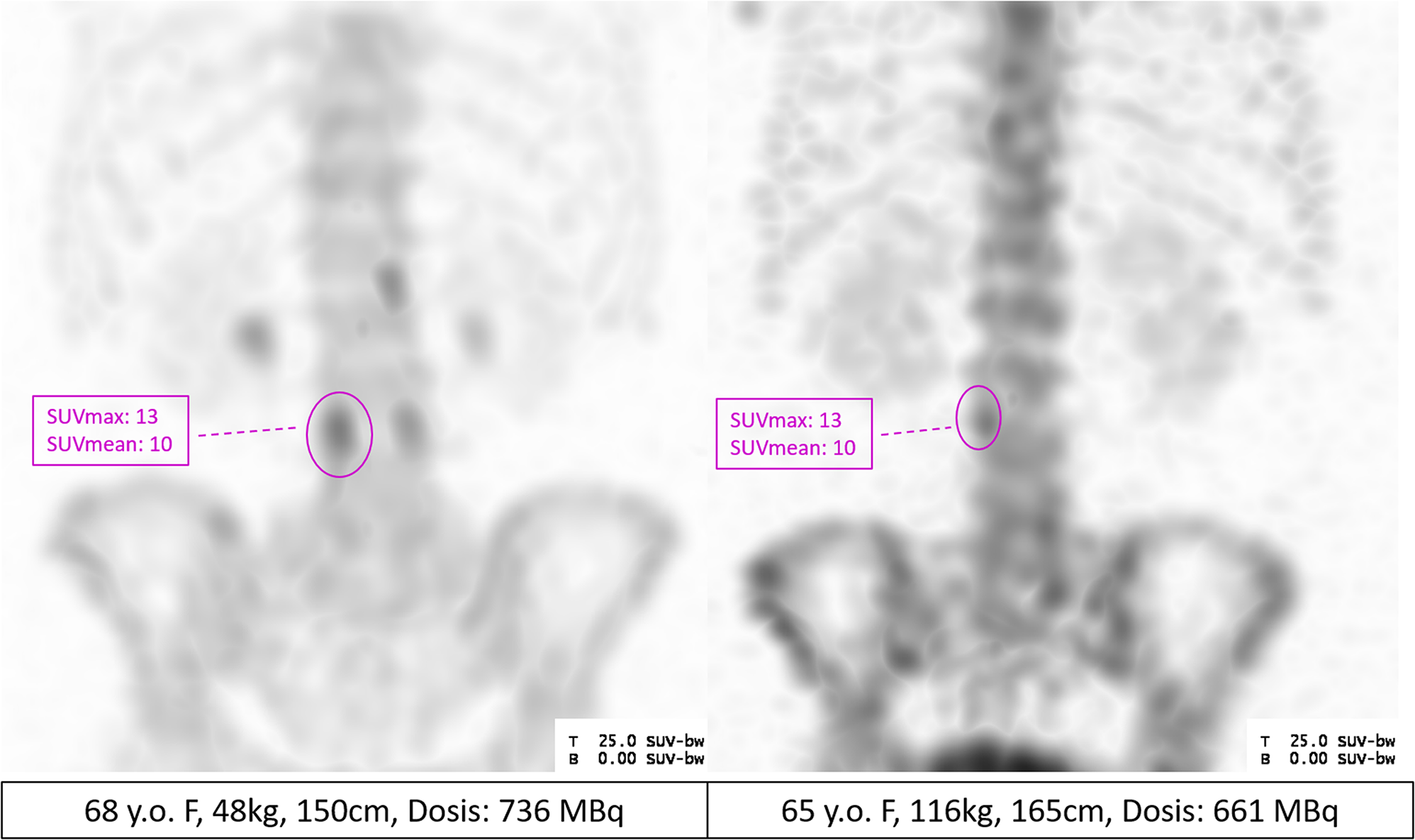
Between January 1, 2019, and August 1, 2023, a total of 843 SPECT/CT scans of the lumbar spine were performed on patients who consented to further data use. From these, 119 patients were selected for this study based on their BW, 66 females and 53 males. Among women over 100 kg, only 6, and for men over 100 kg, only 12 out of 20 could be included. Furthermore, there was only one male patient with a BW below 60 kg. The demographic data, mean activity (kBq/cc), mean bone density (HU), and standardized uptake values for BW (SUVBW) of the patients are presented in Table 1.
Correlation between bone uptake and weight, height, age and bone densityThere was a strong negative correlation between BW (r = -0.64, p < 0.001), weak correlation with height (r = -0.28, p = 0.002), and age (r = -0.34, p = 0.001) with mean tracer uptake in L1 (Fig. 3A-C). These correlations were also observed in L5 and the femoral head (Supp. Figs. 1 and 2). Interestingly, age showed a positive correlation with uptake in the femoral head (Supp Fig. 2). In the lumbar spine (L1 and L5), there was a strong positive correlation between bone density and tracer accumulation, with a weak, but significant correlation of 0.35 for L1 and 0.32 for to L5, (p < 0.001, Fig. 3D, Supp Fig. 1).
Fig. 3
Scatterplots of L1-activity in kBq/cc and body weight, height, age and HU. A simple linear regression line (L1 activity ∼ x) is included for orientation, the strongest correlation was found for body weight (r= -0.64, p < 0.001), compared to an only weak correlation for height (r = -0.28, p = 0.002) and age (r = -0.34, p = 0.001). Density had a weak positive correlation (r = 0.35, p < 0.001)
Correlation between bone density (HU) and weight, height and ageThere was only a very weak association between weight and L1 density (HU) with a correlation coefficient of 0.12 (p = 0.18), and no significant correlation with height (r = 0, p = 0.91) (Fig. 4A and B). However, age showed a strong negative correlation with bone density on CT (r = -0.61, p < 0.001) (Fig. 4C).
Fig. 4
Scatterplots of L1 Density (HU) in relation to body weight, height, age. A simple linear regression line (L1 density ∼ x) is included for orientation. Weight has a very weak positive correlation (r = 0.12, p = 0.18), while there was no correlation with height (r = -0.001, p = 0.91). Age had a strong negative correlation between bone density and age (r = -0.61, p < 0.001)
Correlation between SUVBW and weight, height, age and HUAfter normalizing for BW, a very weak overestimation of L1 activity in patients with higher BW was observed (r = 0.15, p = 0.09), not reaching statistical significance (Fig. 5A). Variance in normal uptake remained high among patients even after this normalization. Furthermore, there was also a very weak positive correlation with height (r = 0.18, p = 0.047). The negative correlation with age deepened (r = -0.5 vs. r =-0.34), and the positive correlation with L1 density increased (r = 0.53, vs. r = 0.35) after normalization to BW (Fig. 5B-D). These findings suggest that in addition to BW, age and bone density are also associated with regular bone uptake.
Fig. 5
Relation between L1 SUVBW and weight, height, age, HU. A simple linear regression line (L1 SUV ∼ x) is included for orientation. Weight (r = 0.15, p = 0.09) and height (r = 0.18, p = 0.047) had very weak positive correlations with L1 SUVBW. Age (r = -0.5, p = < 0.001) had a negative, and L1 Density had a positive moderate correlation with L1 SUVBW (r = 0.53, p = < 0.001)
Model to incorporate clinical parametersBased on these observations, a multiple regression analysis was modeled with L1 activity as the dependent variable, incorporating both linear and squared terms of weight, age, height, and bone density as independent variables. The analysis highlighted weight, age, and bone density as significant predictors (Fig. 6).
Fig. 6
Correlation between L1 activity and weight (kg) (A), density (HU) (B) and age (y) (C) with the multiple regression predictions as well as their prediction intervals (D, E, F). A simple linear regression line (L1 activity ∼ x) is included for orientation (A–C)
A correction formula was derived based on model coefficients in relation to BW, age, and density, and applied to original activity values. The formula for the correction factor incorporated squared and linear terms for age, HU, and weight as follows:
$$\begin\text\text\text\text\text\text\text\text\text\text&=\:-(-\hspace0.003\:*\:\text\text}^+\hspace0.26\:*\:\text}^\\&-\hspace2.1*\:\text\text\text\text\text\text\hspace+\hspace0.01\:*\:\text\text\text\text\text}^)\:\--\:100\end$$
With this a more robust, less dependent estimation of normal bone activity was achieved, with non-significant correlations (r < 0.1) between all parameters and bone activity in L1 (Fig. 7).
Fig. 7
Scatterplots between the corrected uptake values and weight, height, age and L1 Density (HU). A simple linear regression line (correction ∼ x) is included for orientation. The correlations between the corrected uptake values and weight (r = 0.006, p = 0.94), height (r = 0.002, p = 0.94), age (r = 0.009, p = 0.92), and L1 density (r = 0, p = 1, “none”) were very weak
Mixed model for patient-specific effectsIn our mixed-effects model, where patients were included as random intercepts, the adjusted intraclass correlation coefficient (ICC) was 0.74, and unadjusted 0.27, indicating a strong dependence of observations within one patient when measured clinical variables are included.
留言 (0)