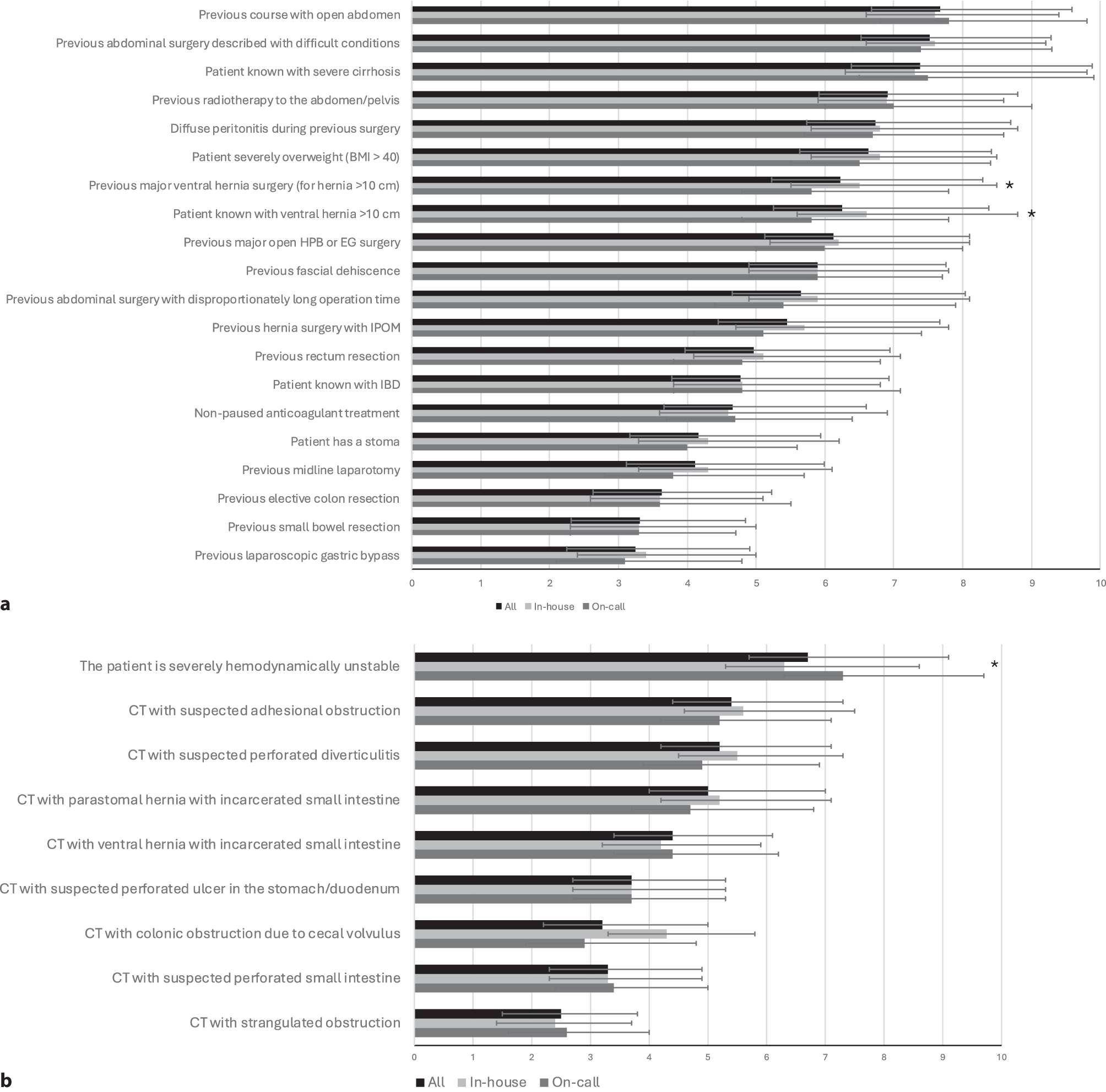
Emergency abdominal surgeries present considerable challenges due to their unpredictable nature and the potential for high postoperative complications and mortality rates, particularly in elderly and frail patients. This study investigated surgeons’ expectations regarding how the knowledge they gain about the patient and their current abdominal surgical condition affects the anticipated intraoperative complexity of emergency abdominal surgeries in Denmark. We found that the prior factors weighing highest were a previous course with open abdomen and previous abdominal surgery described with difficult conditions. The current factors with the highest suspected impact on surgical complexity were being severely hemodynamically unstable and CT with suspected adhesional obstruction. These findings shed light on surgeons’ perceptions and decision-making processes at different experience levels, offering insights into the factors considered crucial for determining surgical management and the need for consultant involvement.
This study revealed a consensus among in-house and on-call surgeons regarding the key factors influencing intraoperative complexity in emergency abdominal surgery. Both groups acknowledged the significance of prior and current characteristics, such as previous abdominal surgery with difficult conditions and diffuse peritonitis during last surgery. Additionally, complex cases involving patients with severe cirrhosis or a history of open abdominal surgeries were identified as particularly potentially challenging. These patients are widely acknowledged for their complexity and associated dismal outcomes [18, 19]. However, a few differences were present in certain areas. For instance, registrars placed greater emphasis on factors such as patients with ventral hernia > 10 cm and previous major ventral hernia surgery (> 10 cm), indicating a potential variation in their risk assessment compared to consultants. Understandably, surgeons with less experience perceive these giant hernias as more challenging, as the conditions are known to be difficult and are recommended to be treated at highly specialized centers with the right skills and volume, even in non-emergency cases [20, 21]. Thus, these variations could stem from differences in experience, training, tradition, or individual perspectives, highlighting the complexity of decision-making in emergency surgical settings and indicating potential benefits of local guidelines outlining when senior surgeons should be present for the procedure.
Several studies have shown outcome variations following cancer resections based on surgeon volume. Higher volume correlates with reduced perioperative mortality, recurrence, and complication rates, alongside improved long-term survival rates [22,23,24]. This is also pertinent to consider in non-cancer surgery, with the principle being that more experienced surgeons are needed in complex surgeries, as surgical performance improves with experience [25]. Our data revealed variations in the factors deemed to necessitate the presence of a consultant from the start of surgery. Consultants were significantly more likely to state that they should be present from the beginning of the surgery due to prior factors such as previous course with open abdomen, diffuse peritonitis during last surgery, previous hernia surgery with IPOM, previous small bowel resection, and previous radiotherapy to the abdomen/pelvis. The latter variable showed a large difference, with 39% of consultants answering that they should be present versus only 3% of the non-consultants. Radiotherapy for pelvic or abdominal malignancies increases intraoperative complexity and worsens outcomes due to radiation-induced damage. The small intestine, particularly fixed portions like the duodenum and terminal ileum, is vulnerable to radiation toxicity, leading to long-term risks such as strictures and fistulas [26]. Similarly, radiation injury to the colon and rectum results in fibrosis and strictures, thus adversely affecting surgical outcomes [26]. Our data suggest that consultants are more aware of the consequences of radiation therapy and the potentially increased intraoperative complexity compared to registrars.
While both groups identified current factors warranting consultant involvement, consultants were more likely to advocate for their presence in cases of severe hemodynamic instability and suspected perforated diverticulitis in CT scans. Hemodynamic instability may be due to different mechanisms, including trauma-related injuries but also non-traumatic conditions such as peritonitis, sepsis, and hemorrhage. These conditions warrant prompt and appropriate treatment, sometimes necessitating a damage control strategy (DCS) [27]. DCS is inherently challenging, and its considerable demands on the surgeon may contribute to the consultant’s preference for being present. Perforated diverticulitis constitutes a critical colonic emergency necessitating emergency surgery due to purulent or feculent peritonitis [28]. In the group of consultants, there were significantly more subspecialists for colorectal surgery, who must be assumed to have an increased sense of responsibility for the actual handling of the condition.
Notably, across all 29 variables (i.e., all prior and current factors), there were no instances where non-consultant surgeons indicated a significantly greater necessity for the presence of a senior surgeon at the beginning of a procedure compared to consultants. This observation is encouraging, considering that summoning experienced colleagues in surgery can be a challenging decision within a field that values autonomy and decisive action [14].
Previous colonic resections are known to cause higher rates of adhesion formation compared to segmental small bowel resection, resection of the rectum, appendectomy, or cholecystectomy [11]. However, in this study, previous elective colonic resection was generally not anticipated to be a preoperative variable leading to an increased risk of intraoperative complexity. The “elective” scenario could influence the respondents in the question. Due to the rates of colorectal malignancy, patients with gastrointestinal emergencies are more likely to have had previous colonic resections compared to other gastrointestinal resections. Thus, these patients comprise a relatively large proportion of emergency abdominal cases and potentially account for one of the most frequent prior factors in the patient population at a surgical emergency department.
The implications of these findings extend beyond individual decision-making to broader considerations in surgical practice and training. Understanding the factors influencing intraoperative complexity and the perceived need for consultant involvement can inform surgical education, resource allocation, and interdisciplinary collaboration in emergency abdominal surgery. Strategies to enhance trainee preparedness for managing complex cases and recognizing situations warranting consultant input could improve patient outcomes and optimize surgical care delivery.
While this study provides valuable insights into surgeons’ expectations regarding intraoperative complexity and the role of consultants in emergency abdominal surgery, certain limitations should be acknowledged. The structure of the residency program in Denmark results in a wildly varying level among non-consultant surgeons, which constitutes a heterogeneous variable that cannot be considered in a questionnaire and could be the explanation for variation and the relatively large standard deviations among surgeons with the same number of years of experience. The study’s reliance on self-reported survey data and the exclusion of malignant conditions may introduce bias and limit the generalizability of the findings. Additionally, variations in surgical practice and training programs across different healthcare systems may influence the applicability of the results beyond Denmark.








留言 (0)