
記住我



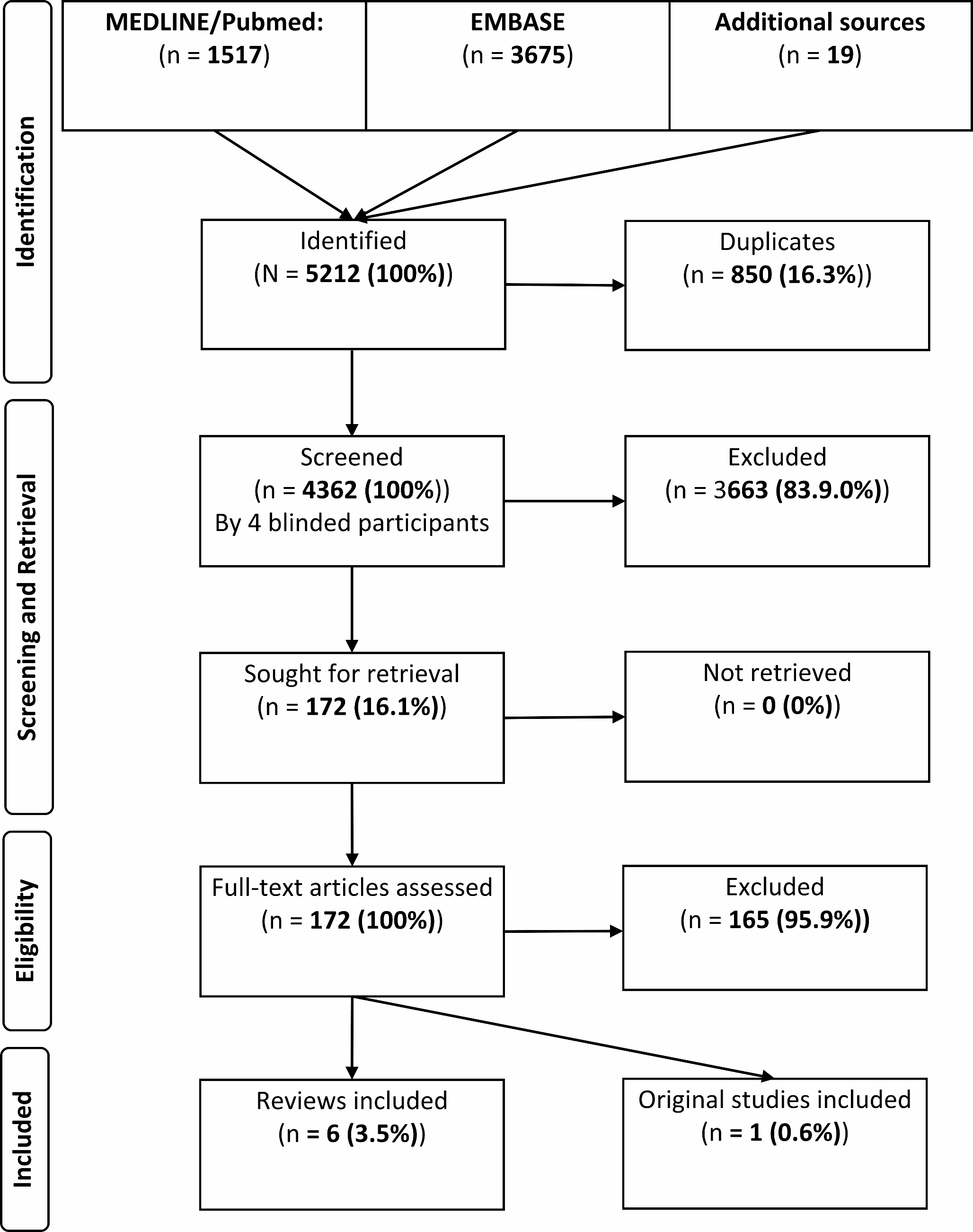
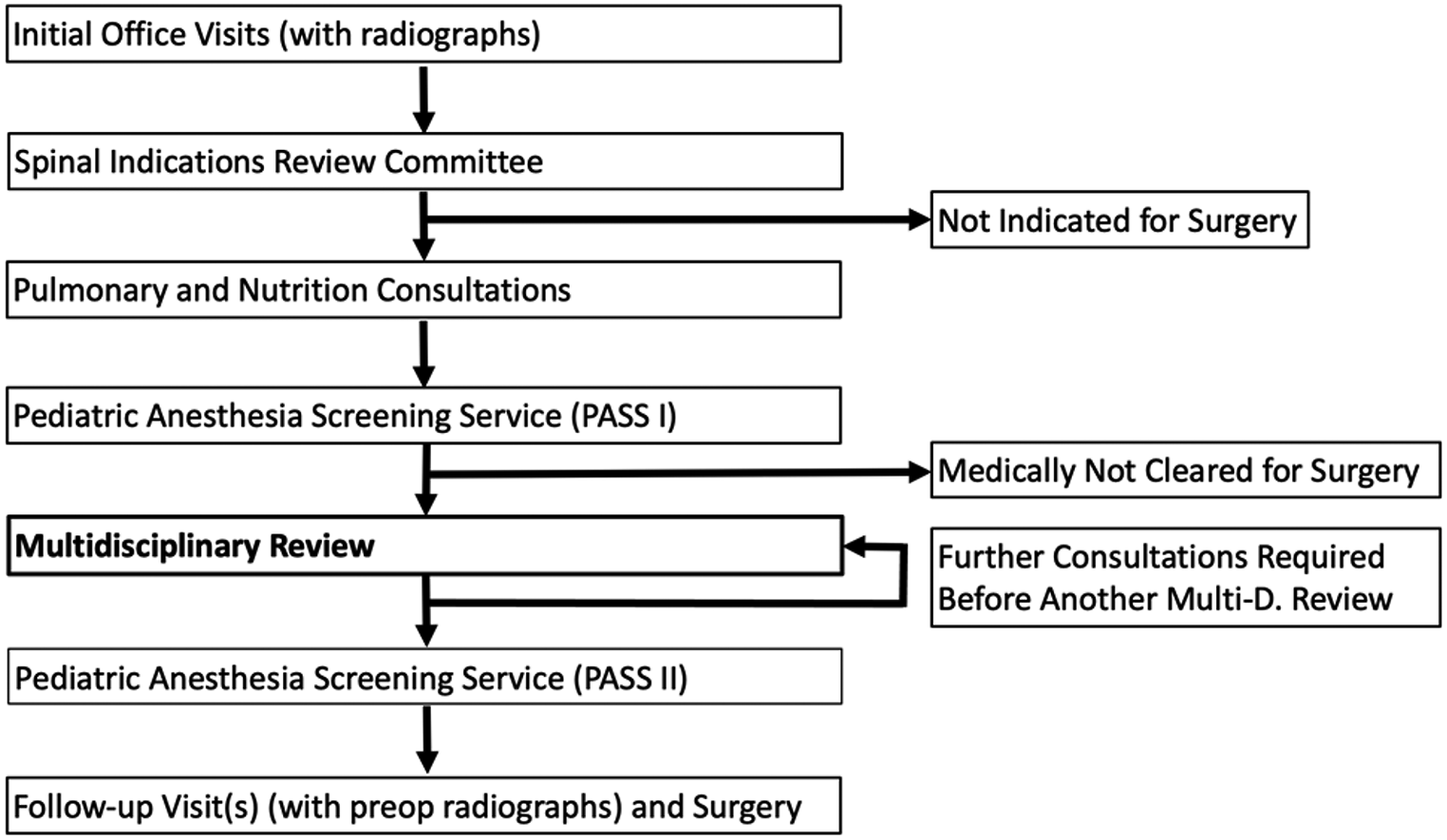

Figure 1 shows the clinical trial profile and patient flowchart. From the original cohort (n = 29 hips in 29 patients), three patients (10.0%) were lost to FU (address unknown / foreign country). Six patients (21.0%) had died from unrelated causes with the implant in situ. In summary, 20 patients (69%) were eligible for analysis. The mean FU of this cohort was 4.5 years (SD 2.2; range 8.4 – 2.1 years). Five patients (17.0%) refused to participate in the study, but all of these patients reported absence of a previous revision surgery. One patient underwent acetabular revision surgery. Complete clinical and radiological follow-up data were available in 14 patients (48.0%) at a mean FU of 4.1 years (SD 2.1; range 2.0 – 8.0 years). Blood samples of these 14 patients were analysed regarding blood concentrations of tantalum. Out of these 14 patients, there were seven male and seven female patients. The mean age of the patients was 72.8 years (range 51–91). The mean BMI was 27.7 kg/m2 (range 21.0–38.9).
Fig. 1
Clinical trial profile and patient flowchart
The indication for the operation was revision THA because of aseptic loosening of the cup in four cases and two-stage revision THA for infection in four cases. The indication for primary total hip arthroplasty was severe osteoarthritis with advanced acetabular bone loss in four cases, aseptic osteonecrosis in 1 case and tumorous destruction (metastatic prostate carcinoma) in one case.
In 11 cases, a tantalum TM augment was used to fill a superior bone void and to restore the anatomical acetabular centre of rotation. In three cases a tantalum TM buttress augment was used.
In 11 cases, a dual-mobility cup was used (see Fig. 2) and in three cases (all primary total hip arthroplasty) a cemented polyethylene cup (see Fig. 3) was used.
Fig. 2
A Preoperative anteroposterior radiograph of the hip of a 56-year-old patient with severe acetabular bone loss including severe posterior acetabular rim defect due to infection and two-stage revision THA. B Anteroposterior radiograph of the same patient 4.5 years after surgery using a modular tantalum TM buttress augment and a cemented dual mobility cup. There are no signs of loosening of one of the components
Fig. 3
A Preoperative anteroposterior radiograph of the hip of a 68-year-old patient with severe osteoarthritis with advanced acetabular bone loss. B Anteroposterior radiograph of the same patient 6 years after surgery using a modular tantalum TM augment and a cemented PE cup. There are no signs of loosening of one of the components
Survival analysisThe cumulative survival rate at 4.5 years with the endpoint “revision of the acetabular component for any reason” was 96.2% (95% Confidence Interval 75.7–99.5). At the most recent FU one patient of the study cohort had undergone revision surgery of the augment and the cup due to a re-infection. The original indication for the operation was two-stage revision of the THA due to a prosthesis infection. In this case, the stable implants had to be completely removed three months after revision surgery due to a persistent infection after an unsuccessful DAIR procedure with replacement of the mobile components five weeks postoperatively.
Patient reported outcome measures and radiographic evaluationMean HHS improved from 36.1 (SD 16.0; 10.0–62.0) points preoperatively to 66.3 (SD 15.5; 42.0–92.0) points at the last FU (p < 0.001). The UCLA Score improved from a mean preoperative score of 1.9 (SD 0.7; 1.0–3.0) points to 3.9 (SD 1.6; 2.0–6.0) points (p < 0.001) (see Fig. 4). Mean postoperative PCS-12 was 32.2 (SD 7.0; 20.7–39.5) points and MCS-12 was 42.6 (SD 9.7; 19.8–38.8) points.
Fig. 4
Comparison of Harris Hip Score and UCLA Score before surgery and at last follow-up, represented in Box- Whisker-Plots. The box marks the interquartile range, the band inside the box indicates the median, whiskers indicating minimum and maximum data
At the last FU, one patient (see Fig. 5) showed signs of initial implant migration with a broken screw and a change of the position of the augment and the cup. We assume secondary osseointegration of the augment with stability of the augment/cup-construct, as no further migration between the first (1 year postoperatively) and the latest FU (3 years postoperatively) has occurred. In addition, the patient confirms absence of symptoms. In the other cases no signs of loosening or implant migration of neither the augment nor the acetabular cup was observed. Two patients developed Brooker grade 1 heterotopic ossification, two patients grade 2, and two patients grade 3 [3].
Fig. 5
A Preoperative anteroposterior radiograph of the hip of a 91-year-old patient with severe osteoarthritis with advanced acetabular bone loss. B Anteroposterior radiograph of the same patient 3 month postoperatively, with a tantalum TM augment in combination with a cemented polyethylene cup. C Anteroposterior radiograph of the same patient 3.1 years postoperatively, with signs of loosening and dislocation of the tantalum augment with broken screw with unchanged cup position
Blood examinationBlood samples from the patients demonstrated a mean tantalum concentration of 0.16 µg/l (SD 0.3, range 0.02 – 0.87 µg/l). Tantalum concentrations of the study group were statistically significantly higher when compared to the control group (mean 0.002 µg/l; SD 0.001, range 0.0002 – 0.002 µg/l) (p < 0.001) [18].
留言 (0)