
記住我



This is an ongoing prospective population-based cohort study conducted in Chongqing Municipality, Southwest China, based on the China Multi-Ethnic Cohort (CMEC) study, which has been described in detail elsewhere [18, 19]. Between September 2018 and February 2019, a total of 23,308 Han Chinese participants aged 30–79 years were recruited to complete an electronic questionnaire with face-to-face interviews (e.g., sociodemographics, diet and lifestyle, medical history), medical examinations (e.g., height, body weight, and blood pressure), and clinical laboratory tests (e.g., blood and urine specimens).
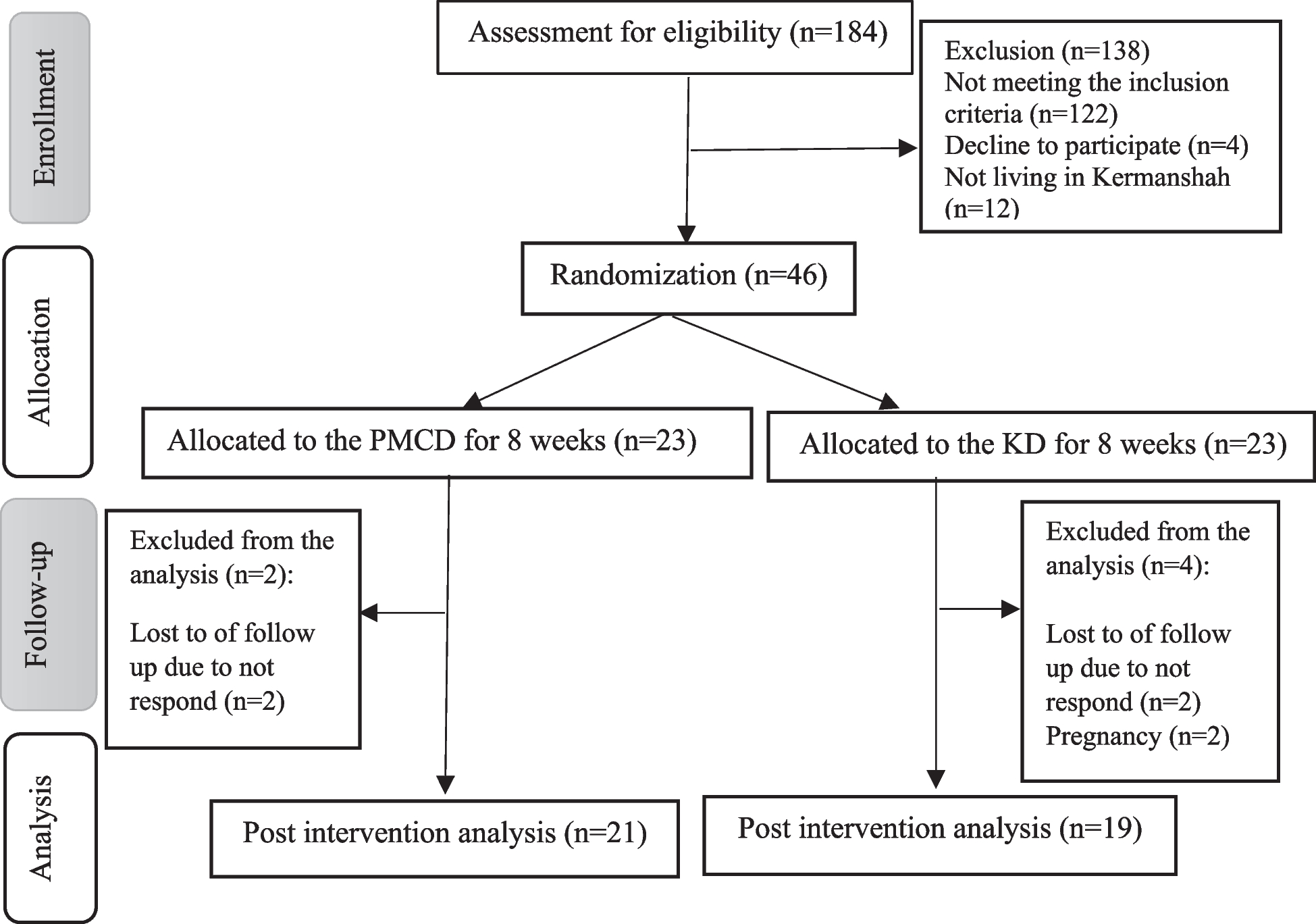
To focus our analysis on individuals at risk of developing diabetes during the follow-up period, we excluded 2,818 participants with a prior diabetes diagnosis before the baseline survey, including those who had been previously diagnosed with diabetes, as well as those with a fasting blood glucose level of ≥ 7 mmol/L, or a glycated hemoglobin percentage of ≥ 6.5% at the time of enrollment. Additionally, a total of 855 individuals with incomplete data on spicy food consumption, diabetes, or other relevant covariates were excluded, along with 3041 participants who reported a history of peptic ulcer, gastroenteritis, or cancer, and 22 subjects who were pregnant or lactating. Finally, 16,572 participants were included (Fig. 1). Ethical approvals from the Medical Ethics Committee of Chongqing Center for Disease Control and Prevention (2021(006),2017(001)) and the Sichuan University Medical Ethical Review Board (K2016038) were obtained. Informed consent was obtained from all study participants.
Fig. 1 Follow-up and outcomes assessment
Follow-up and outcomes assessmentThe follow-up for T2D was conducted by matching with the diabetes case reporting system and death registry system of Chongqing Municipality, with a resurvey among 10% of the surviving participants in 2020, and with annual telephone follow-ups between 2019 and 2022. The definition of T2D onset was based on the ICD-10 (International Statistical Classification of Diseases and Related Health Problems (10th Revision)) code of E11 [20] in the diabetes case reporting system and death system, with the diagnosis date after the baseline survey date; Additionally, self-reported diagnosis of diabetes by a physician in active follow-ups (10% resurvey and annual telephone follow-ups), or a fasting blood glucose level of ≥ 7 mmol/L or a glycated hemoglobin percentage of ≥ 6.5% found on-site during the resurvey. Participants contributed person-months from their enrollment date until the onset of T2D, death (from any cause), loss to follow-up, or the final follow-up assessment date (June 2, 2023, for this current study), whichever came first.
Assessment of spicy food consumptionSpicy food intake refers to the consumption of any “hot” spices when cooking or eating, including fresh or dried chili pepper, chili sauce, chili oil, or other hot spices. Participants were asked about their consumption frequency (never or rarely, only occasionally, 1–2 days/week, 3–5 days/week, or 6–7 days/week) in the past month at baseline. Those individuals who chose the last 3 categories (1–2 days/week, 3–5 days/week, or 6–7 days/week) were categorized as regular spicy food consumers and non-consumers (never or rarely, only occasionally) served as the reference group in this study. Regular spicy food consumers were further asked “What strength of spicy food do you usually eat?”, with three response categories: “weak”, “moderate”, and “strong”. The questions about spicy food consumption mentioned above were based on the China Kadoorie Biobank (a large-scale natural population standard cohort in China). For 3,782 participants who completed the baseline survey in 2018–2019 and the resurvey in 2020 (with an average interval of 21.3 ± 1.2 months), we calculated the Spearman correlation coefficients for the frequency and strength of spicy food consumption, both of which were 0.38.
Assessment of covariatesSociodemographic covariates included gender (male and female), age (continuous), and education level (primary school and below, middle school, high school, college or university and above). A family history of diabetes was defined as having at least one parent or sibling diagnosed with diabetes. Based on the responses to the question “Do you smoke?” participants were categorized as current nonsmokers (no) or current smokers (yes). Alcohol consumption was calculated as grams of pure alcohol per week, based on the self-reported alcohol type, amount drunk, and frequency, assuming the following alcohol content by volume (v/v) in China: beer 4%, grape wine 12%, rice wine 15%, weak spirits 38% and strong spirits 53% [21]. Harmful drinking was defined as > 61 g/day for men and > 41 g/day for women [22]. Physical activity was estimated by summing the corresponding metabolic equivalent values (METs) of four domains, namely, leisure, work, transportation, and housework [23]. Sleep duration was defined as the total time spent sleeping each day, including naptime.
The collection of food intake data was achieved through a quantitative food frequency questionnaire (FFQ). Its validity and reproducibility were both assessed by conducting repeated FFQ and 24-hour dietary recalls in a resurvey in 2020 [24]. Each of the seven food groups, including whole grains, fresh fruits, vegetables, beans, red meat products, dairy, and sodium, was assigned a score of 1 to 5 based on the quintile of the average food intake. For whole grains, fresh fruits, vegetables, beans, and dairy, a score of 5 was given for the highest quintile, while a score of 1 was given for the lowest quintile. For red meat products and sodium, this pattern of scoring was inverted. The sum of the seven component scores resulted in an overall DASH score ranging from 7 (minimal adherence) to 35 (maximal adherence) [24].
Hypertension was defined as systolic/diastolic blood pressure (SBP/DBP) ≥ 140/90 mmHg or a history of hypertension diagnosed by doctors [25]. Dyslipidemia was regarded as having any one of the following conditions: triacylglycerol (TG) ≥ 2.26 mmol/l; serum total cholesterol (TC) ≥ 6.22 mmol/l; low-density lipoprotein cholesterol (LDL-C) ≥ 4.14 mmol/l; high-density lipoprotein cholesterol (HDL-C) < 1.04 mmol/l; or a history of hyperlipemia diagnosed by a physician [26]. If participants had hypertension or dyslipidemia, it was defined as “hypertension or dyslipidemia”.
Statistical analysisContinuous variables were expressed as the median [interquartile range, IQR], and statistical significance was assessed by the Wilcoxon rank sum test. Categorical variables were described as numbers (percentages), and statistical significance was assessed by the chi-square test.
To assess the association between spicy food consumption and the incidence of T2D, we employed Cox proportional hazards regression for multivariable analyses. Additionally, we plotted cumulative survival curves after adjusting for potential confounding factors to visualize the survival probabilities over time. Potential confounding factors were selected based on the literature [22] and the distribution characteristics of the data from this study, and they were progressively adjusted in a series of models. Model 1 was the crude model without any adjustments; Model 2 was adjusted for gender (male and female), age (continuous), education level (primary school and below, middle school, high school, college or university and above), and family history of diabetes (no and yes); Model 3 was adjusted for Model 2 plus smoking status (no and yes), harmful drinking (no and yes), total energy intake (continuous), DASH score (continuous), physical activity (continuous), sleep duration (continuous), BMI (continuous), waist circumference (continuous); Model 4 was adjusted for Model 3 plus hypertension or dyslipidemia (no and yes).
In sensitivity analyses, we utilized a competing risk model to analyze the relationship between spicy food consumption and the incidence of T2D. Additionally, after excluding participants who self-reported a weight loss of at least 2.5 kg in the past year at the baseline survey, we conducted the Cox proportional hazards regressions again to assess the impact of weight loss on the study results.
Data analyses were performed using SPSS (Version 25.0. IBM Corp., Armonk, NY, USA) and R Statistic software (version 4.3.0, R Foundation for Statistical Computing, Vienna, Austria). A two-sided p-value < 0.05 was considered to indicate statistical significance.
留言 (0)