
記住我



This cohort study included data from 47,337 individuals (Fig. 1), including 27,293 (57.7%) women and 20,044 (42.3%) men. Their overall mean (standard deviation) age was 51.9 (8.9) years. During a median follow-up of 15 years, 9,231 deaths were recorded, including 4,215 deaths from CVD, 1,887 deaths from cancer, and 3,373 deaths from other causes. The baseline characteristics of participants, stratified by extreme quintiles of different categories of amino acid consumption, are shown in Table 1.
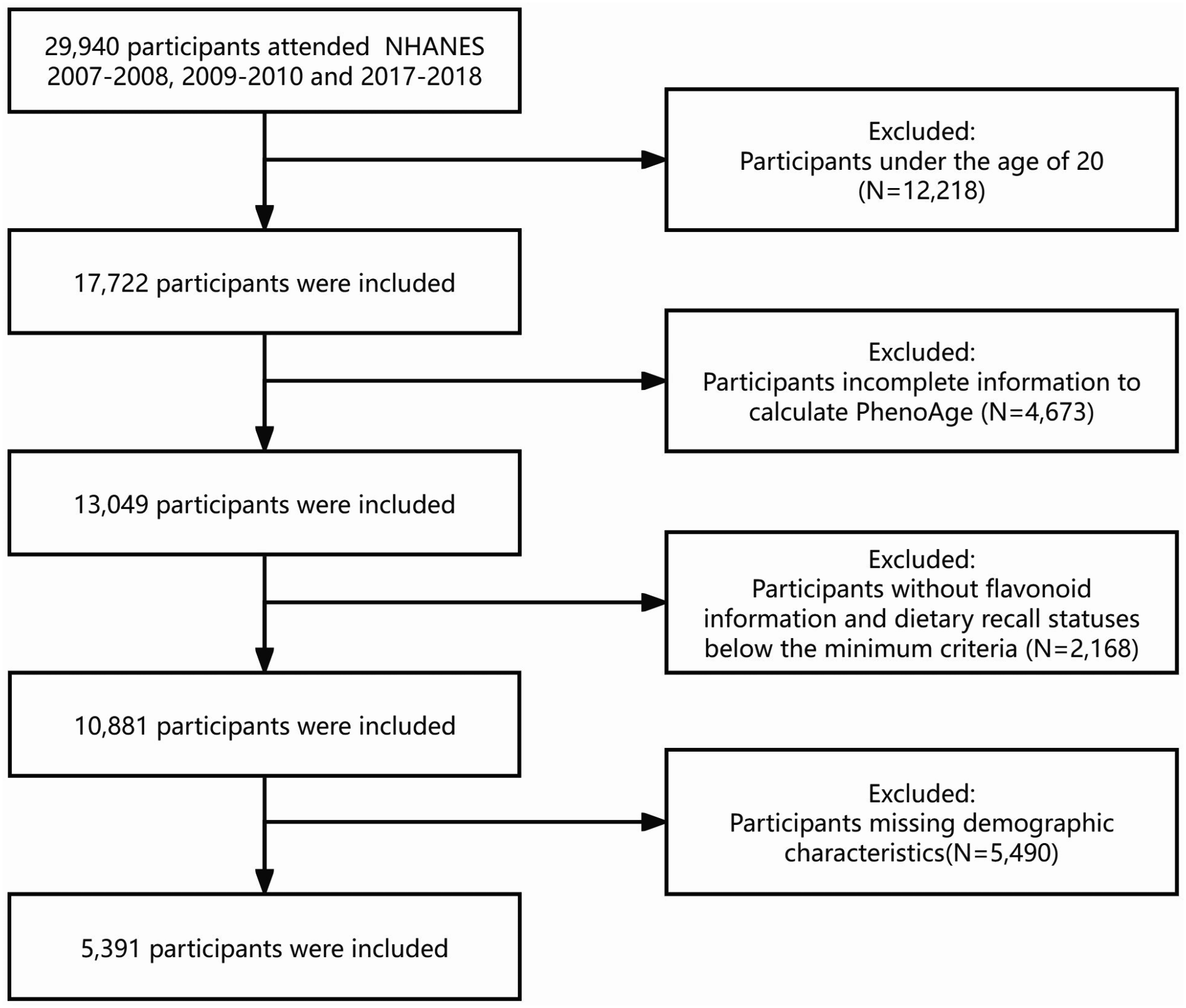
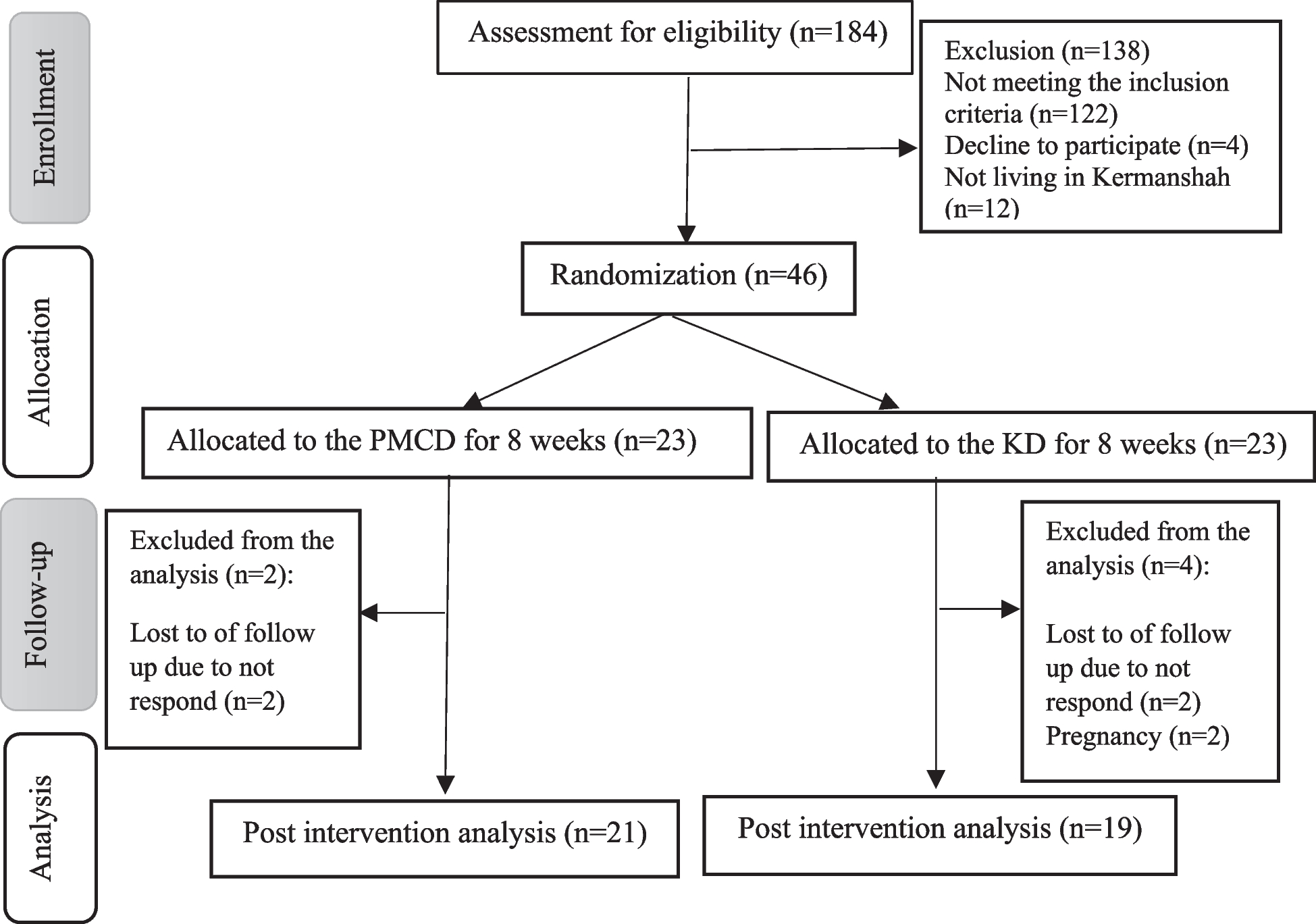
Fig. 1
Flowchart illustrating the selection process of participants
Table 1 Characteristics of the study population, according to the extreme quintiles of amino acid intakeCompared to individuals in the lowest quintile, those in the highest quintile of all categories of amino acids consumption were more likely to be male, have a higher BMI, and more likely to be alcohol drinkers or cigarette smokers. They were more often highly educated, physically active, and had a higher wealth index. Those with higher dietary amino acid consumption were more likely to have diabetes mellitus, have higher energy intake, total lipid and protein intakes, and were less likely to have hypertension.
Essential amino acids and mortalityIn the age-, sex-, and calorie intake-adjusted model (minimally adjusted model), a non-linear association was observed between dietary intake of essential amino acids and hazard of all-cause mortality (P for non-linear trend < 0.001) (Table 2). After fully adjusted model (model 2) was applied, the HRs of all-cause mortality were 1.16 (95%CI, 1.07–1.26) in the first quintile, and 1.08 (95%CI, 1.00-1.16) in the second quintile (P for non-linear trend < 0.001), when compared with the reference group (the third quintile). Figure 2A shows dose-response associations between essential amino acid consumption and all-cause mortality in the fully adjusted model, which is slightly U-shaped.
Fig. 2
Multivariable adjusted cubic spline models for the association between essential amino acids intake and HRs for all-cause mortality (A) and CVD mortality (B); and for the association between non-essential amino acids intake and hazard ratios for all-cause mortality (C), CVD mortality (D), and other cause of mortality (D). Solid lines demonstrate estimates of HRs, while dashed lines demonstrate 95% confidence intervals. Abbreviations: CI, confidence interval; CVD, cardiovascular disease; HR, hazard ratio
Table 2 Multivariate Cox regression derived HRs and 95% CIs for all-cause mortality and cause-specific mortality by essential amino acid intakesParticipants in the first, fourth, and fifth quintiles of essential amino acid intake were at about 11–32% higher risk of CVD mortality, in the minimally adjusted model (P for non-linear trend < 0.001). In the fully adjusted model, compared with the reference group, the HR of CVD mortality was 1.23 (95% CI, 1.09–1.38) in the first quintile (P for non-linear trend = 0.003) (Fig. 2B).
After multivariable adjustment, no significant associations were observed between essential amino acid intake and cancer-related or other causes of mortality.
Non-essential amino acids and mortalityAs shown in Table 3, a non-linear trend was found between non-essential amino acid intake and hazard of all-cause, CVD, and other mortality in minimally and fully adjusted models (P for non-linear trend < 0.05) (Fig. 2C-E). Higher HRs of all-cause (Q5 vs. Q3, 1.20; 95% CI, 1.12–1.30), CVD (Q5 vs. Q3, 1.34; 95% CI, 1.20–1.50), and other mortality (Q5 vs. Q3, 1.27; 95% CI, 1.12–1.45) were found in the upper quintile of non-essential amino acid intake in the minimally adjusted model. These associations were attenuated in the fully adjusted model. Moreover, in the fully adjusted model, participants in the lowest quintile of non-essential amino acid intake (median intake of 29.07 g/day) were at higher risk of all-cause mortality (Q1 vs. Q3, 1.16; 95% CI, 1.06–1.26), CVD mortality (Q1 vs. Q3, 1.14; 95% CI, 1.01–1.29), and other mortality (Q1 vs. Q3, 1.16; 95% CI, 1.01–1.33). No significant association was observed between hazard of cancer-related mortality and non-essential amino acid intake.
Table 3 Multivariate Cox regression derived HRs and 95% CIs for all-cause mortality and cause specific mortality by non-essential amino acids intakeBranched-chain amino acids and mortalityIn the minimally adjusted model, participants in the highest quintile of BCAAs intake were at higher risks of all-cause (HR for Q5 vs. Q3, 1.17; 95%CI, 1.08–1.26), CVD (HR for Q5 vs. Q3, 1.30; 95%CI, 1.17–1.45), and other mortality (HR for Q5 vs. Q3, 1.17; 95%CI, 1.03–1.32). However, when the fully adjusted model was applied, the significance of the associations was lost (Table 4).
Table 4 Multivariate Cox regression derived HRs and 95% CIs for all-cause mortality and cause specific mortality by BCAAs intakeIn the fully adjusted model, the first quintile was associated with all-cause mortality risk (P for non-linear trend < 0.001). Participants with a median BCAAs intake of 7.87 g/day were at about 15% higher risk of all-cause mortality in the fully adjusted model (HR for Q1 vs. Q3, 1.5; 95%CI, 1.06–1.25) (Fig. 3A).
Fig. 3
Multivariable adjusted cubic spline models for the association between BCAAs intake and HRs for all-cause mortality (A) and CVD mortality (B); and for the association between AAAs intake and hazard ratios for all-cause mortality (C) and CVD mortality (D). Solid lines demonstrate estimates of HRs, while dashed lines demonstrate 95% confidence intervals. Abbreviations: AAAs, aromatic amino acids; BCAAs, branched chain amino acids; CI, confidence interval; CVD, cardiovascular disease; HR, hazard ratio
Furthermore, a non-linear association was noted between BCAAs intake and the risk of CVD mortality, as shown in Fig. 3B. BCAAs intakes within the first quintile were associated with about 19% higher risk of CVD mortality in the fully adjusted model (HR for Q1 vs. Q3, 1.19; 95%CI, 1.05–1.34; P for non-linear trend = 0.005).
Aromatic amino acids and mortalityAs shown in Fig. 3C, a non-linear association was observed between dietary aromatic amino acids intake and risk of all-cause mortality (P for non-linear trend < 0.001), with the highest HRs for participants in the first quintile (fully adjusted HR for Q1 vs. Q3, 1.19; 95% CI, 1.09–1.29). A similar trend was found for HRs of mortality from CVD (P for non-linear trend = 0.004) (Fig. 3D). Aromatic amino acids intake within the first quintile (median intake of 4.24 g/day), was significantly associated with increased hazards of CVD mortality (HR for Q1 vs. Q3, 1.21; 95% CI, 1.07–1.36) and cancer mortality (HR for Q1 vs. Q3, 1.28; 95% CI, 1.07–1.54) in the fully adjusted model (Table 5).
Table 5 Multivariate Cox regression derived HRs and 95% CIs for all-cause mortality and cause specific mortality by AAAs intakeSulfur-containing amino acids and mortalitySAAs intake appeared to be associated with all-cause, CVD, cancer, and other mortality in both minimally and fully adjusted models (P for non-linear trend < 0.05), as demonstrated in Fig. 4A-D.
Fig. 4
Multivariable adjusted cubic spline models for the association between SAAs intake and HRs for all-cause mortality (A), CVD mortality (B), cancer mortality (C) and other causes of mortality (D). Solid lines demonstrate estimates of HRs, while dashed lines demonstrate 95% confidence intervals. Abbreviations: CI, confidence interval; CVD, cardiovascular disease; HR, hazard ratio; SAAs, sulfur-containing amino acids
Those who were in the highest quintile of SAAs intake (3.96 g/day) had increased hazards of all-cause, CVD, and other mortality in the minimally adjusted models (P for non-linear trend < 0.001). However, this trend did not remain significant in the fully adjusted model.
Compared with those in the reference group, higher HRs for all-cause (HR for Q1 vs. Q3, 1.18; 95% CI, 1.09–1.28), CVD (HR for Q1 vs. Q3, 1.17; 95% CI, 1.03–1.32), cancer (HR for Q1 vs. Q3, 1.21; 95% CI, 1.01–1.45), and other (HR for Q1 vs. Q3, 1.18; 95% CI, 1.03–1.35) mortality were observed in the fully adjusted model for participants in the first quintile, with a median SAAs intake of 1.75 g/day (Table 6).
Table 6 Multivariate Cox regression derived HRs and 95% CIs for all-cause mortality and cause specific mortality by SAAs intakeEach specific amino acids and mortalityWe further investigated the associations between dietary intake of each amino acid and all-cause and cause-specific mortality. Minimally and fully adjusted HRs are presented in Supplementary Tables 1–18.
In the fully adjusted model, lower intakes of amino acids (first quintile) compared with third quintile were associated with about 12–18% increased hazards of all-cause mortality, for all amino acids except lysine (P for non-linear trend < 0.05 for all comparisons). Furthermore, high intake of proline was associated with significantly increased hazards of all-cause mortality (HR for Q5 vs. Q3, 1.11; 95% CI, 1.01–1.22).
In the fully adjusted model, participants with lower consumption of amino acids (first quintile) had about 13–22% higher hazards of CVD mortality, compared with the reference group (P for non-linear trend < 0.05 for all comparisons). However, such association was not evident for cysteine, glutamic acid, and glycine. Moreover, participants with high intake of glycine had significantly higher hazards of CVD mortality (HR for Q5 vs. Q3, 1.13; 95% CI, 1.00-1.29).
Increased adjusted HRs of cancer-related mortality were found among those who consumed low amount of tryptophan (Q1 vs. Q3, 1.22; 95%CIs, 1.02–1.47), threonine (Q1 vs. Q3, 1.21; 95%CIs, 1.00-1.45), phenylalanine (Q1 vs. Q3, 1.24; 95%CIs, 1.03–1.50), tyrosine (Q1 vs. Q3, 1.21; 95%CIs, 1.01–1.45), valine (Q1 vs. Q3, 1.20; 95%CIs, 1.00-1.44), arginine (Q1 vs. Q3, 1.24; 95%CIs, 1.04–1.48), glycine (Q1 vs. Q3, 1.21; 95%CIs, 1.02–1.44), and serine (Q1 vs. Q3, 1.25 (1.04–1.50).
Adjusted HRs of other causes of mortality were increased among participants within the first quintile of cysteine (Q1 vs. Q3, 1.23; 95%CIs, 1.07–1.42), arginine (Q1 vs. Q3, 1.16, 95%CIs, 1.01–1.32), glycine (Q1 vs. Q3, 1.14; 95%CIs, 1.00-1.30), and proline (Q1 vs. Q3, 1.15; 95%CIs, 1.00-1.32).
Stratified and sensitivity analysesAs a sensitivity analysis, the robustness of data was further examined by excluding individuals who lost to follow-up, died or were diagnosed with cancer within the first two years of the study. In the two-year lag analysis, the risk of all-cause and cause-specific mortality did not differ significantly among the extreme quintiles of amino acids consumption (data not shown).
We conducted stratified analyses to investigate whether the associations between categories of amino acids and mortality were modified by baseline characteristics. Stratification by age, revealed significant interactions between age and intake of essential amino acids (P for interaction = 0.025), BCAAs (P for interaction = 0.010), AAAs (P for interaction = 0.011), and SAAs (P for interaction = 0.038), in relation to hazards of all-cause mortality. Among those younger than 65 years, increased hazards of mortality in higher intakes were observed. However, in older adults (≥ 65 years), lower intakes were associated with increased hazards of mortality (Fig. 5). After stratification by smoking status, there was a significant interaction between smoking status and BCAAs and AAAs intake in relation to the risk of all-cause mortality (P for interaction ˂0.05). In general, the higher risk of all-cause mortality in lower amino acid consumption appeared to be more pronounced in ever-smoker participants in comparison to never-smoker participants. For non-essential amino acids, the associations appeared to be greater among diabetic participants (P for interaction 0.026). In SAAs, in addition to age, significant interaction with sex was also observed for all-cause mortality (P for interaction 0.027). No significant interactions have been found across the stratum for BMI and history of hypertension (Supplementary Figs. 1–5).
Fig. 5
Multivariate Cox regression derived HRs and 95% CIs for all-cause mortality by amino acids intake which were categorized according to age. Multivariable models were adjusted for sex, intake of energy, BMI, cigarette smoking, opium use, diabetes, hypertension, alcohol use, wealth index, education, physical activity, total lipid intake, and total protein intake.*Indicate significant effect (P-value < 0.05). Abbreviations: BCAA, branched-chain amino acids; AAAs, aromatic amino acids; SAAs, sulfur-containing amino acids; AAAs aromatic amino acids; CI, confidence interval; HR, hazard ratio; Q, quintile; Ref, reference
留言 (0)