
記住我







The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and its later amendments. This retrospective study was conducted with the approval of the Research Ethics Committee of the First Affiliated Hospital of Harbin Medical University, the Second Affiliated Hospital of Harbin Medical University, and Heilongjiang Provincial People's Hospital, China (Approval number is SYDWGZR-2020–128). The retrieved data originated from the imaging systems of each hospital for those who had undergone coronary CTA scans for analysis. The follow-up information of the patients was obtained through outpatient visits or telephone follow-ups. Each patient provided written informed consent for undergoing the procedures and for having their data collected and analyzed for research purposes.
Study design and participantsBetween January 2016 and December 2020, we conducted a retrospective study involving 3,392 T2DM patients with symptoms of angina who underwent coronary CTA and were diagnosed with UA, with at least one visible calcification site detected via CTA imaging, which includes both microcalcifications and localized calcifications identified by imaging specialists. Of these, 1,792 patients were recommended to undergo ICA based on a comprehensive assessment by cardiovascular specialists. Ultimately, 1,091 patients and 1,372 vessels underwent ICA, with angiography being accompanied by invasive FFR measurements (Fig. 1). The exclusion included acute coronary syndrome, chronic congestive heart failure, left main coronary artery disease, severe liver and kidney dysfunction, and patients with a life expectancy < 3 years.
Fig. 1
Study flowchart. T2DM, type 2 diabetes mellitus; UA, unstable angina; CCTA, coronary computed tomography angiography; ICA, invasive coronary angiography; CT-FFR, computed tomography-derived computed fractional flow reserve; MACCE, major adverse cardiovascular and cerebrovascular events
Patients were divided into two groups based on their CT-FFR values: those with CT-FFR > 0.80 and those with CT-FFR ≤ 0.80. The CT-FFR values for the three main coronary arteries (left anterior descending artery, left circumflex artery, and right coronary artery) and their branches were measured for each patient. The lowest value obtained was recorded and used as the test value for analysis.
Coronary CTA scanning protocolsEach participating medical center will perform coronary CTA using 256-detector row CT scanners (GE Revolution, General Electric Medical Systems, USA). The scanning procedures will adhere to each center’s established coronary CTA clinical practices. Standard administration of nitroglycerin and beta-blockers will be according to each center’s protocol. After the coronary CTA, an electronic questionnaire will collect baseline details for each patient, including the type of scanning equipment, protocols, iodinated contrast injection details (name, concentration, dosage, and rate), average heart rate during scanning, and the use of nitroglycerin and beta-blockers. The Digital Imaging and Communications in Medicine (DICOM) files will be transmitted to the core laboratory, either online or offline, for preliminary image quality and coronary stenosis evaluation. Following a thorough review, patients meeting the inclusion criteria will be officially enrolled and notified by the core laboratory [16].
Prior to the coronary CTA, a coronary calcium scoring study without contrast enhancement will be conducted. Measurements and calculations were performed using the GE Revolution CT scanner and its SmartScore software. Coronary artery coronary artery calcification score (CACS) analysis was conducted under the AJ130 threshold model, applying the Agatston scoring method to calculate the CACS values [17].
Scan parameters, contrast injection protocols, and reconstruction parametersCalcium Scoring Scan Parameters:
1.Scanner: A 64-slice multidetector CT scanner was used.
2.Tube Voltage: 120 kVp
3.Tube Current: 200 mAs
4.Slice Thickness: 2.5 mm
5.Reconstruction Algorithm: A standard filtered back-projection algorithm was applied to assess the coronary artery calcification.
CT Angiography Scan Parameters:
1.Tube Voltage: 100–120 kVp (adjusted based on patient body mass index)
2.Tube Current: 600–700 mAs
3.Slice Thickness: 0.625 mm
4.Rotation Time: 0.35 s
5.Pitch: 0.2–0.3
6.Reconstruction Algorithm: Images were reconstructed using iterative reconstruction techniques to enhance image quality, particularly in the presence of high-density calcifications.
Contrast Injection Protocol:
1.Contrast Agent: Iodinated contrast medium (350–370 mg I/mL)
2.Injection Rate: 4–5 mL/second, followed by a 30–50 mL saline flush at the same rate.
3.Volume: Total contrast volume was typically between 50–70 mL, depending on patient body weight and scan length.
4.Timing: Bolus tracking was used to optimize the timing of the contrast-enhanced scan. A region of interest (ROI) was placed on the ascending aorta, and scanning commenced when the contrast reached a predefined threshold.
Heart Rate Control:
1.Beta-Blockers: Administered as needed to reduce heart rate below 65 beats per minute prior to the scan.
2.Nitroglycerin: Sublingual nitroglycerin (0.4 mg) was administered 2–3 min prior to scanning to achieve coronary vasodilation.
Reconstruction Parameters:
1.Kernel: A medium-smooth kernel (B46f) was used for calcium scoring, while a sharper kernel (B26f) was applied for coronary CTA.
2.Slice Thickness: 0.6 mm with a 0.4 mm increment for coronary CTA reconstruction to ensure high spatial resolution.
3.Reconstruction Field of View (FOV): Limited to the heart to reduce noise and improve resolution.
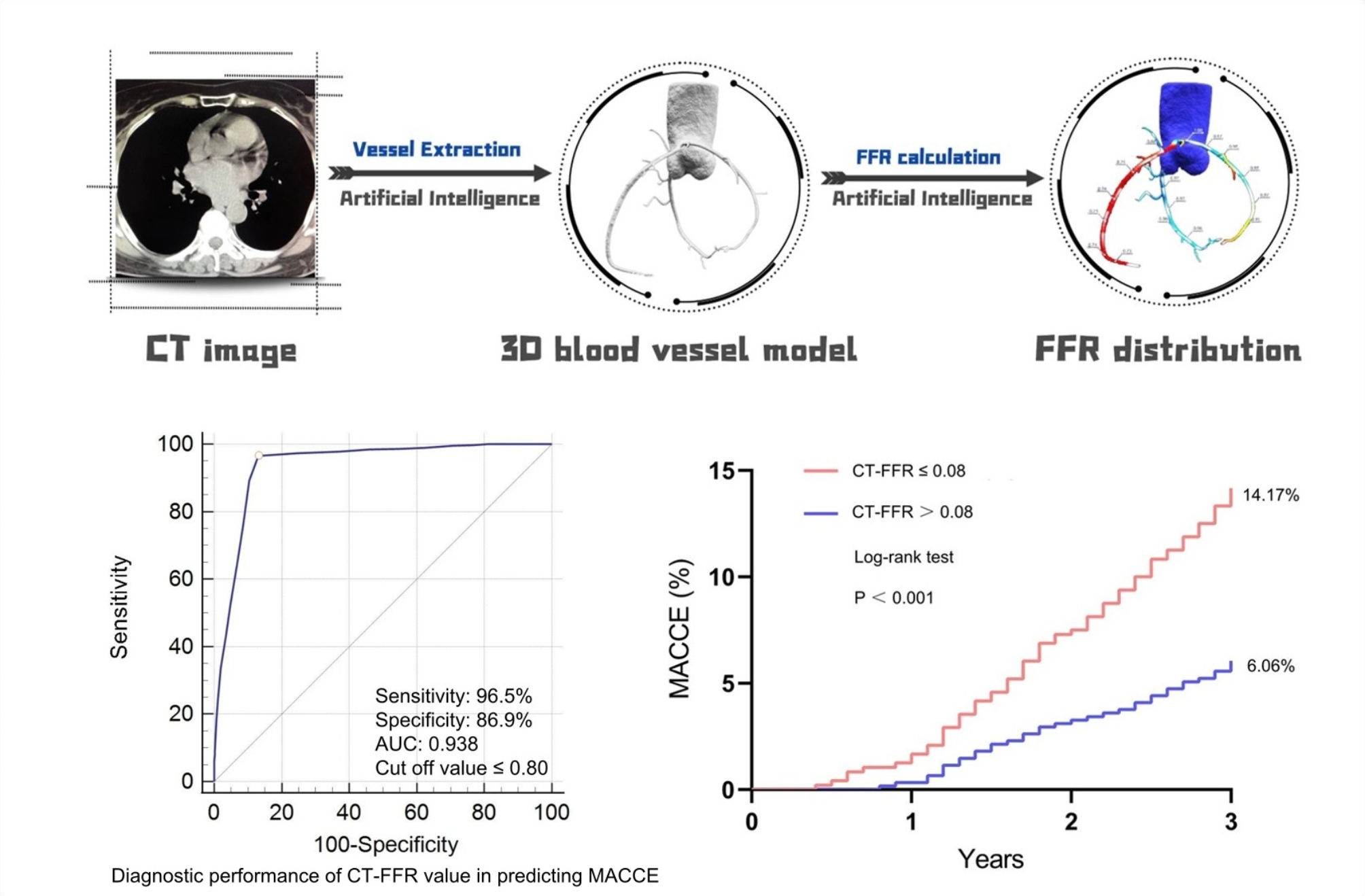
CT-FFR measurementsAll CT-FFR values will be calculated using automated software (DeepVessel-FFR from Keya Medical Technology Co., Ltd.). This software includes two primary components: the coronary artery segmentation model and the computational fluid dynamics (CFD) simulation model (Fig. 2A–C). Specifically, a modified V-Net is initially employed to segment the coronary arteries from the coronary CTA images [18]. First, using established anatomical guidelines and prior vessel segmentation data, we label the vascular branches. A simplified CFD model is then applied to calculate blood flow and pressure, automatically generating CT-FFR values along the coronary arteries. CT-FFR assessments for coronary arteries with diameters of ≥ 1.8 mm will be conducted in the core laboratory by two cardiovascular radiologists. An additional experienced observer will confirm the identification of coronary plaques and the extent of lumen stenosis. CT-FFR measurements will be taken at the proximal and distal points of the stenosis, as well as 20 mm beyond the stenosis to the end of the target vessel (with a minimum diameter of 1.8 mm). A CT-FFR ≤ 0.80 indicates hemodynamically significant coronary stenosis. In this study, lesion-specific CT-FFR values were used for analysis. Specifically, patients with a CT-FFR ≤ 0.80, measured 20 mm distal to the stenosis, were considered to have lesion-specific ischemia. On the other hand, those with a CT-FFR ≤ 0.80 at the end of the target vessel were classified as having distal vessel ischemia. However, for the purpose of analysis, we focused on the lesion-specific CT-FFR values.
Fig. 2
A 72-year-old patient underwent CTA, CT-FFR, and FFR examinations. (A) The axial and curved planar reformatted images of the calcified segment for LAD (the bracket); (B) The cross-sectional and curved planar reformatted images of the calcified segment for LAD (the arrow); (C) The CT-FFR value of the mid-segment of the LAD was 0.74; (D) The FFR value of the mid-segment of the LAD was 0.73. CTA, coronary computed tomography angiography; CT-FFR, computed tomography-derived computed fractional flow reserve; LAD, left anterior descending artery
Invasive coronary angiographyAll ICAs were performed at the following hospitals using a standard protocol [19]: the First Affiliated Hospital of Harbin Medical University, the Second Affiliated Hospital of Harbin Medical University, and Heilongjiang Provincial People's Hospital, all of which are tertiary interventional centers conducting over 5,000 ICAs annually. The procedures were carried out by experienced interventional cardiologists, each performing more than 1,000 ICAs per year, who were not involved in this study. Data on baseline demographics, angiographic characteristics, and laboratory and physical examination outcomes during hospitalization were systematically reviewed from the medical records maintained by each hospital.
Invasive FFRAll major coronary arteries were routinely assessed using FFR, regardless of stenosis severity, except in cases of occluded or subtotal lesions exceeding 90%. Intracoronary adenosine (150 mg) or intravenous adenosine infusion (140 ug/kg/min) was administered to induce maximal coronary hyperemia [20]. FFR was calculated as the ratio of mean distal intracoronary pressure to mean arterial pressure (Fig. 2D). A coronary lesion was deemed hemodynamically significant if the FFR was ≤ 0.80 or if stenosis severity exceeded 90% as determined by quantitative coronary angiography when FFR was unavailable. Lesions with an FFR > 0.80 or a stenosis severity < 30% (as measured by quantitative coronary angiography) in the absence of FFR measurements were considered not functionally significant. All images and FFR signals were interpreted by experienced interventional cardiologists who were blinded to the imaging results [16].
DefinitionUA is defined as acute angina while at rest (within the 48 h before presentation), subacute angina while at rest (within the previous month but not within the 48 h before presentation), or new onset of accelerated (progressively more severe) angina; the clinical circumstances in which unstable angina develops, defined as either angina in the presence or absence of other conditions (e.g., anemia, fever, hypoxia, tach ycardia, or thyrotoxicosis) or angina within two weeks after an acute myocardial infarction; and whether or not electrocardiographic abnormalities are present [21]. DM was diagnosed if a patient was taking insulin or oral hypoglycemic drugs, or if not on these medications, had a casual plasma glucose level > 11.1 mmol/L, a fasting plasma glucose level > 7 mmol/L, or a glycosylated hemoglobin level > 6.0%. Hypertension was diagnosed if the systolic blood pressure was ≥ 140 mmHg and/or diastolic blood pressure was ≥ 90 mmHg, or if the patient had been on antihypertensive medication long-term. Hyperlipidemia was defined as a fasting total serum cholesterol level > 5.17 mmol/L, a low-density lipoprotein cholesterol > 3.15 mmol/L, or a serum triglyceride level > 1.70 mmol/L, or if the patient was on lipid-lowering medication due to a history of hypercholesterolemia. Smoking status was defined as current regular use of cigarettes or having quit smoking within the past year [22]. Repeat revascularization is defined as any subsequent revascularization procedure (such as PCI] or coronary artery bypass grafting [CABG]) performed after the initial revascularization [23]. Major adverse cardiovascular and cerebrovascular events (MACCE) were defined to include all-cause mortality, cardiac death, non-fatal myocardial infarction (MI), stroke, and repeat revascularization.
Statistical analysisQuantitative data are presented as mean ± standard deviation, while qualitative data are shown as frequency (percentage). Comparisons between groups were performed using the independent two-sample t-test. The chi-square test or Fisher’s exact test, as appropriate, was used for categorical variables. The Pearson correlation coefficient was used to determine the correlation between CT-FFR and invasive FFR. A linear regression was used to analyze the correlation between CT-FFR values and CACS. For the regression analysis, we categorized CT-FFR values into two groups: CT-FFR ≤ 0.8 and CT-FFR > 0.8. This binary classification was used in both univariate and multivariate logistic regression analyses to identify predictors of MACCE. The threshold of 0.8 is commonly used to signify hemodynamically significant coronary lesions, allowing for a clear comparison of outcomes between the two groups. A receiver operating characteristic (ROC) curve was generated to determine the optimal cutoffs for indicators with the best diagnostic sensitivity and specificity. The Kaplan–Meier (K-M) method was used to estimate follow-up outcomes, and the log-rank test assessed differences in MACCE distributions. Two-sided P-values < 0.05 were considered statistically significant. All statistical analyses were conducted using SPSS version 22.0 (SPSS Inc., Chicago, IL, USA).
留言 (0)