
記住我

The TRACES trial was conducted prospectively as a randomized, single-blind study. Patients were randomly assigned to standard monitoring or to standard monitoring with additional transcutaneous CO2 monitoring. To ensure comprehensive consideration of all potential influencing factors on the study outcomes, such as the duration of the examination or hemodynamic stress, a stratification according to examination modalities was implemented. The study protocol involved a stratified block randomization into three intervention modality groups requiring deep sedation: cryo-pulmonary vein isolation, 3D mapping-integrated interventions, and ventricular tachycardia ablation. This stratification aimed to evenly distribute any potential influencing factors, such as examination duration or hemodynamic stress observed in ventricular tachycardia ablations, across both study groups. Blocking was applied, and the block size was four. As per the protocol, there were no crossovers in this study. The randomization process occurred before patients entered the investigation room. A technical assistant opened a pre-prepared envelope containing the assigned randomization group and the patient's trial pseudonym, in accordance with the pre-defined investigation modality stratification. Subsequently, the technical assistant placed an electrode for the transcutaneous CO2 monitoring based on the randomization group on the patient's forehead, independent of the group assignment. In the transcutaneous CO2 monitoring group, the monitor and alarms were visible to the treating interventionalist. In contrast, in the standard monitoring group, the interventionalists were blinded to the continuous transcutaneous CO2 monitoring by placing an opaque box over the CO2 monitor and deactivating its alarms. Only the technical assistance team was authorized to operate the transcutaneous CO2 sensor system.
Although both groups had transcutaneous CO2 sensors applied, no data from the transcutaneous CO2 sensor system were included in the analysis of this study, nor were they part of the study endpoints. The transcutaneous CO2 monitoring served as additional monitoring alongside the defined standard monitoring to enhance the interventionalists’ awareness of CO2 elevations. The study's readouts focused on clinical parameters that may be influenced by rising CO2 levels, including pH, venous pCO2 from venous blood gas analysis, peripheral oxygen saturation, non-invasive blood pressure, and the amount of sedation used.
Written informed consent was obtained from all patients prior to randomization, and the protocol received approval from the Ethics Committee of the University of Ulm. The study adheres to the principles of the Declaration of Helsinki. The trial was registered on clinicaltrials.gov on February 15, 2019, under the registration number NCT04038476 and the title 'Transcutaneous Carbon-dioxide Monitoring in Electrophysiological Procedures in Deep Sedation (TRACES)'. The study's reporting adheres to established reporting guidelines, including CONSORT [15].
Trial populationIn this study, all patients scheduled for an electrophysiological examination under deep sedation were eligible for enrollment. Patients were enrolled from August 20, 2019, until October 11, 2023, at the Ulm University Heart Center. The inclusion criteria for the study comprised individuals aged 18 years or older who required an electrophysiological intervention with deep sedation and had provided written informed consent prior to the examination. Exclusion criteria included the absence of written informed consent from the patient or any contraindication (e.g., allergy) to using the forehead sensor of the transcutaneous CO2 monitor.
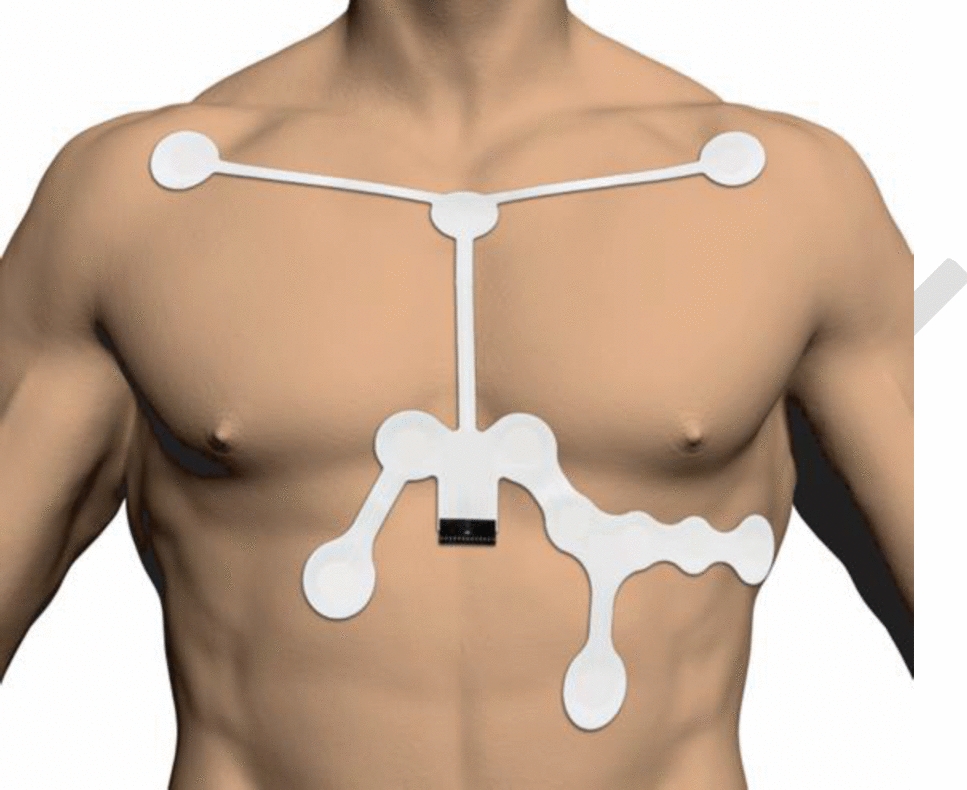
Monitoring setup and sedationA transcutaneous monitoring (TCM) device (TCM400, Radiometer®, Denmark) was utilized for transcutaneous CO2 monitoring. Each patient scheduled for an electrophysiological procedure under deep sedation was randomized following the provision of written informed consent. The electrochemical transcutaneous CO2 sensor was positioned on the forehead of every patient according to the manufacturer's specifications (Fig. 1).
Fig. 1
The illustration of the transcutaneous monitoring setup includes the placement of the electrochemical transcutaneous sensor at the patients’ forehead. TCM, transcutaneous monitoring; PtCO2, carbon dioxide partial pressure measured transcutaneously; SpO2, oxygen saturation measured by pulse oximetry;
Respiratory and hemodynamic standard monitoring included continuous monitoring of heart rate, electrocardiogram, and pulse oximetric oxygen saturation. Non-invasive blood pressure measurements were taken every three minutes, and peripheral venous blood gas analysis was performed every half-hour. The timing and dosage of administered medications, airway management interventions (e.g., Guedel/Wendel airway insertion, oxygen administration), and peripheral venous blood gas analysis results were documented in a sedation protocol by the technical sedation assistance. If patients were randomized to standard monitoring, the transcutaneous CO2 monitoring was concealed, and alarms were deactivated. For patients randomized to additional transcutaneous CO2 monitoring, the examiner had an additional monitor displaying the current transcutaneous CO2 partial pressure as a numerical value and graph. Additionally, the TCM device measures SpO2 and heart rate. An alarm would alert the examiner if transcutaneous CO2 levels exceeded 55 mmHg or the SpO2 levels fell below 90%. Sedative medication was administered in this group once the transcutaneous CO2 graph showed a consistent waveform following self-calibration.
Sedation was performed in a proceduralist-directed, nurse-administered (PDNA) setting. Following preoxygenation via nasal cannula, sedation commenced with a 5 mg bolus of midazolam for anxiolysis, succeeded by continuous propofol infusion through a perfusor pump. The propofol infusion rate was adjusted to achieve deep sedation [5]. Additional opioids (e.g., 50 µg fentanyl bolus for cryo-pulmonary vein isolation or continuous remifentanil infusion for patients undergoing 3D mapping integrated intervention and VT ablation) were administered prior to transseptal puncture and ablation. During deep sedation, airway patency was ensured with a Wendel and/or Guedel airway, and patients received supplemental oxygen via mask. Following the examination and upon the patient's full awakening, the sensor positioned on the forehead was removed.
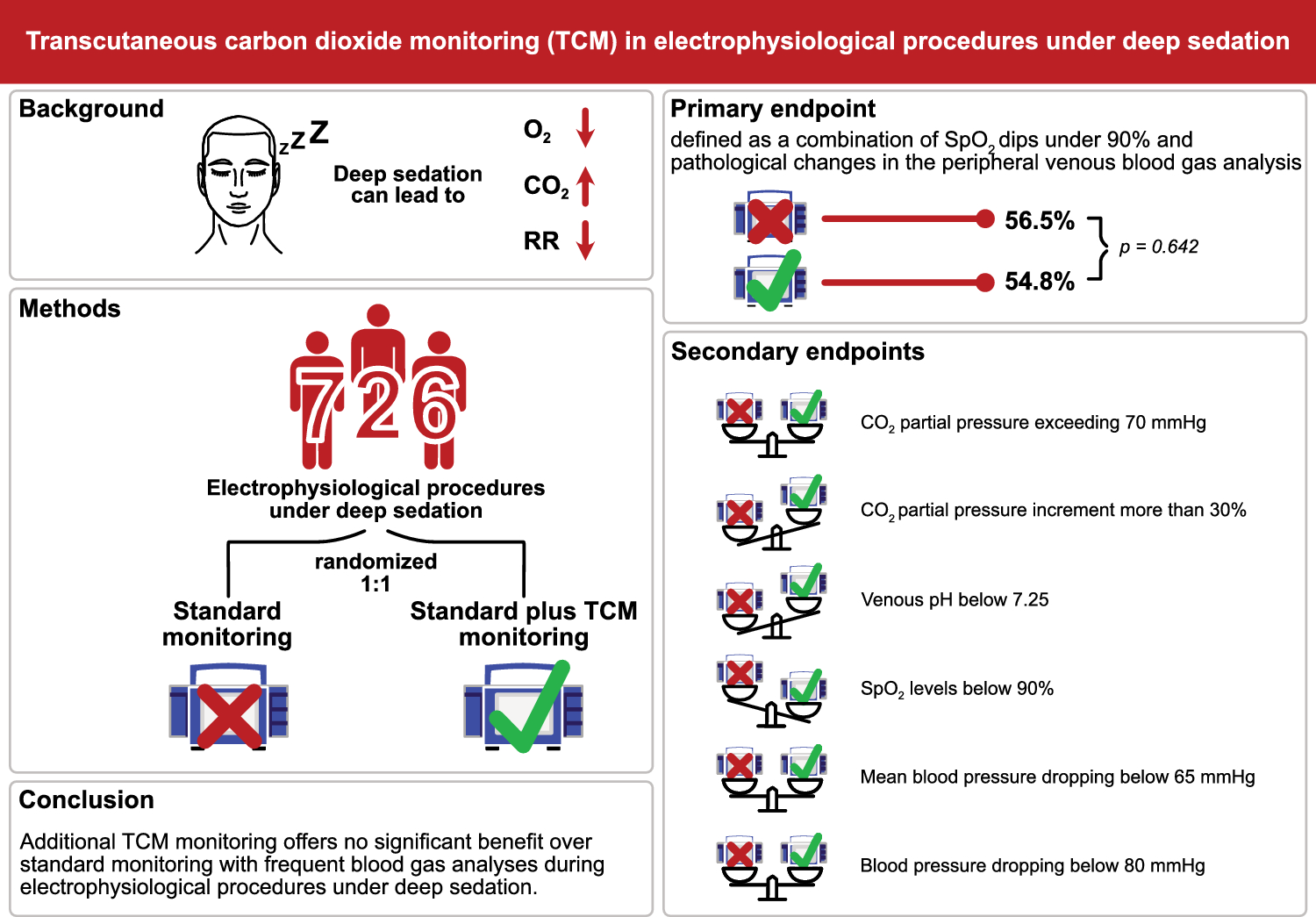
Trial endpointsThe primary composite endpoint was defined as a combination of SpO2 dips under 90% and pathological changes in the peripheral venous blood gas analysis. Pathological alterations were defined as: a CO2 partial pressure (pCO2) increase of more than 30% from baseline, a pCO2 exceeding 70 mmHg, or a pH value under 7.25 indicative of respiratory acidosis. The secondary endpoint comprised the individual components of the combined primary endpoint. Additionally, the secondary endpoint included systolic peripheral blood pressure dropping below 80 mmHg and mean blood pressure dropping below 65 mmHg, which were assessed using non-invasive blood pressure measurements. Therapy with vasopressors was only given after one of the blood pressure endpoints occurred. Variations in the quantity of administered sedatives or opioids, measured in morphine equivalent doses, were also considered.
Statistical analysisInitially, the sample size was estimated to be a total of 246 patients, based on an assumed 18% point reduction in the primary endpoint through transcutaneous CO2 monitoring compared to standard monitoring, derived from clinical routine data. In a sample size analysis using preliminary data, the incidence of the primary endpoint was observed to be 37.6% in the standard monitoring group and 27.4% in the group with additional transcutaneous CO2 monitoring. After correcting for the primary endpoint reduction in the TCM group, the adjusted reduction was 10.2%. The data from this recalculation had not been unblinded to the interventionalists and was solely unblinded for the analysis team. With an alpha error of 0.05 and a desired power of 0.8, the sample size was estimated and finally set at 330 patients for each group: standard monitoring and standard monitoring with additional transcutaneous CO2 monitoring groups, totaling 660 patients. To accommodate potential patient dropouts, such as technical issues with transcutaneous CO2 monitoring or redirection of the patient to an electrophysiology lab without transcutaneous CO2 monitoring capability, an additional 10% of patients were included in the calculation. Thus, the final required sample size for the study was 726 patients.
The statistical analysis utilized SPSS Statistics (V29, IBM, Armonk, NY, USA). A significance level of p < 0.05 was applied. Categorical variables were summarized as frequencies and analyzed using the Chi-square test or Fisher’s exact test, as appropriate. Numeric variables were assessed for normal distribution via the Shapiro–Wilk test and equal variance with Levene’s test. Normally distributed variables were presented as mean ± standard deviation and analyzed using Student’s t-test. Non-normally distributed variables were presented as median ± interquartile range (IQR) and analyzed using the Mann–Whitney rank sum test.
留言 (0)