
記住我
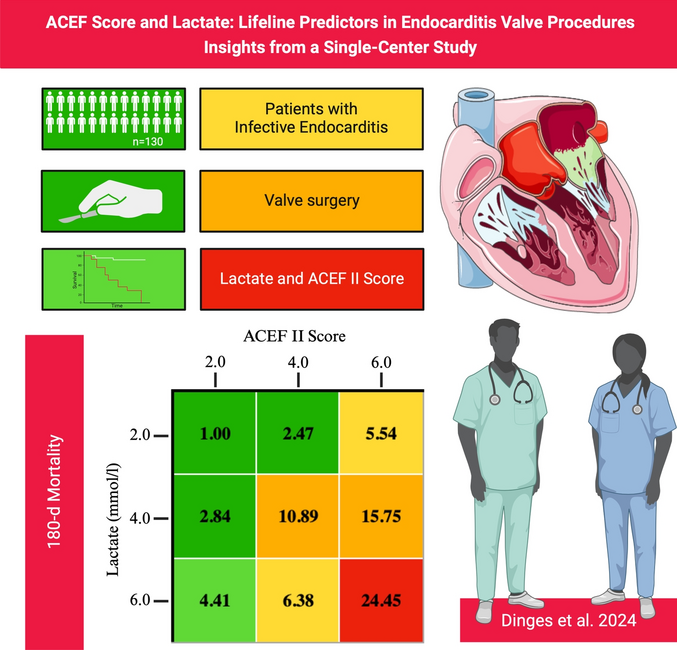

Table 1 provides an overview of the baseline characteristics of all participants, highlighting differences between those who survived one year post-surgery and those who did not. The study included 130 patients. 28 patients (21.5%) died within one year after surgery for infectious endocarditis. The average age of the cohort was 61.9 ± 14.4 years, with males comprising 70.8% of the group. Staphylococci were the most commonly identified pathogens (36.9%), followed by Streptococci (22.3%). Pathogen evidence was insufficient in 21 patients (16.2%). Patients who did not survive after one year had the tendency to prolonged total surgery time, clamp time, and perfusion time, as well as extended ventilation duration and ICU stay. Furthermore, non-survivors exhibited higher preoperative ACEF II Scores (3.9 ± 1.8 vs. 2.9 ± 1.4; p = 0.007) and significantly elevated postoperative 24-h levels of lactate (4.5 ± 4.7 mmol/l vs. 2.7 ± 3.2 mmol/l; p = 0.001), Troponin-T (998.5 ± 2934.3 ng/l vs. 769.0 ± 991.0; p = 0.031), and CK-MB (96.1 ± 67.1 U/l vs. 54.2 ± 22.4 U/l).
Table 1 Baseline characteristics of overall study cohort and presence or absence of 1-year mortalityAUROC—short-term survivalLactate, troponin-T, CK-MBFigure 1 illustrates the AUROC curves for predicting mortality at various short-term survival points using lactate, Troponin-T, and CK-MB levels. In Panel A, the AUROC curves for 30-day mortality reveal that maximum lactate levels 24 h postoperatively have the highest area under the curve (AUC = 0.822). Panel B shows the curves for 90-day mortality, with lactate again demonstrating a relatively high AUC of 0.710. Panel C displays the curves for 180-day mortality, where lactate maintains its strong predictive capability with an AUC of 0.759. Each panel also includes tables that summarize the AUC, 95% confidence intervals, p-values, cut-off values, sensitivity, specificity, and YI for each biomarker.
Fig. 1
AUROC analysis (Lactate, Troponin-T, CK-MB) with corresponding cut-off values, sensitivity, specificity and Youden index for short-term mortality (Panel A: 30d mortality; Panel B: 90d mortality; Panel C: 180d mortality)
ACEF II Score and EuroSCORE IIFigure 2 displays the AUROC curves for predicting short-term mortality at various time points using the ACEF II Score and EuroSCORE II. The first panel reveals that for 30-day mortality, the ACEF II Score demonstrates a higher predictive capability with an AUC of 0.776 compared to the EuroSCORE II, which has an AUC of 0.696. Moving to 90-day mortality, the second panel shows that the ACEF II Score continues to outperform the EuroSCORE II, achieving an AUC of 0.721 against 0.667. The third panel illustrates the AUROC curves for 180-day mortality, where the ACEF II Score once again proves to be more accurate, with an AUC of 0.729 compared to the EuroSCORE II’s AUC of 0.644.
Fig. 2
AUROC analysis (EuroSCORE II, ACEF II Score) with corresponding cut-off values, sensitivity, specificity and youden index for short-term mortality (Panel A: 30d mortality; Panel B: 90d mortality; Panel C: 180d mortality)
AUROC—long-term survivalLactate, troponin-T, CK-MBFigure 3 shows the AUROC curves evaluating the predictive performance of postoperative lactate, troponin, and CK-MB levels for 1, 2, and 3-year mortality. For 1-year mortality (Panel A), lactate had an AUC of 0.759, cut-off of 3.40 mmol/L, sensitivity of 0.67, and specificity of 0.76. Troponin's AUC was 0.621, cut-off 0.91 ng/mL, sensitivity 0.53, and specificity 0.64. CK-MB's AUC was 0.654, cut-off 65.80 U/L, sensitivity 0.57, and specificity 0.69. For 2-year mortality (Panel B), lactate's AUC was 0.743, troponin's was 0.607, and CK-MB's was 0.663. For 3-year mortality (Panel C), lactate's AUC was 0.733, troponin's was 0.592, and CK-MB's was 0.649. The cut-off values and sensitivity/specificity were similar to those for 1-year mortality.
Fig. 3
AUROC analysis (Lactate, Troponin-T, CK-MB) with corresponding cut-off values, sensitivity, specificity and youden index for long-term mortality (Panel A: 1-year mortality; Panel B: 2-year mortality; Panel C: 3-year mortality)
ACEF II score and EuroSCORE IIFigure 4 presents ROC curves for the ACEF II Score and EuroSCORE II predicting 1, 2, and 3-year mortality. For 1-year mortality (Panel A), ACEF II had an AUC of 0.729, cut-off of 3.15, sensitivity of 0.68, and specificity of 0.71. EuroSCORE II had an AUC of 0.644, cut-off 5.53, sensitivity 0.79, and specificity 0.54. For 2-year mortality (Panel B), ACEF II's AUC was 0.665, and EuroSCORE II's was 0.669. For 3-year mortality (Panel C), ACEF II's AUC was 0.673, and EuroSCORE II's was 0.597. The cut-off values and sensitivity/specificity were similar across these time frames.
Fig. 4
AUROC analysis (EuroSCORE II, ACEF II Score) with corresponding cut-off values, sensitivity, specificity and youden index for long-term mortality (Panel A: 1-year mortality; Panel B: 2-year mortality; Panel C: 3-year mortality)
Kaplan–Meier curves—survival analysis according to lactate and ACEF II score cut-off values according to AUROC analysesLactateIn Fig. 5, the Kaplan–Meier survival curves show postoperative survival probabilities based on maximum lactate levels below 3.40 mmol/L versus those with levels equal to or greater than 3.40 mmol/L. Panel A focuses on short-term survival at 30, 90, and 180 days. Significant differences in survival are indicated with p-values of 0.008 for 30-day, < 0.001 for 90-day, and < 0.001 for 180-day survival, as shown by the log-rank test. Panel B extends the analysis to three years, comparing the same lactate level groups. Significant differences in long-term survival are shown with p-values < 0.001 for 1-year, 2-year, and 3-year survival, as demonstrated by the log-rank test.
Fig. 5
Kaplan–Meier curves with corresponding numbers at risk and log-rank tests for detection of short- and long-term mortality regarding a lactate cut-off value of 3.40 mmol/l (Panel A: 30d to 180d mortality; Panel B: 1- to 3-year mortality)
ACEF II scoreFigure 6 shows a comparison of postoperative survival between patients with ACEF II Scores below 3.15 and those with scores of 3.15 or higher. Panel A depicts short-term survival at 30, 90, and 180 days, highlighting significant differences with p-values of 0.003, < 0.001, and < 0.001, respectively. Panel B extends this comparison to a three-year period, illustrating the survival differences between the same groups. The log-rank test indicates highly significant differences in long-term survival, with p-values of < 0.001 for 1-year, 2-year, and 3-year survival.
Fig. 6
Kaplan–Meier curves with corresponding numbers at risk and log-rank tests for detection of short- and long-term mortality regarding a ACEF II Score cut-off value of 3.15 (Panel A: 30d to 180d mortality; Panel B: 1- to 3-year mortality)
Kaplan–Meier curves—survival analysis according to lactate and ACEF II score intervalsLactateFigure 7 presents the Kaplan–Meier survival curves illustrating postoperative survival probabilities based on maximum lactate levels 24 h postoperatively. In Panel A, short-term survival is analyzed at 30, 90, and 180 days, with patients stratified into four lactate categories: 0–2 mmol/L, 2–4 mmol/L, 4–6 mmol/L, and > 6 mmol/L. The log-rank test reveals statistically significant differences in survival across these groups, with p-values of 0.014 for 30-day survival, 0.007 for 90-day survival, and 0.002 for 180-day survival. Panel B extends this survival analysis up to three years, maintaining the same lactate level stratifications. Significant differences in long-term survival are evident, as indicated by p-values of 0.002 for 1-year survival, 0.001 for 2-year survival, and 0.002 for 3-year survival, according to the log-rank test.
Fig. 7
Kaplan–Meier curves with corresponding numbers at risk and log-rank tests for detection of short- and long-term mortality regarding different lactate intervals (Panel A: 30d to 180d mortality; Panel B: 1- to 3-year mortality)
ACEF II scoreIn Fig. 8, the Kaplan–Meier survival curves depict postoperative survival probabilities based on the ACEF II Score. Panel A focuses on short-term survival at 30, 90, and 180 days, with patients categorized into four ACEF II Score groups: 0–2, 2–4, 4–6, and > 6. Highly significant differences in survival are observed across these groups, with p-values < 0.001 for 30-day, 90-day, and 180-day survival, as shown by the log-rank test. Panel B of presents extended survival analysis up to three years for the same ACEF II Score categories. The log-rank test again indicates significant survival differences, with p-values < 0.001 for 1-year, 2-year, and 3-year survival.
Fig. 8
Kaplan–Meier curves with corresponding numbers at risk and log-rank tests for detection of short- and long-term mortality regarding different ACEF II Score intervals (Panel A: 30d to 180d mortality; Panel B: 1- to 3-year mortality)
Correlation analysisThe correlation analysis of Table 2 identified several significant associations between clinical variables and postoperative biomarkers (lactate, Troponin, CK-MB). Significant positive correlations with maximum lactate levels 24 h postoperatively were found for weight, BMI, ACEF II Score, surgery time, clamping time, perfusion time, ventilation period, ICU stay, intraoperative fluid volume, diabetes mellitus, atrial fibrillation, use of diuretics, endocarditis of two heart valves, sepsis and further clinical characteristics. Additionally, negative correlations were observed between maximum lactate and minimal intraoperative hemoglobin (Hb) and renal excretion 1–2 h and 2–3 h postoperatively. Maximum Troponin-T levels 24 h postoperatively were significantly correlated with surgery time, clamping time, perfusion time, minimum intraoperative hemoglobin, minimum postoperative hemoglobin, COPD and renal excretion 1–2 h and 2–3 h postoperatively. Significant correlations for maximum CK-MB levels 24 h postoperatively included surgery time, clamping time, perfusion time, maximum lactate levels, maximum lactate and Troponin-T levels 24 h postoperatively, and complicated pneumonia.
Table 2 Correlation analysis (Lactate, Troponin-T, CK-MBHeatmaps of short-term mortality rates by lactate and ACEF II scoresFigure 9 is crucial as it visually represents the interaction between lactate levels and ACEF II Scores in predicting short-term postoperative hazard ratios regarding short-term mortality. The heatmaps detail hazard ratios at 30, 90, and 180 days, highlighting the correlation between elevated lactate levels, higher ACEF II Scores, and increased hazard. For instance, at 30 days, patients with lactate levels greater than 6 mmol/l and an ACEF II Score above 6 had the highest hazard ratio of 20.05. This pattern continues at 90 days, where the highest hazard ratio observed is 20.11 for patients with both high lactate levels and ACEF II Scores. At 180 days, the trend persists, with the maximum hazard ratio reaching 24.45 for those with lactate levels above 6 mmol/l and an ACEF II Score greater than 6.
Fig. 9
Heatmaps with hazard ratios of 30d, 90d and 180d mortality highlighting the correlation between lactate and ACEF II Score
留言 (0)