
記住我




A 75-year-old male patient with a history of diabetes, hypertension, and stable coronary artery disease is presented. In June 2015, he developed bacterial infective endocarditis due Streptococcus gallolyticus complicated by aortic valve insufficiency, necessitating conventional valve replacement (23 mm Carpentier). In May 2021, he experienced prosthetic dysfunction and Underwent percutaneous aortic valve-in-valve replacement using a 26 mm CoreValve Evolut R prosthesis. In October 2021, he underwent colectomy due to pT1 pN0 M0 colon cancer. On the first postoperative day, he developed fever without a defined source, which persisted despite treatment with multiple antibiotics during a 40 days hospitalization. Subsequently, he was referred to our center for further investigation.
Upon admission, the patient’s vital signs were stable, but he appeared pale and febrile (axillary temperature of 38 °C). Physical examination revealed no abnormalities in the respiratory, cardiovascular, abdominal, or extremities systems, except for a well-healing surgical wound. Chest X-ray and electrocardiogram showed no abnormalities. Initial laboratory tests revealed only an elevated C-reactive protein level. Repeat blood and urine cultures were negative, consistent with previous results. Additional imaging studies, including computed tomography scans of the chest and abdomen, did not reveal any significant findings. A transesophageal echocardiogram showed normal functioning of the prosthetic valve with minimal periprosthetic thickening, without evidence of vegetations or abscess.
Considering the persistent fever and the absence of a clear focus of infection despite broad-spectrum antibiotics, a positron emission tomography-computed tomography (PET-CT) scan was performed. The PET-CT scan showed increased uptake around the aortic prosthesis, indicating an active infectious process (Fig. 1). Furthermore, a repeat transesophageal echocardiogram revealed an organizing periprosthetic abscess (Fig. 2).
Fig. 1
- Fig. 1 - PET-CT: Increased metabolic activity observed in the prosthesis. A - Axial sequence of slices. B - Coronal slice
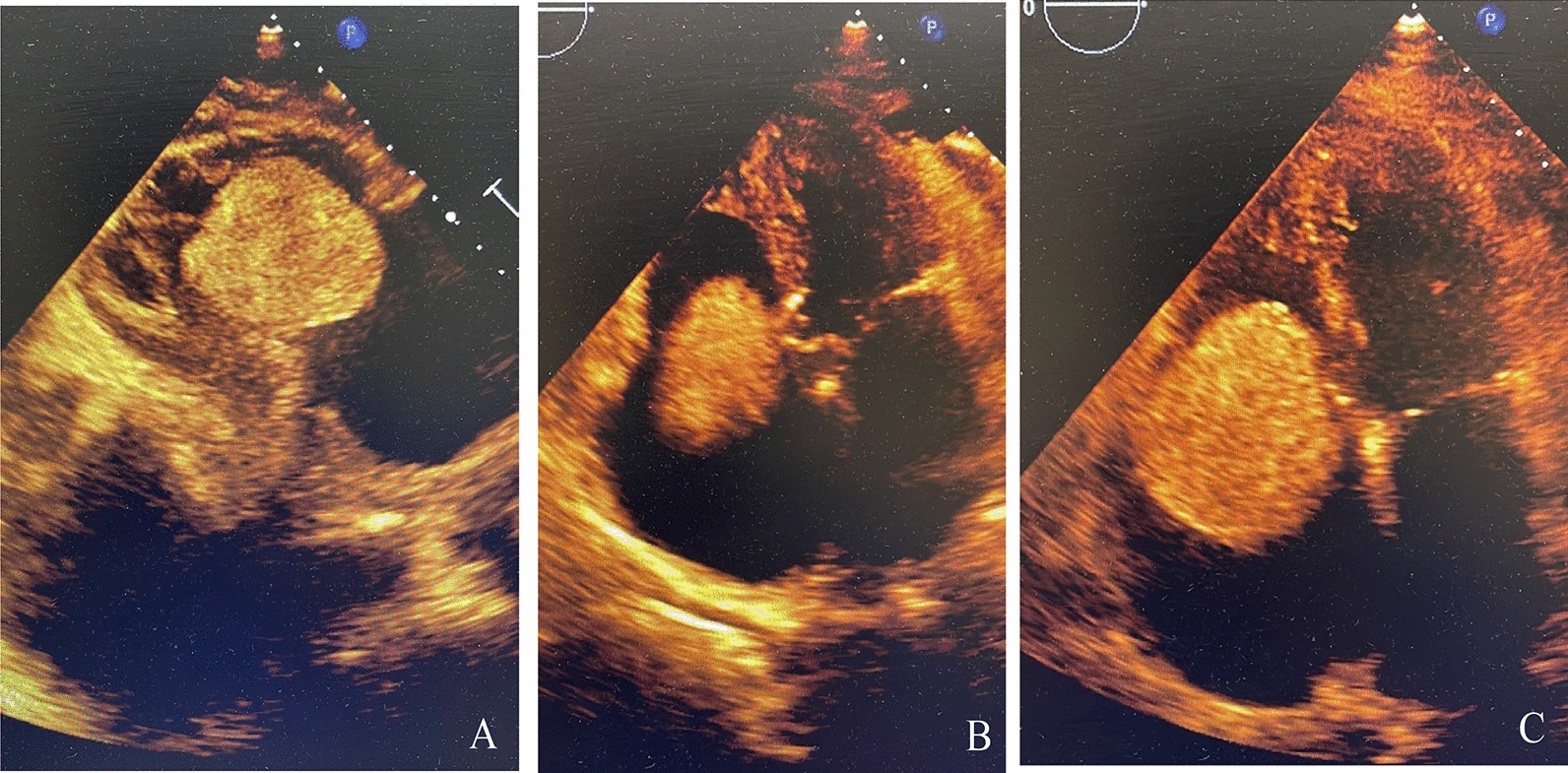
Fig. 2
3D Transesophageal echocardiogram demonstrating a normally functioning bioprosthetic valve in the aortic position, but with evidence of periprosthetic thickening and abscess formation
Given these findings and the refractory nature of the condition despite multiple broad-spectrum antimicrobial therapy, antifungal coverage was added with liposomal amphotericin B. At that moment, after a multidisciplinary discussion, it was decided to extend clinical treatment with antifungal therapy, as the patient was considered to be at very high risk. Furthermore, the surgical team deemed the procedure highly complex due to the need for explantation of two valves combined with the likely resection of the ascending aorta. The patient’s condition showed no improvement. After a few weeks treatment at our center, in 12/31/2021, serial contrast-enhanced chest tomography scans revealed an enlargement of the valve abscess, as well as progression of periaortic hematoma and pseudoaneurysm of the ascending aorta, with the neck located close to the distal end of the aortic prosthesis (Fig. 3). Due to the high mortality associated with the identified condition, urgent surgery was chosen for pseudoaneurysm repair.
Fig. 3
Pseudoaneurysm of the ascending aorta with a neck measuring 0.7 cm contained by a periaortic hematoma (diameter 8 cm). One of the valve prosthesis struts is in contact with the aortic wall, leading to the formation of the communication related to the neck of the pseudoaneurysm. A - Sagital Slice. B - Coronal section showing an 8 cm hematoma. C - Coronal section showing pseudoaneurysm of the ascending aorta with a neck measuring 0.7 cm
Initially, the patient was placed on cardiopulmonary bypass via femoral vein and artery cannulation with hypothermia at 28ºC. The aorta was clamped and exposed (Fig. 4.A), followed by dissection of the pseudoaneurysm until the laceration in the ascending aorta was visualized (Fig. 4.B). After a longitudinal dissection of the aorta, the TAVI strut was observed at the site of the laceration (Fig. 4.C), extending through all layers of the vessel wall and protruding into the pseudoaneurysm. The bioprosthesis, along with the aortic wall incorporated into the device mesh, was explanted with no macroscopic signs of endocarditis (Fig. 4.D; 4.E). At this point, cold cardioplegia with Custodiol® was administered in the coronary ostia. A decision was made to proceed with an aortic valve replacement using a 23 mm Edwards Inspiris bovine bioprosthesis, secured with mersilene® 2 − 0 mattress sutures in the annulus. Subsequently, the ascending aorta was replaced with a No. 28 Dacron tube, extending from the supracoronary plane to below the brachiocephalic trunk. The total cross-clamp time was 225 min, with 208 min of ischemia. Intraoperative echocardiography demonstrated normal functioning of the new prosthesis.
Fig. 4
A - Intraoperative exposure of the pseudoaneurysm. B - Identification of the laceration site (Arrow) measuring approximately 0.5 cm x 0.5 cm. C - Exposure of the TAVI frame in contact with the pseudoaneurysm, with one of the struts perforating the layers of the aorta. D and E - Surgical specimen, with no macroscopic evidence of endocarditis
In the immediate postoperative period, the patient experienced mediastinal and pleural bleeding, which required re-operation to achieve hemostasis of the chest wall vessels. Following this intervention, the patient had a good clinical course. Microbiological analysis of surgical specimens (pseudoaneurysm and explanted prosthesis) identified multisensitive Candida albicans. The patient continued to show improvement and was discharged on a prolonged regimen oral fluconazole. The patient remains under clinical follow-up, with the most recent transthoracic echocardiogram from January 2024 showing a normally functioning aortic prosthesis, a maximum systolic gradient of 16 mmHg, and no evidence of endocarditis.
留言 (0)