In a contemporary cohort of preterm infants with grade 2 or 3 BPD, we did not find a significant difference in serum sodium, potassium, or chloride changes following administration of furosemide compared to chlorothiazide. These findings suggest that chlorothiazide may not be a “gentler” diuretic than furosemide when characterized based on serum sodium, potassium, and chloride loss in preterm infants with high grade BPD.
Our previous findings also call into question whether chlorothiazide has less pronounced effects on serum electrolytes. In a cohort of 3252 very preterm infants developing high-grade BPD at United States children’s hospitals, we showed that chronic thiazide use was associated with greater sodium chloride and potassium chloride supplementation compared to chronic loop diuretic exposure [21]. Our findings are inconsistent with a previous study by Dartois et al., who reported a lower risk of electrolyte derangement with thiazide diuretics compared to furosemide (37% vs. 87%, p < 0.001) exposure in infants born between 36 and 41 weeks’ gestational age. However, this study evaluated a broad neonatal population that included preterm and term infants, and no significant difference in electrolyte derangements were noted among the preterm infant population born < 32 weeks’ gestation [17]. The differing findings between our studies may reflect heterogenous treatment effects in distinct neonatal populations.
We identified several clinical and diuretic characteristics that were associated with greater changes in serum electrolytes following furosemide or chlorothiazide administration. A higher diuretic dose and exposure to a higher number of diuretic administrations were associated with greater serum sodium and chloride loss. Our findings of greater electrolyte change following exposure to a higher diuretic dose and higher number of diuretic administrations are consistent with findings from two recent studies. Sridharan et al. found that a cumulative dose of 4 mg/kg/day of furosemide increased the risk of electrolyte abnormality among preterm infants in a single-center study [25]. Similarly, Dartois et al. found that a total daily dose of chlorothiazide of 15 mg/kg was associated with a higher risk of serum electrolyte disturbance or prescription of electrolyte supplementation compared to a total daily dose of 10 mg/kg [17]. Our findings add to this evidence demonstrating an association between higher diuretic exposure and greater change in serum sodium and chloride.
We found that as a greater amount of time elapsed between diuretic exposure and follow-up laboratory collection, there was a smaller change in serum sodium, potassium, and chloride. We speculate that this finding may reflect the influence of time and counterregulatory mechanisms in response to initial electrolyte loss over time. While we are not aware of any contemporary studies that report similar findings, recently published data report rapid tolerance to furosemide diuresis. In a retrospective cohort study of repeatedly dosed furosemide in a similar BPD population, there was a decrease in net fluid balance in the first 24 h following furosemide initiation, followed by a progressively diminishing diuretic effect over the next 48 h [26]. In the context of our study, qualifying exposures included the receipt of a single diuretic dose or the first dose of a prolonged course of diuretic. Electrolyte values collected after a longer duration from diuretic initiation may reflect the attenuating impact of time and diuretic tolerance on electrolyte derangements.
As numerous physiologic processes contribute to sodium, potassium, and chloride homeostasis, it is plausible that alternate biological mechanisms associated with electrolyte homeostasis may have contributed to our null findings, including perturbation of the hypothalamic-pituitary-adrenal axis or acute kidney injury. Adrenal insufficiency is commonly observed in infants with BPD due to prematurity and steroid exposure during NICU admission [27]. We controlled for the receipt of hydrocortisone in our model, baseline electrolyte supplementation, and increases in electrolyte supplementation during the novel diuretic exposure period therefore we speculate that adrenal insufficiency and potentially associated electrolyte derangements were unlikely to contribute to our findings. While we did not assess baseline creatinine, eGFR, or urine output in our model to account for acute kidney injury, a strength of the study includes the pre-post study design. Our assessment of within-subject change in serum sodium, potassium, and chloride would attenuate confounding due to baseline differences in renal function between groups. Additionally, we defined novel exposures to furosemide and chlorothiazide conservatively, only including infants with no diuretic exposures in the preceding 7-days. Therefore, we speculate that differences in acute kidney injury are unlikely to have contributed to the null findings of the study.
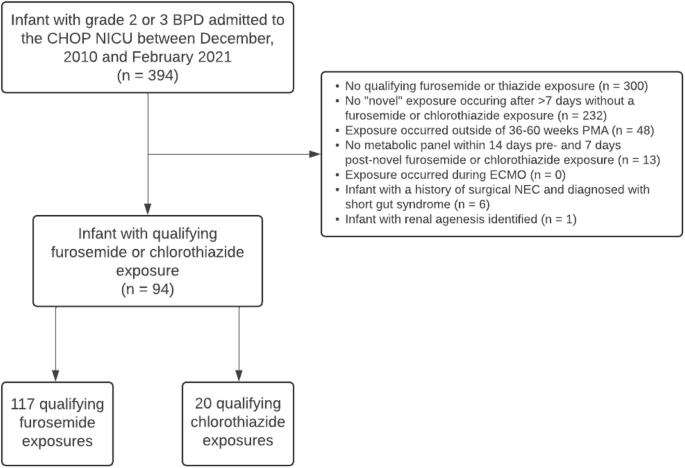
Our study has several limitations. First, it is a retrospective cohort study relying on clinical data extracted from the electronic health record, allowing for the possibility of misclassification bias from inaccurate documentation. Second, we encountered variability in the timing of electrolyte measurements relative to diuretic exposures. To mitigate bias, we included the timing of electrolyte measurement and the cumulative number of diuretic administrations received in our multivariable modeling and reported the independent effect of this expected variation in clinical practice on the observed electrolyte levels. Heterogeneity in blood sampling method (i.e. capillary vs free-flowing venous sample vs arterial sample) may also affect the reported electrolyte values. While our cohort of 94 infants is the largest cohort study evaluating serum electrolyte derangements after diuretic exposures in preterm infants with high grade BPD, our findings reflect a single center experience, and may not generalize to alternative diuretic dosing strategies. Lastly, our comparison was limited to 20 novel chlorothiazide exposures, raising the possibility of a type 2 error. To explore this limitation, we considered power calculations using a traditional approach for two independent means, assuming an alpha of 0.05 with our observed sample size and variances. We considered a change of 4 mmol/L for sodium, 1 mmol/L for potassium, and 5 mmol/L for chloride as minimally important clinical differences. Based on the subjects and data we obtained, the estimated power to detect these differences were 99% for sodium, 98% for potassium, and 99% for chloride. Although these power estimates do not reflect the full complexity of our data structure and multivariable model, they provide pragmatic reassuring estimates that our sample was adequate to detect clinically relevant difference in electrolyte changes.
Our findings contribute data to the understudied area of diuretic therapy in preterm infants with BPD. In keeping with results from our previous study, we found that chlorothiazide is not associated with less electrolyte loss compared to furosemide, challenging the assumption that it is a “gentler” diuretic in this context. Clinicians may exercise caution when considering the preferential use of thiazide diuretics if the goal is to exert a diuretic effect while lessening the impact of sodium, potassium, and chloride loss. Future studies should investigate differences in additional side effects associated with diuretic administration including calcium losses and nephrolithiasis. This study highlights the need for future prospective studies that measure electrolyte levels in a standardized manner and randomize infants to furosemide vs chlorothiazide to properly compare treatment efficacy and safety in preterm infants with BPD.


留言 (0)