This observational study aimed to evaluate the prevalence of suicidality (SI, SSI, SB, and NSSIB) in adult patients with ADHD using a dimensional approach and a validated instrument; we also analyzed socio-demographic and clinical factors potentially related to occurrence of SI, SSI, SB, or NSSIB in these patients.
The Columbia-Suicide Severity Rating Scale (C-SSRS) has enabled us to more precisely define and quantify the complex phenomenon of suicidality, which cannot be captured by a single question. As emphasized by Posner and colleagues in the original validation findings of this scale, a general desire to be dead does not pose a comparable risk factor for SB when contrasted with active SI [7]. Additionally, given the high levels of impulsivity in patients with ADHD and the associated risk of acting out, identifying those with active SI could be crucial in preventing suicide.
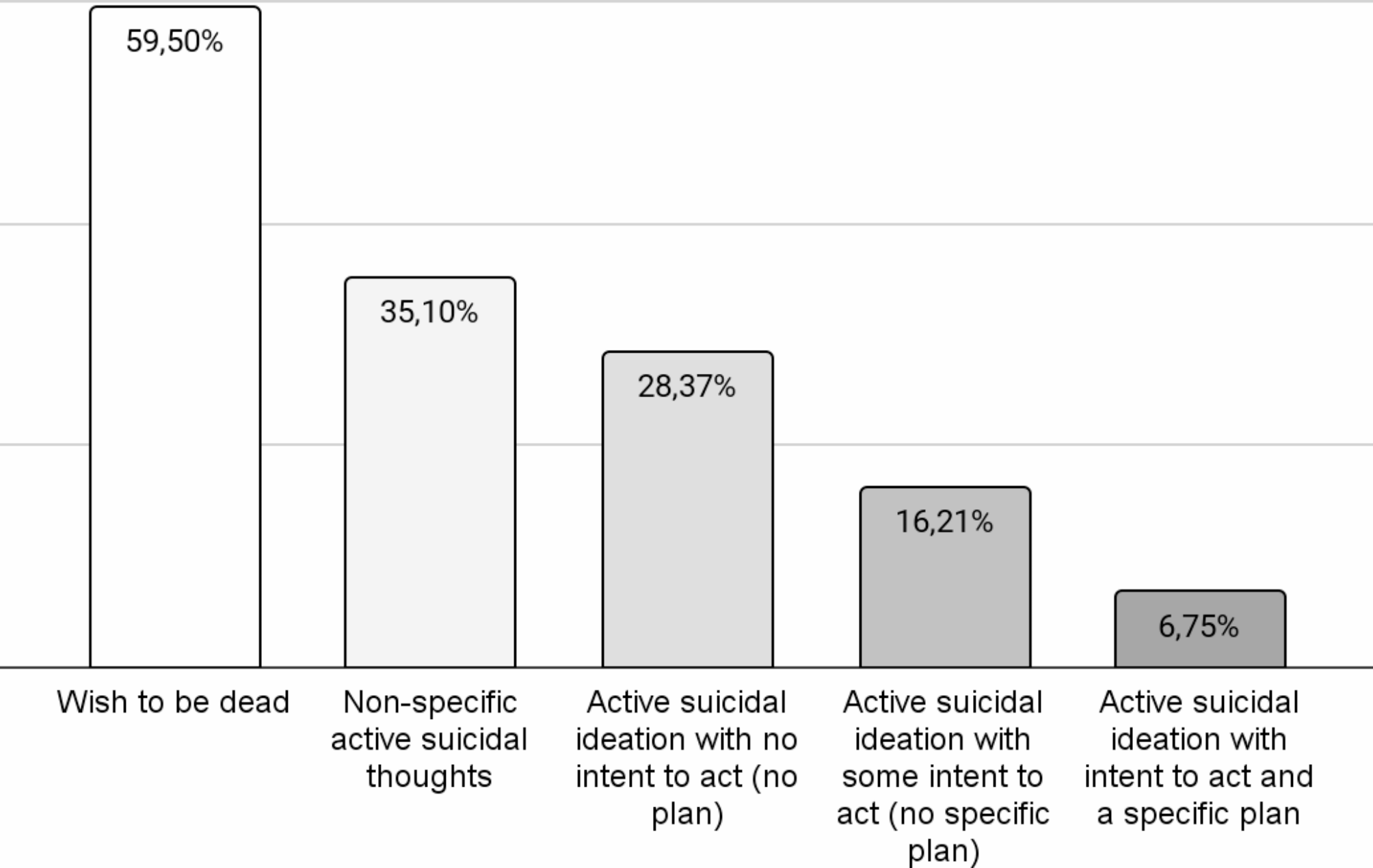
We identified a high prevalence of suicidality in adult patients with ADHD. Specifically, 59.5% of our sample reported wishing to be dead at least once in their life; moreover, 9.5% of the participants reported at least one lifetime SB. A considerable proportion of individuals with ADHD can be considered at high risk for suicide: 16.2% of our sample scored ≥ 4 on the severity scale of the C-SSRS, presenting lifetime active SI with a specific plan and intent (6.8%) or active SI with some intent to act but no plan (9.4%). Concerning SB, only a minority of our patients had actually attempted suicide (6.8%); many others, however, engaged in some SB, such as interrupted attempts (1.4%), aborted or self-interrupted attempts (2.7%), or in preparatory acts or behaviors (5.4%). Moreover, a considerable part of our sample (10.8%) engaged in NSSIB. Our results are reasonably in line with findings from a recent meta-analysis showing the lifetime prevalence of SI and SB to be 40% and 18.9%, respectively [6].
The identification of a high suicidality risk among adults with ADHD underscores the necessity for focused assessment and careful monitoring within clinical practice. Regular clinical assessments and implementation of psychoeducational interventions, not only for patients but also for their familial and caregiving networks, can be crucial tools in addressing this complex clinical concern. It is essential to assess suicidality in patients with ADHD in a dimensional manner during the initial evaluation, employing both clinical judgment and, where feasible, specific tools such as the Columbia Suicide Severity Rating Scale. For patients exhibiting a heightened risk profile, suicidality should not only be monitored as an ongoing component but also integrated into clinical outcomes and management strategies. This includes considering the use of medications that may have transdiagnostic suicidal effects, such as lithium salts [40], particularly in cases where the risk is deemed elevated.
The severity of inattentive symptoms in adulthood appeared significantly associated with lifetime SI, while the severity of hyperactivity/impulsivity symptoms did not result to have an impact on suicidality (both SI, SSI, SB and NSSIB). This evidence suggests that the association between ADHD and suicidality could be mediated by inattention, which represents the core symptom of ADHD.
In accordance with this hypothesis, the only type of impulsiveness (measured through BIS-11) which resulted associated with suicidality (specifically with SSI) in our sample was attentional impulsiveness. This has been defined as an inability to focus attention or concentrate, and it assesses task-focus, intrusive thoughts, and racing thoughts [41]. Instead, motor impulsiveness (acting without thinking) and non-planning impulsiveness (lack of “futuring” or forethought) did not result to affect both SI and SB, confirming that the risk of suicide in ADHD patients could depend on inattention rather than impulsivity itself.
Furthermore, while lifetime SI appeared related to the severity of inattentive symptoms in adulthood, we found that lifetime SSI was associated with the severity of inattentive symptoms during childhood. This result endorses the potential impact in adulthood of the symptoms during childhood, underlining that the intensity of symptoms during this critical developmental period plays a more crucial role in influencing suicidality risk than the timing of the diagnosis itself. Previous research has identified several predictive factors for suicidality in ADHD, such as early externalizing behaviors, adverse childhood experiences, and negative father-daughter interactions, while not placing emphasis on inattentive symptoms [42]. Therefore, considering SSI as the proper risk factor for suicide, exploring symptoms of attention deficit in childhood should be a target in ADHD patients. However, in clinical practice, identifying this cluster in childhood can be challenging due to the occasional unavailability of caregivers and the less overt presentation of inattention, which is not always the predominant feature of ADHD, particularly in children.
It is important to underline that in our sample SI, SSI, SB and NSSIB did not appear associated with any psychiatric comorbidity, in line with prior research findings from Septier’s et al. meta-analysis [6].
Furthermore, we did not find any clinical or socio-demographic factors significantly associated with SB and NSSIB in adult patients with ADHD, indicating a direct correlation between these phenomena.
Unlike SB and NSSIB, other clinical factors were found to be associated with SI and SSI in addition to the previously mentioned inattentive symptoms and attentional impulsiveness. Patients with SI exhibited significantly more frequent impairments in social functioning, though not in other areas. This finding, consistent with existing literature, supports the notion of a causal link between social isolation and suicide, as well as the protective influence of social support against suicide [43]. Physical activity appeared to be associated with a lower lifetime prevalence of SSI, suggesting that being physically active could reduce suicidal risk. While engaging in physical activity has proven to be a protective factor against SSI, the intensity of the activity did not appear to be correlated with the risk, suggesting that even light-intensity physical activity can be protective. This evidence aligns with a recent meta-analysis conducted on psychiatric patients [44] and is significant considering that there are only a limited number of interventions that have demonstrated effectiveness against suicide, and these are not always accessible within public health systems. Indeed, only a few medications have been shown to clearly reduce suicidal risk, such as lithium, ketamine and clozapine [45, 46]. Meanwhile, interventions like cognitive-behavioral therapy have proven effective but are often not readily available within public health systems [45].
Low self-esteem is a known risk factor for suicide, especially in emerging adulthood [47]. It appeared significantly related with lifetime SI (it was found in 84.1% of the patients with suicidality history), but it is important to underline how frequently it occurs also in patients without an history of SI/SSI/SB/NSSIB (60%), being one of the most associated symptoms in ADHD.
No gender differences emerged regarding both SI, SSI, SB and NSSIB in our sample.
Our study has several strengths, including a well-characterized clinical sample comprised of carefully diagnosed patients with thorough evaluations of their ADHD symptoms and comorbidities, the use of standardized validated assessments, and a dimensional approach. However, our study should be considered in light of some limitations. First, the cross-sectional design does not allow for the inference of causal relationships or the evaluation of etiological factors. Another limitation of our study is the gender ratio of approximately 2:1 (males to females) among the patients, which, although slightly higher than the 1.7:1 ratio reported in the literature [48], is still consistent with the general epidemiology of the disorder. Furthermore, while we addressed various aspects of emotional dysregulation (such as anger control, mood reactivity, and frustration tolerance), we did not comprehensively cover emotional dysregulation in its entirety. The absence of patients with the predominantly hyperactive-impulsive subtype and the high prevalence of single patients represent a potential additional barrier to the generalization of our results, as well as the low prevalence of familial ADHD in our sample limits our ability to generalize the results and precludes us from excluding a potential protective role of familial ADHD in suicidality. Additionally, the sample did not include individuals who had completed suicide, which means we cannot determine if the results apply to suicide deaths. Another significant limitation of this study is the small number of participants, which renders the results regarding potential predictors of SB/NSSIB preliminary. Additionally, the absence of a comparison group from the general population further limits the ability to contextualize these findings. It is, therefore, not possible to rule out the possibility that the risk of SB and NSSIB is mediated by factors such as personality disorders or specific temperaments. These traits are particularly prevalent among adults with ADHD [49], contributing to greater functional impairment and reduced treatment response [50], and have also been associated with suicidality dimensions [8].
Despite these limitations, our findings are noteworthy since they highlight that a significant proportion of patients with ADHD have lifetime SI/SB. Moreover, this association appeared not to be affected by psychiatric comorbidities. Instead, our findings suggest that the risk of suicide in ADHD patients could depend on inattention itself. Interestingly, this dimension may be more closely associated with suicidality severity due to several interrelated psychological and social factors. Specifically, individuals exhibiting higher levels of inattention might experience lower self-esteem, a pervasive sense of hopelessness, limited opportunities for personal and professional development, decreased engagement in social situations, and heightened feelings of isolation. These elements can create a detrimental emotional environment that exacerbates suicidality risk, suggesting a complex interplay between ADHD symptoms and the psychosocial challenges faced by these individuals. In conclusion, adult patients with ADHD can be considered at risk of suicide, and it is important to identify which patients are at higher risk, in order to guide preventive pharmacological or psychological treatments and psychoeducational interventions. Therefore, for adult ADHD patients, alongside pharmacological therapy, the utilization of psychotherapeutic interventions, particularly cognitive-behavioral and psychoeducational approaches, is crucial. These interventions aid patients in gaining a deeper understanding of their condition, enhancing self-esteem, and guiding them towards adopting healthy and protective lifestyles, such as regular physical activity.
Future research should aim to replicate our findings in a larger sample to enhance generalizability and robustness. Additionally, it would be beneficial to integrate cognitive assessments specifically focused on the attentional dimension, as well as other cognitive measures, to further explore their associations with dimensions of suicidality. Furthermore, it would be valuable to examine how previous psychotherapy experiences, as well medications and psychosocial interventions (whether individual or family-based) influence suicidality. Such investigations could provide important insights into effective management strategies for individuals with ADHD.









留言 (0)