
記住我
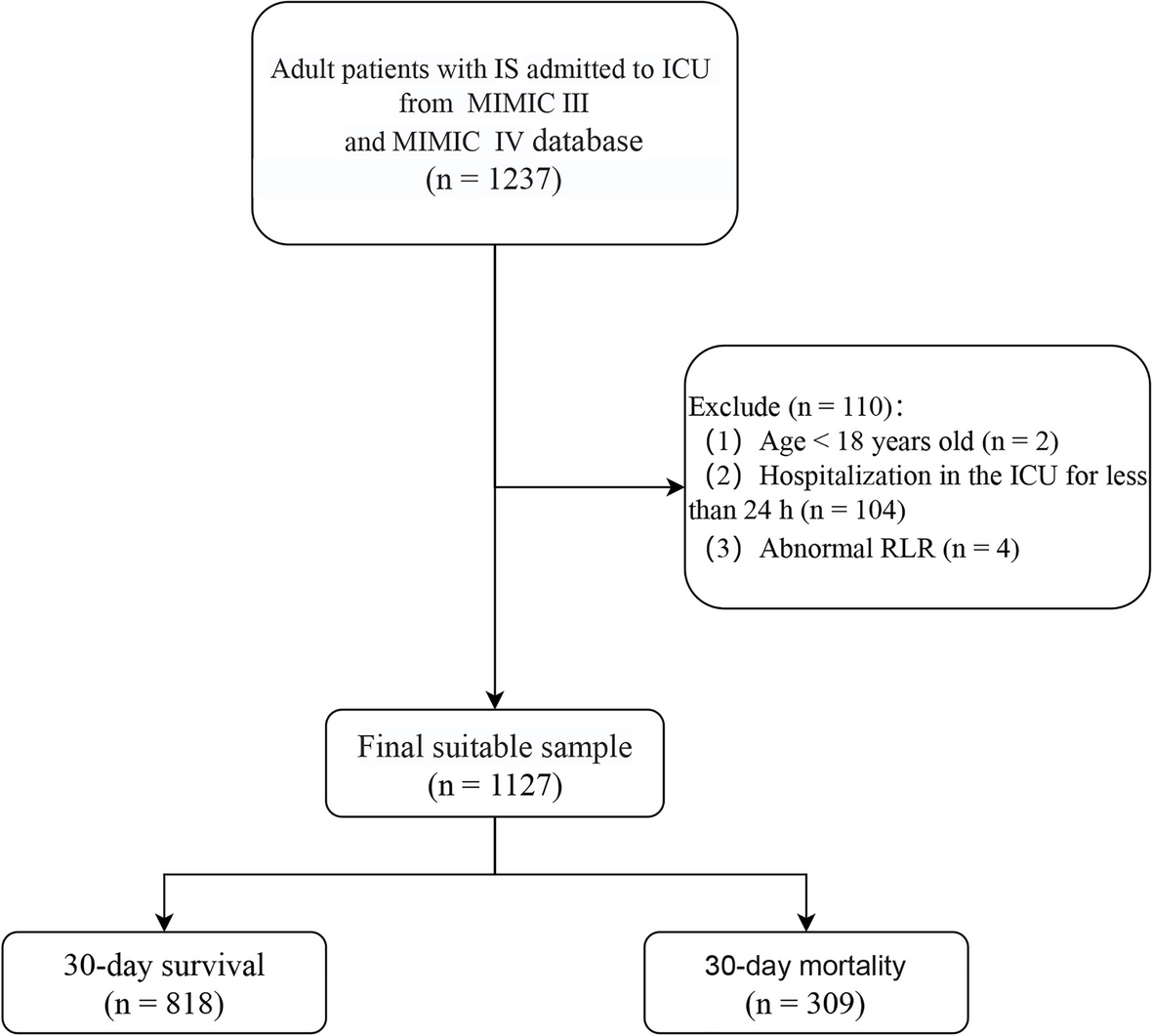








After screening according to inclusion and exclusion criteria, a total of 196 patients [male: 92 (46.9%); age (mean ± SD): 38.17 ± 13.64] were enrolled in this study eventually. 85 patients [male: 35 (41.2%); age: 38.07 ± 13.59] were diagnosed with severe CVT, while 35 [male: 10 (28.6%); age: 38.29 ± 13.83] and 14 patients [male: 5 (35.7%); age (mean ± SD): 43.21 ± 19.70] experienced short-term and long-term poor outcomes, respectively. The screening process of enrolled patients is shown in the flow chart (Fig. 1). More details of demographic characteristics are shown in Table 1. In this study, fibrinogen, D-dimer, and DFR values did not follow a normal distribution. Therefore, results were presented using quartiles, and all related analyses employed non-parametric tests.
Fig. 1
Flow-chart. CVT: cerebral venous thrombosis; mRS: modified Rankin Scale
Table 1 Baseline characteristicsDFR and the severity of CVTA cohort of 85 patients met the diagnostic criteria for severe CVT, manifesting mental status disorder (15.3%), deep cerebral venous thrombosis (17.6%), coma (14.1%), and cerebral hemorrhage (76.5%). Beyond the hallmarks of severe CVT, these patients also exhibited significantly elevated incidences of focal neurological deficits (38.8% vs. 25.2%, P = .002), seizures (44.7% vs. 24.3%, P < .001), venous cerebral infarction (70.6% vs. 35.1%, P < .001), endovascular interventions (47.1% vs. 28.8%, P = .009), and decompressive craniectomy (8.72% vs. 0%, P = .007) compared to those with non-severe CVT. Notably, severe CVT patients had significantly higher DFR values (median [IQR]: 0.38[0.20, 0.82] vs. 0.17[0.07, 0.44], P < .001) compared to non-severe CVT (Table 1).
Significant difference in DFR values were observed in the subgroup analysis, with all significance levels reaching below 0.001. Patients with seizures (median [IQR]: 0.42[0.22, 1.01] vs. 0.18[0.09, 0.45], P < .001), venous infarction (median [IQR]: 0.37[0.20, 0.75] vs. 0.15[0.07, 0.46], P < .001), mental status disorder (median [IQR]:0.67[0.26, 1.12] vs. 0.23[0.10, 0.54], P < .001), coma (median [IQR]:0.67[0.25, 1.12] vs. 0.23[0.10, 0.54], P < .001), and cerebral hemorrhage (median [IQR]:0.38[0.21, 0.91] vs. 0.19[0.09, 0.48], P < .001) have higher DFR level compared to their counterparts without these conditions (Supplementary Table 1). In other subgroups, including headache, neurological deficits, multiple venous thromboses, and deep cerebral venous thrombosis, no significant differences in DFR levels were observed.
ROC curve analysis underscored DFR’s predictive capability for severe CVT, achieving an AUC of 0.690 (95% CI: 0.617–0.764, P < .001) with an optimal cutoff value of 0.253 (sensitivity 68.2% [95%CI: 64.9–71.6], specificity 64.0% [95%CI: 60.9–67.3]). (Fig. 2.a). DFR was included in the regression analysis as a categorical variable (≥ 0.253 or < 0.253).
Fig. 2
Receiver operating characteristic curve for DFR on predicting severe CVT (a), poor short-term outcome (b) and poor long-term outcome (c). AUC: area under the curve, CI: confidence interval
Univariate logistic regression analysis showed that DFR ≥ 0.253 was significant predictor of severe CVT [ odds ratio (OR) (95% CI): 2.89 (1.57–5.34), P < .001] (Supplementary Table 2). After adjusting all variables, multivariate logistic regression analysis showed that DFR ≥ 0.253 was also significant predictor of severe CVT [adjusted OR (95% CI): 1.95 (1.05–3.61), P = .033]. This association persisted even after adjusting for variables demonstrating a clear correlation in the univariate analysis [adjusted OR (95% CI): 2.03 (1.10–3.75), P = .024]. (Fig. 3).
Fig. 3
Multivariate logistic regression analyses for association of variables with severe CVT. DFR: D-dimer to fibrinogen ratio; aOR: adjusted odds ratio; CI: Confidence interval. Model 1: Multivariate regression models constructed for all variables. Model 2: The multivariate regression model is constructed in the univariate regression analysis of variables with significant correlation with DFR. * P < .05; ** P < .017
DFR and short-term outcome of CVTA cohort of 196 patients was stratified into two groups based on their mRS scores at discharge, delineating good versus poor short-term outcomes. Notably, the frequency of male patients in the poor prognosis group was significantly diminished compared to the good outcome cohort (28.6% vs. 50.9%, P < .001). Patients with poor short-term outcomes demonstrated a higher DFR (median [IQR]: 0.71[0.35, 1.10] vs. 0.20[0.10, 0.47], P < .001), a shorter interval from symptom onset to hospital admission (mean ± SD: 7.46 ± 5.90 days vs. 10.08 ± 5.78 days, P = .020), and an increased prevalence of focal neurological deficits (62.9% vs. 24.2%, P < .001), seizures (68.6% vs. 25.5%, P < .001), venous infarctions (85.7% vs. 42.9%, P < .001), mental status alterations (28.6% vs. 1.9%, P < .001), coma (28.6% vs. 1.2%, P < .001), cerebral hemorrhages (71.4% vs. 24.8%, P < .001), and severe CVT (82.9% vs. 34.8%, P < .001). Additionally, interventions such as endovascular treatments (60.0% vs. 31.7%, P < .001) and decompressive craniectomy (20.0% vs. 0%, P < .001) were markedly higher in the poor outcome group. These findings are detailed in supplementary Table 3.
Variables exhibiting significant collinearity with DFR are detailed in supplementary Table 4, including duration from onset to admission (correlation coefficient: -0.26, P = .000), seizure (0.22, P = .000), mental status disorder (0.17, P = .018), coma (0.19, P = .007), venous cerebral infarction (0.17, P = .018), cerebral hemorrhage (0.23, P = .001), and deep cerebral venous thrombosis (0.14, P = .049). These variables were not included as confounding factors in the multivariate logistic regression analysis examining the correlation between DFR and prognosis.
The ROC curve for baseline DFR underscored its predictive utility for discerning poor short-term outcomes, with an AUC of 0.773 (95% CI: 0.701–0.845, P < .001). An optimal DFR cutoff of 0.322 was identified, exhibiting a sensitivity of 82.9% (95%CI: 78.6–87.1) and a specificity of 63.4% (95%CI: 59.4–67.6) (Fig. 2.b). DFR was included in the regression analysis as a categorical variable (≥ 0.322 or < 0.322).
Univariate logistic regression analysis identified DFR ≥ 0.322 as a significant forecaster of adverse short-term outcomes [OR (95% CI): 2.70 (1.51–4.76), P < .001] (Supplementary Table 5). Multivariable logistic regression, refined to exclude variables showing significant collinearity with DFR, reaffirmed the predictive value of DFR ≥ 0.322 for poor short-term prognosis [adjusted OR (95% CI): 2.63 (1.47–5.88), P = .003], even after adjusting for factors closely associated in univariate analysis [adjusted OR (95% CI): 2.63 (1.43–4.76), P = .002] (Fig. 4).
Fig. 4
Multivariate regression analyses for association of variables with poor short-term outcome at discharge. DFR: D-dimer to fibrinogen ratio; aOR: adjusted odds ratio; CI: Confidence interval. Variables with significant collinearity to DFR were not included in the multiple regression analysis model. Model 1: Multivariate regression models constructed for all variables that are not collinear with DFR. Model 2: The multivariate regression model is constructed in the univariate regression analysis of variables with significant correlation and not collinear with DFR. * P < .05; ** P < .017
DFR and long-term outcome of CVTA total of 196 patients were stratified into two cohorts based on their 12-month mRS scores, delineating groups with either good or poor long-term outcomes. Baseline demographics and clinical characteristics are detailed in supplementary Table 6. Analysis revealed that patients categorized within the poor long-term outcome group exhibited significantly elevated DFR levels (median [IQR]: 0.89[0.36, 1.43] vs. 0.24[0.11, 0.57], P = .002) compared to their counterparts with good outcomes. Furthermore, the poor outcome group was characterized by a notably shorter median interval from symptom onset to hospital admission (4.479 ± 5.90 vs. 9.98 ± 6.06, P = .020), alongside increased incidences of seizures (71.4% vs. 28.1%, P < .001), venous infarctions (92.9% vs. 47.3%, P = .001), mental status disorders (28.6% vs. 1.9%, P < .001), coma (42.9% vs. 3.3%, P < .001), cerebral hemorrhages (64.3% vs. 30.8%, P = .016), and severe CVT (78.6% vs. 40.7%, P = .006). Additionally, the utilization of decompressive craniectomy was significantly more frequent in the poor long-term outcome group (21.4% vs. 2.2%, P = .009).
The ROC curve analysis for baseline DFR confirmed its predictive capability regarding poor long-term outcomes, with an AUC of 0.753 (95% CI: 0.619–0.886, P = .002). The optimal DFR threshold was determined to be 0.754, achieving a sensitivity of 64.3% (95%CI: 56.2–72.4) and a specificity of 83.0% (95%CI: 73.9–92.9) (Fig. 2.c). DFR was included in the regression analysis as a categorical variable (≥ 0.754 or < 0.754).
Univariate logistic regression analysis identified DFR ≥ 0.754 as a significant predictor of poor long-term outcomes [OR (95% CI): 1.66 (1.39–5.56), P = .004] (Supplementary Table 7). In the multivariate logistic regression model, after excluding variables with significant collinearity with DFR, DFR ≥ 0.754 remained a strong independent predictor of poor long-term outcomes [adjusted OR (95% CI): 3.22 (1.39–7.14), P = .006]. This association persisted even after adjusting for variables demonstrating a clear correlation in the univariate analysis [adjusted OR (95% CI): 2.86 (1.32–6.25), P = .008] (Fig. 5).
Fig. 5
Multivariate regression analyses for association of variables with poor long-term outcome at 12-months. DFR: D-dimer to fibrinogen ratio; aOR: adjusted odds ratio; CI: Confidence interval. Variables with significant collinearity to DFR were not included in the multiple regression analysis model. Model 1: Multivariate regression models constructed for all variables that are not collinear with DFR. Model 2: The multivariate regression model is constructed in the univariate regression analysis of variables with significant correlation and not collinear with DFR. * P < .05; ** P < .017
留言 (0)