
記住我

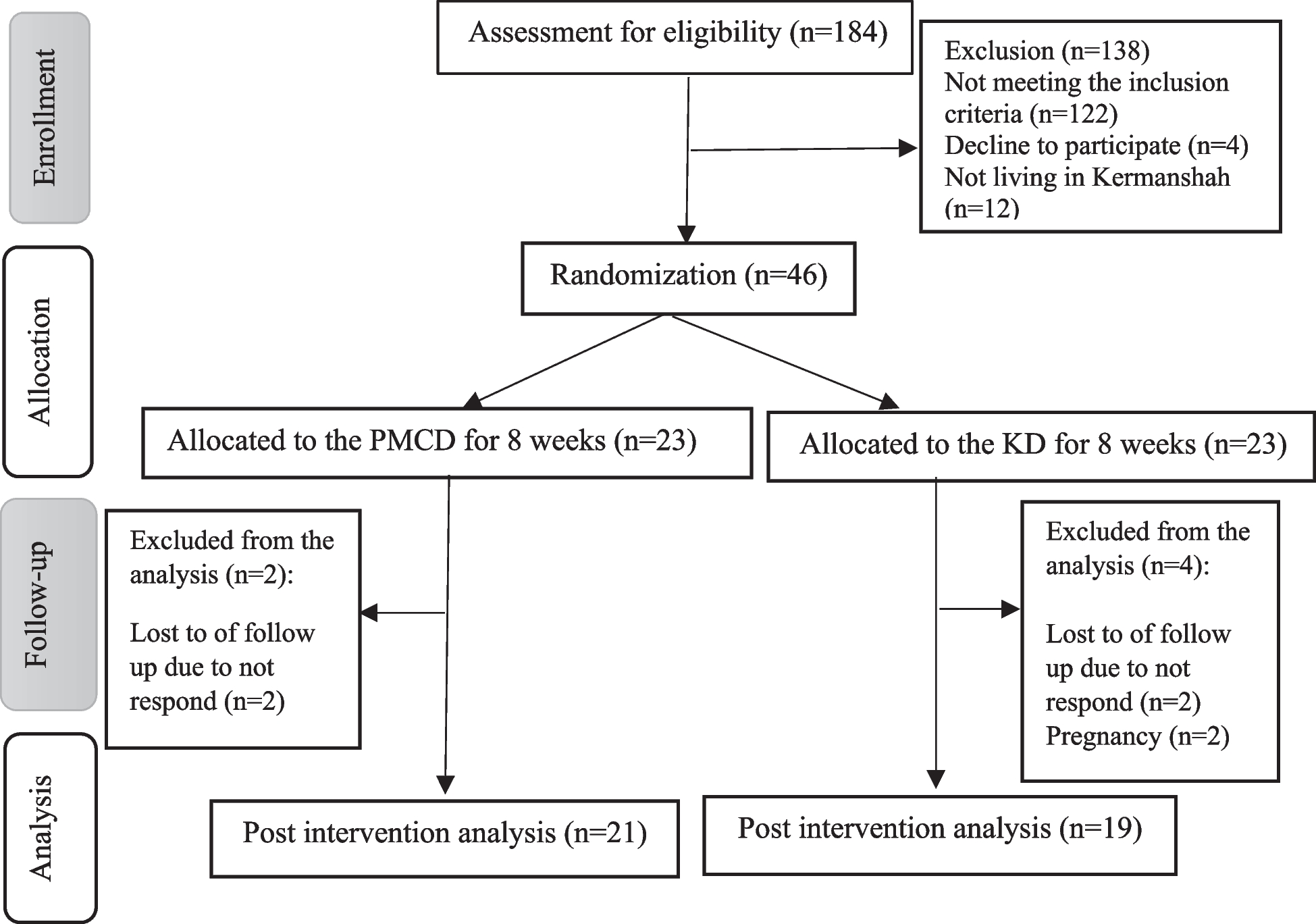


Details of the study design and some major results of the CHNS have been described elsewhere [25,26,27,28]. Briefly, the CHNS is an ongoing, national, multipurpose, longitudinal, open cohort study initiated in 1989 and has been followed up every 2–4 years. By 2011, the provinces included in the CHNS constituted 47% of China’s population [26]. The present study was based on 6 rounds of CHNS data from 1997 to 2011 (1997, 2000, 2004, 2006, 2009, and 2011), including a total of 82,343 person-waves. We first excluded participants who were pregnant or < 18 years old. Among the remaining participants (including 65,611 person-waves), those with missing diabetes diagnoses (including 3895 person-waves) or with only one survey wave (including 8841 person-waves) were further excluded. Therefore, a cohort based on 13,500 participants (including 52,875 person-waves) with two or more survey waves was identified, and the first survey round was considered as the baseline. Of the 13,500 participants, 213 participants with self-report diabetes at baseline and 712 with extreme dietary energy data (males: > 4200 or < 800 kcal/day; females: > 3600 or < 600 kcal/day) [29] were further excluded. Ultimately, a total of 12,575 participants were included in the final analysis (Fig. 1).
Fig. 1
Flow chart of the study participants
The characteristics of the included (n = 12,575) and excluded (n = 8061) populations are shown in Table S1. The institutional review boards of the University of North Carolina at Chapel Hill, the National Institute of Nutrition and Food Safety, and the Chinese Center for Disease Control and Prevention approved the study. Each participant provided written informed consent. The data and study materials that support the findings of this study can be found on the official CHNS website.
Assessment of the Mediterranean DietThe dietary intake of each participant was assessed using 24-h recalls for three consecutive days (2 weekdays and 1 weekend day). Researchers at the CHNS recorded the types and amounts of food consumed at each meal during the previous day. Detailed information on the data collection has been reported previously [30, 31]. In the analyses, 3-day average intakes of dietary intake in each round were calculated. Repeated 3-day dietary recalls may reduce the day-to-day variation in dietary intake, and collect more complete food information. Moreover, all values of each nutrient in the analyses, if not specified, were presented as the cumulative averages, using all results from baseline to the last visit or the date of new-onset diabetes, to represent long-term dietary intake status and minimize within-person variation.
We used the MDA score scale proposed by Trichopoulou [24, 32]. This scale includes nine components: vegetables, legumes, fruits, nuts, cereals, fish, meat, dairy products, and alcohol. Values of 0 or 1 were assigned to each of the components, using the sex-specific median values for the participants as cutoffs for all components except for alcohol and dairy. For the six components presumed to be beneficial (vegetables, legumes, fruits, nuts, cereals, and fish), participants whose intake was at or above the sex-specific medians were assigned a value of 1, while those whose intake was below these medians were assigned a value of 0. For meat, a value of 0 was assigned to participants whose intake was above the median, while those whose intake was below the sex-specific median were assigned a value of 1. For alcohol intake, a value of 1 was assigned to men who consumed 10–50 g/day and women who consumed 5–25 g/day. For dairy products, a value of 1 was assigned to those whose daily intake was between 5 and 25 g. The scores of the nine categories were summed. The total range of the MDA score was from 0 to 9. The MDA score was calculated for all individuals upon recruitment. MDA was categorized into three levels, below the median (score 0–3), median (score 4), or above the median (score 5–9) [33], using the low level as the reference level.
Assessment of other covariatesInformation on age, sex, body mass index (BMI), urban or rural residence, region, education level, occupation, income, physical activity, smoking status and cumulative average total energy intake was obtained from the questionnaires at each follow-up survey. Height and weight were measured following a standard procedure with calibrated equipment. BMI was calculated as weight (kg) by height squared (m2). The level of physical activity was the product of the self-reported time spent in each activity multiplied by specific metabolic equivalent (MET) values [34]. For all the nondietary covariates, we used the baseline year measurements. The cumulative average total energy intake was calculated using 3-day average intakes of dietary intake in each round.
Study outcomeDiabetes status was identified by a questionnaire-based interview at each follow-up. In the physical examination questionnaire, two questions were used to collect diabetes diagnosis data: (a) Has the doctor ever told you that you suffer from diabetes? If yes, (b) did you use any of the following treatment methods? (1) special diet, (2) weight control, (3) oral medicine, (4) injection of insulin, (5) Chinese traditional medicine, (6) home remedies, and (7) Qi Gong (Spiritual). The participants who answered yes to the question “a” were classified as diabetes cases in the primary analysis. In CHNS, data of blood glucose and HbA1c were only available in the wave of 2009. To test the reliability of self-reported diagnosis, we used two more criteria defining diabetes cases in sensitivity analysis, which were (1) self-reported cases based on the question “a” and cases identified based on blood glucose and HbA1c (fasting blood glucose ≥ 7.0 mmol/L or HbA1c ≥ 6.5%) in the wave of 2009, and 2) cases using oral hypoglycemic medicine or insulin injection based on question “b” [35].
Statistical analysisThe population characteristics are presented as the means ± standard deviations (SDs) or medians (IQRs) for continuous variables and proportions for categorical variables. Differences in population characteristics by MDA scores were compared using one-way ANOVA tests, Kruskal–Wallis test, or chi-square tests, accordingly.
The year of each participant’s first entry into the survey was considered as a baseline. The follow-up person-time for each participant was calculated from baseline until the first new-onset diabetes diagnosis, the last survey round before the participant departed from the survey, or the end of the latest survey (2011), whichever came first. Participants were censored on the date of the last survey round before the participant departed from the survey or the end of the latest survey. The incidence rates of new-onset diabetes, expressed as person-years, were calculated as the sum of follow-up years for participants.
Variables that are known to be traditional or suspected risk factors for diabetes or variables that showed significant differences among different MDA score levels were chosen as the covariates in the adjusted models. The relationships between the MDA score and new-onset diabetes were estimated using Cox proportional hazards models. Model 1 included adjustments for age and sex. Model 2 included the adjustments in Model 1 plus BMI, occupation, education level, region, smoking status, urban or rural residence, income, physical activity (low, moderate, high) at baseline, and cumulative average total energy intake. We also used restricted cubic splines (RCS) with 3 knots to explore the potentially non-linear relationship of MDA score with new-onset diabetes with adjustments in Model 2. Moreover, possible modifications of the association between MDA score and new-onset diabetes were evaluated by stratified analyses and interaction testing. Those with missing values of covariates were excluded from the main analysis. A series of sensitivity analyses were conducted to test the robustness of our findings, such as (1) both self-reported cases and cases diagnosed by blood glucose and HbA1c in the wave of 2009 were defined as diabetes cases, (2) only cases taking oral hypoglycemic medicines or insulin injection were defined as diabetes cases, (3) multiple imputations were also used to handle missing covariates.
A two-sided P value < 0.05 was considered to indicate statistical significance in all analyses. All the statistical analyses were conducted using Stata 17 and R version 3.6.3.
留言 (0)