This prospective, single-center, observational study was conducted at B.P. Koirala Institute of Health Sciences (BPKIHS) from January 2021 to February 2022. Ethical approval was obtained from the Institutional Review Committee (IRC) of BPKIHS (reference number: IRC/1872/020). The study was registered prior to patient enrollment at clinicaltrials.gov (NCT04692870, Principal investigator: Shirish Silwal, https://clinicaltrials.gov/ct2/show/NCT04692870, Date of registration: January 5, 2021). Written informed consent was obtained from participants either in the labor room or obstetric emergency ward prior to the study procedure. This study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
The study included term pregnant laboring women (gestational age ≥ 37 weeks) with American society of Anesthesiology physical status (ASA PS) II who underwent emergency CS under spinal anesthesia, and with categories either 2 (no immediate threat to life of pregnant women and fetus) or 3 (requiring early delivery) based on NICE (National Institute for Clinical Excellence) guidelines. [15] Parturient with pregnancy induced hypertension, gestational hypertension, known fetal abnormalities, contraindication to spinal anesthesia, multiple gestation, baseline systolic blood pressure (SBP) < 100 mmHg, intrauterine growth restriction, stillbirth, height < 150 cm, antepartum hemorrhage, gestational diabetes, cardiovascular, cerebrovascular, endocrine disease, and those requiring conversion to general anesthesia (GA) were excluded from the study.
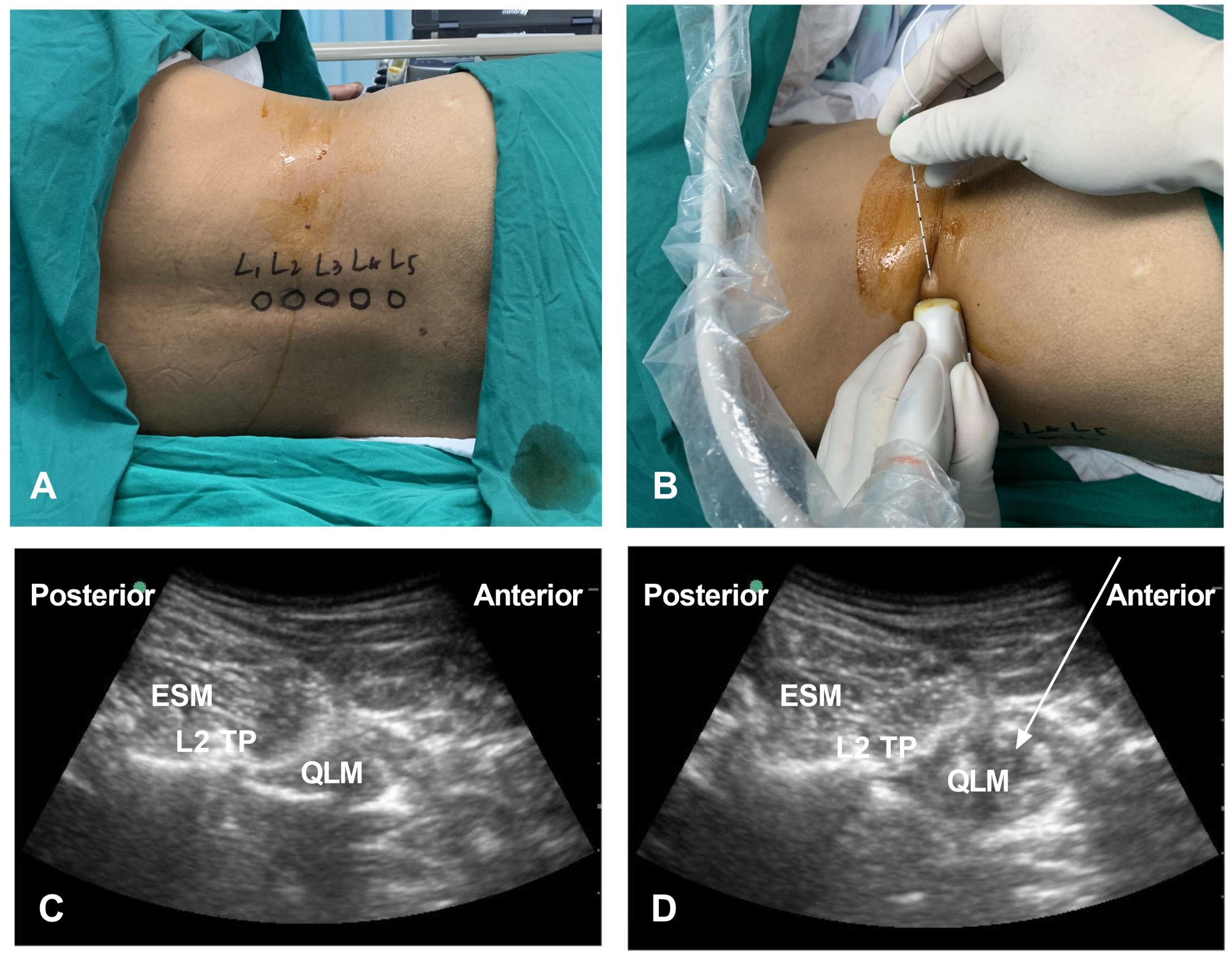
During the pre-anesthetic visit, patients’ data that included age, gestational age, height, weight, body mass index (BMI), indication for CS, and preoperative anxiety assessed with Nepali version of Amsterdam preoperative anxiety and information scale (APAIS) [16] were recorded. Before the patient was shifted to the operating room (OR), ranitidine 50 mg and metoclopramide 10 mg was administered intravenously via 18 G cannula. Once in the OR, patients were positioned supine with a 15° left lateral tilt, and standard monitors were attached to record their 3-lead ECG, pulse oximetry, and noninvasive blood pressure. The patient’s systolic blood pressure (SBP) and heart rate (HR) were measured three times, with each measurement taken one minute apart. The averages of these measurements were recorded as the baseline SBP and HR. Also, shock index (HR / SBP) was calculated before administering spinal anesthesia. Vein patency was maintained with a minimal rate infusion of Ringer’s lactate (RL) solution. In sitting position and under all aseptic precautions, 2.0 ml of 0.5% hyperbaric bupivacaine with 10 µg fentanyl was administered in L4- L5 or L3- L4 interspace with 25 G spinal needle, after ensuring free flow of cerebrospinal fluid. The patient was then placed in a supine position with a right hip wedge, and immediately after the spinal injection, 1 L of RL was rapidly co-loaded over 10 – 15 min using pressure bag, while a phenylephrine infusion was started at a rate of 25 μg/min. Ondansetron 4 mg IV was given to all patients after spinal anesthesia. Surgery commenced once the sensory level reached T6, which was determined by checking for loss of cold sensation with alcohol-soaked cotton swabs. Hemodynamic parameters were measure at baseline, immediately after spinal anesthesia, every minute for the first 15 min after spinal injection, and every 2.5 min until the end of surgery.
Hypotension (SBP < 80% of baseline or SBP < 100 mmHg) was treated with phenylephrine 50 µg bolus and rapid infusion of RL 200 ml. If the hypotension was associated with bradycardia (HR < 55 beats/min), an IV injection of atropine 0.5 mg was given. Intraoperative hypertension (defined as SBP greater than 120% of the baseline reading) managed by temporarily stopping phenylephrine infusion and resuming it when the SBP returned to within 20% of the baseline reading. After the baby was delivered, 3 IU of oxytocin was administered IV over at least 30 s followed by an infusion of 10 IU/h. The amount of IV fluids given during surgery, estimated blood loss, and use of uterotonic agents were all recorded. Intraoperative nausea or vomiting (IONV) was treated with IV dexamethasone 4 mg. Incidences of intraoperative pruritus and shivering were also recorded and treated accordingly. The primary outcome measure was the occurrence of post spinal hypotension, defined as SBP < 80% of the baseline reading or SBP < 100 mmHg from the administration of spinal anesthesia until the delivery of the baby. The secondary outcome measure was post-delivery hypotension, defined as SBP < 80% of baseline reading or SBP < 100 mmHg observed from the initiation of oxytocin until the end of surgery.
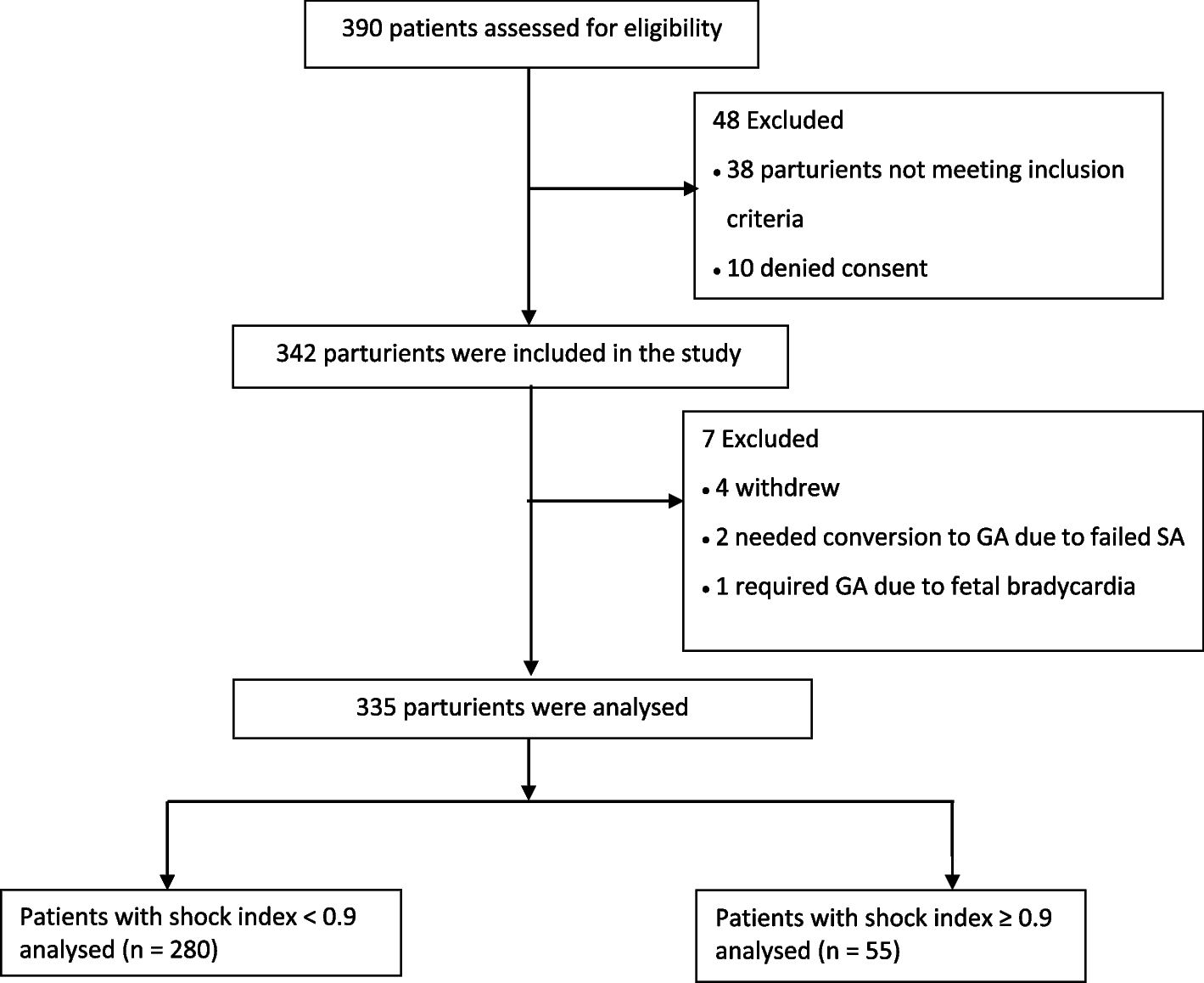
Based on previous studies, [3,4,5,6] we estimated an approximate 34% occurrence of post-spinal hypotension. The sample size calculation was based on a rule of 10–15 events per risk predictor variable in logistic regression. [17] We used formula [N = (n × 15) / I], where N represents the required sample size, n is the number of variables to be tested, and I is the incidence of the primary outcome. The number of potential risk predictor variables to be included in the model was seven (Age, baseline SBP, baseline HR, baseline SI, maximum block height, BMI, preoperative anxiety), and with 15 events per covariate, it required 105 events. Dividing 105 events by the estimated occurrence of post-spinal hypotension resulted in 308 participants. We accounted for a 10% dropout rate and calculated an adjusted sample size of 342 participants using the formula, calculated sample size ÷ (1—dropout rate).
Data normality was assessed by skewness and kurtosis, Shapiro–Wilk test, and by visually inspecting histograms. Patient data was presented as the mean (standard deviation) or median (Interquartile range) or frequency (percentage). Demographic and surgical profiles of the parturient, baseline and intraoperative hemodynamic parameters, and neonatal outcomes were compared using unpaired t-test or Mann–Whitney test, as appropriate. Chi-square tests were used for categorical variables or Fisher exact tests if expected cell counts were less than five. We conducted univariable and multivariable logistic regression analysis to explore the association between baseline shock index (categorized as < 0.9 and ≥ 0.9) and hypotension after spinal anesthesia. Variables that were univariably associated (P < 0.15) with hypotension, along with clinically relevant variables, were included in the multivariable model building. It was reported as odds ratios (OR) with 95% confidence intervals (CI). We assessed the degree of multicollinearity using the variance inflation factor (VIF) and dropped variables with VIF value > 10. The diagnostic ability of the baseline SI to predict post-spinal and post-delivery hypotension was analyzed using receiver operating characteristic (ROC) curves. We used Hosmer–Lemeshow test to assess the goodness of fit of the logistic regression for multivariable analysis and characterized the multivariate model discrimination using a ROC curve C statistic. A P- value < 0.05 was considered statistically significant. Stata version 15.0 (StataCorp LP, College Station, TX, USA) was used for all analysis.







留言 (0)