
記住我






This study aimed to evaluate the efficacy of QLBi for postoperative pain management in patients who underwent open inguinal hernia repair with mesh. The study was registered on the Chinese Clinical Trial Registry (June 2, 2018; ChiCTR1800016457) and conducted from July 2018 (first patient enrolled: July 9, 2018) to June 2019 (last patient completed: June 27, 2019). This study was approved by the ethics committee of the First Affiliated Hospital of Wenzhou Medical University (clinical research ethics number 2018-033). Written informed consent was obtained from all patients included in the study.
Sample size calculationBased on previous research, the standard deviation of the injection block range at the L2 level is 0.77 segments. In this study, the sample size was calculated using PASS software, with a confidence level of 95% and an expected standard error of 0.5 segments. The required sample size was determined to be 18. Considering a 10% dropout rate, the final sample size for this study was set at 20.
Study populationTwenty volunteers who were scheduled to undergo open inguinal hernia repair with mesh were selected for this study. The inclusion criteria were age 18–60 years, intact skin sensation in the abdomen, ASA I-II classification, and willingness to undergo open inguinal hernia repair with mesh. The exclusion criteria were body mass index (BMI) < 18 kg/m2 or > 30 kg/m2, language communication and comprehension disorders, history of local anesthesia allergy, spinal deformity, peripheral nerve disorders, and spinal cord dysfunction.
QLBi procedureThe volunteers fasted for 8 h and were prohibited from drinking water for 2 h before surgery. Routine monitoring of blood pressure, electrocardiogram, pulse oximetry, and forearm vein puncture was performed before the operation. A sedative and analgesic mixture of midazolam (1 mg/ml) and fentanyl (20 µg/ml) was intravenously administered at a dose of 1–2 ml to reduce discomfort caused by needle puncture. The volunteers were placed in the lateral position for the block, and the blockade was performed on the side facing upward. A marker was placed on the back to indicate the location of the L2 spinous process, and the area was disinfected and draped.
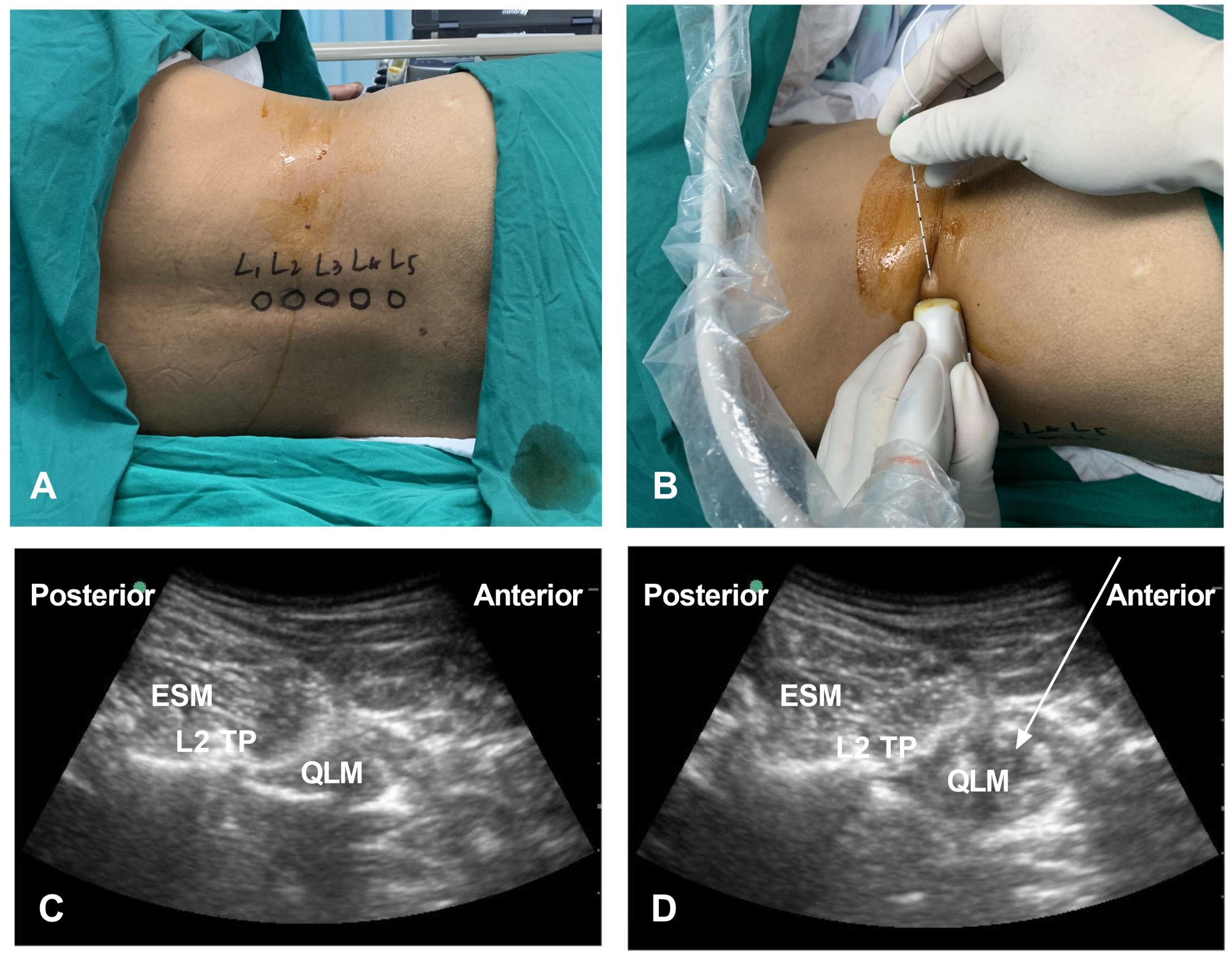
All volunteers received QLBi from an anesthesiologist with extensive experience in ultrasound-guided QLB. A sterile cover was placed over a low-frequency 3–6 MHz convex probe (SonoSite X-Porte, SonoSite Inc., Bothell, WA, USA), and the probe was positioned on the side of the blockade. The 12th rib was first identified with an ultrasound probe, and the L1, L2, L3, L4, and L5 spinous processes were identified by moving the probe downward. (Fig. 1A) The L2 transverse process and quadratus lumborum muscle were identified at the L2 level. The transverse process was located laterally, while the quadratus lumborum muscle was located dorsally, and the psoas major muscle was located ventrally. The needle was introduced in-plane, and a 0.7 mm*80 mm needle (Zhejiang Kangdelai Medical Equipment Co., Ltd., 0.7*80 TWLB) was inserted 1 cm from the probe. (Fig. 1B) After the needle reached the quadratus lumborum muscle, 1–2 ml of normal saline was injected to confirm the location, followed by an injection of 20 ml of 0.5% ropivacaine (batch no. LAYY. AstraZeneca, Cambridge, UK). The level of the block was evaluated by an ice test 1 h after injection (Fig. 1CD).
Fig. 1
Photograph and ultrasonographic images of the QLBi. (A) L2 level positioning; (B) Ultrasound probe positioning and puncture method; (C) Ultrasound image before puncture; (D) Ultrasound image after puncture. ESM: Erector Spinae Muscle; QLM: Quadratus Lumborum Muscle; TP: Transverse Process. Arrows indicate the trajectory direction of the needle tip
The medication used for QLBi in this study was prepared by an anesthesiologist who did not participate in the anesthesia procedure or postoperative assessment. After the area of the block was confirmed, general anesthesia was induced via a laryngeal mask. The anesthetic technique used was intravenous general anesthesia with oxygen supplied through a facemask. Anesthesia was induced with rocuronium (0.15 mg/kg), fentanyl (3–5 µg/kg), and propofol (1–2 mg/kg). A laryngeal mask was inserted when the corneal reflex disappeared, the jaw was relaxed, and mechanical ventilation was initiated. Propofol and remifentanil were administered via a pump during surgery to maintain anesthesia. The doses were adjusted based on changes in the volunteer’s blood pressure and heart rate. At the end of the operation, 50 mg of flurbiprofen was intravenously administered before the abdomen was closed.
Outcome measuresCutaneous sensory blockade area [20]After the blockade, various lines on the abdomen were marked: the midline in the front and back, the vertical line passing through the anterior superior iliac spine, the axillary posterior line, the horizontal line through the navel, the rib line, the iliac crest line, the greater trochanter of the femur, and the ischial tuberosity.
One hour after the blockade, ice was applied at a rate of 2 cm/s to determine the distribution of sensory loss on the trunk skin from the midline in the front to the midline in the back. The ice was moved and marked when the volunteer’s skin sensation changed from 2 to 1 or from 1 to 0 (according to the skin temperature blockage, there were three levels: level 2 represented normal sensation, level 1 represented cold sensation reduction, and level 0 represented cold sensation loss). The cold sensation-reduced area was connected with a solid blue line. The cold sensation loss area is connected with a solid red line.
The distribution area of sensory reduction or loss on the trunk skin was covered with a colorless transparent square film, and the trunk skin sensory blockade image and the marked lines were transferred to the transparent film. The pixel size of the scanned image (fixed pixels) was set, a scanner (Bizhub Press c7000) was used to convert the prepared transparent film into a digital image, which was saved in JPG format on a computer.
Duration of blockadeThe cold sensation was tested every hour after the surgery. The testing method was the same as before, and testing continued until the sensation was the same as that on the contralateral side. The duration of the blockade is defined as the time when the cold sensation returns to normal.
Analgesic Effect and Adverse Reactions.
Visits were made to the volunteers at 2, 4, 8, 12, and 24 h after surgery. The time when the patient first felt pain and the use of analgesics within 24 h were recorded. The NRS score of the volunteer was recorded at each time point after the surgery. A score of 0 indicates no pain, and a score of 10 indicates extreme pain. Adverse reactions, including hypotension, nausea and vomiting, and decreased muscle strength in the lower limbs, were recorded. Hypotension was defined as a decrease in systolic blood pressure of more than 30% from before surgery.
Statistical analysisSPSS 22.0 software was used for statistical analysis. Height, weight, age, and action time are expressed as the mean ± standard deviation, and other data are expressed as the median and interquartile range. GraphPad Prism 8 was used to create the figures.
留言 (0)