In this prospective cohort study, we explored the association between DAL and HDPs, including preeclampsia, chronic HTN, and GHTN. Our findings provide novel insights into the complex association between DAL and these adverse pregnancy outcomes, particularly emphasizing the significance of both high and low extremes of DAL in the risk of developing these conditions.
The association between DAL and preeclampsia, a major concern during pregnancy, yielded significant results. Our study demonstrated a notable statistical and clinical association between the dietary PRAL scale and the incidence of preeclampsia. Specifically, the probability of developing preeclampsia was 87% higher in the first quartile and 101% higher in the third quartile of PRAL compared to pregnant women in the second quartile. Additionally, the risk of developing preeclampsia in the third quartile of PRAL was 14% higher than in the first quartile, indicating that both higher and lower DALs may increase the risk of preeclampsia. However, our study did not reveal a consistent association for the fourth quartile of PRAL. Several factors, such as physiological changes during pregnancy, potential imprecision in DAL assessment, and limited statistical power due to the low incidence of preeclampsia, may account for this inconsistency. Moreover, while the crude and multivariable analysis of the NEAP scale did not indicate a significant association with preeclampsia, the continuous analysis of PRAL did not reveal a significant linear association either, suggesting that the association between DAL and preeclampsia may be non-linear and influenced by specific dietary thresholds rather than a gradual increase in risk across the spectrum of PRAL scores.
Our investigation into chronic HTN revealed a clearer association with DAL. Both extremes of PRAL and NEAP were significantly associated with an increased risk of chronic HTN. Participants in the lowest and highest PRAL quartiles, as well as the highest NEAP quartile, exhibited a markedly higher risk of developing chronic HTN compared to those in the second quartile. Moreover, a significant linear association was observed in the continuous analysis for both PRAL and NEAP, reinforcing the robustness of our findings and suggesting a direct impact of DAL on chronic HTN risk.
Similarly, the analysis of DAL in relation to GHTN also demonstrated significant associations in the extreme quartiles of PRAL and NEAP, with higher risks observed in the lowest and highest quartiles compared to the reference group. Interestingly, as with preeclampsia, the continuous analysis did not reveal a significant linear association between DAL and GHTN, further highlighting the possibility of a threshold effect in the association between DAL and HDPs outcomes.
These findings collectively indicate that the association between DAL and HDPs is complex and likely influenced by specific dietary patterns that create either high or low acid loads. The increased risk observed at both extremes of DAL underscores the importance of maintaining a balanced diet during pregnancy, as both excessive and insufficient acid-producing foods may contribute to adverse HDPs outcomes. Further research is needed to elucidate the underlying mechanisms driving these associations and to establish clear dietary guidelines for pregnant women to mitigate the risk of HDPs. Overall, our findings suggest that it may be beneficial for pregnant women to follow a standardized dietary regimen with consistent levels of DAL, avoiding both extremes, to reduce the likelihood of developing these conditions.
Numerous studies have been carried out over the past decades to examine the association between prenatal and pre-pregnancy dietary habits and negative outcomes in pregnancy and neonatal health. The results of these investigations, however, have varied and lacked consistency. This research marks one of the initial attempts to assess the association between DAL and the development of HDPs. The impacts of maternal DAL on pregnancy-related complications are not yet fully understood. While prior studies in non-pregnant populations have yielded inconsistent results regarding the impact of DAL on HTN risk, this investigation contributes novel insights. Hajianfar et al. suggested that high dietary PRAL and NEAP both have a protective effect against the odds of developing preeclampsia while being associated with pregnancy-related complications such as intrauterine growth restriction and a significant increase in SBP and DBP. This protective effect was associated with glutamine, a non-essential amino acid [34]. This theory contains several inaccuracies and unfounded conclusions. First, the association between glutamine intake and preeclampsia risk is not supported by strong evidence. While glutamine plays various roles in the body, the claim that adequate glutamine consumption diminishes the risk of muscle degradation and inflammatory reactions in pregnant women is not well-substantiated. Second, the argument oversimplifies the complex etiology of preeclampsia, which involves multifactorial and often poorly understood mechanisms. Third, although previous evidence has linked HDPs, particularly preeclampsia, with IUGR, this study indicates that a high DAL regimen heightened the risk of IUGR while simultaneously reducing the likelihood of developing preeclampsia. Furthermore, smoker were excluded from the study without providing a clear rationale for the exclusion. Tielemans et al. reported a null association between dietary PRAL, NEAP, vegetable or animal protein/potassium ratio, and the risk of developing HDPs. Based on this study, a higher vegetable protein/potassium ratio can alleviate DBP due to less sulfur content in vegetable proteins [35]. In this study, participants provided their medical histories through self-reporting without any accompanying documentation, raising concerns about the accuracy of the data. Two notable limitations of the aforementioned studies are the use of odds ratios to compare NEAP and PRAL quartiles, acknowledging that in non-rare outcomes, the odds ratio can exaggerate and magnify the findings. Also, a lack of exclusion for women adhering to specific dietary regimens or taking supplements. Additionally, the statistical analysis did not incorporate a causal approach.
Delving into the literature, some meta-analyses have demonstrated dietary PRAL association with hypertensive disorders in non-pregnant populations. For instance, Parohan et al. reported a 20-unit increase in dietary PRAL values was associated with a 3% increase in the risk of HTN [36]. Studies that did not find a significant association tended to be of lower quality compared to those that found a positive association [36]. Out of the nine studies in Parohan et al.‘s meta-analysis that found a non-significant or inverse association between NEAP and HTN, six included fewer than 10,000 participants without any control for energy intake and BMI [36]. On the other hand, among the two studies that found a positive association, both had a sample size of 10,000 individuals or more, and one controlled for energy intake and BMI [36]. Daneshzad et al. indicated the association between high DAL with 1.74 and 0.75 mmHg increase in SBP and DBP, respectively [37]. Chen et al.‘s meta-analysis showed a strong association between dietary PRAL and NEAP with essential HTN, reporting that higher dietary PRAL had a positive impact on increasing SBP and DBP, and a higher NEAP increased the odds of developing HTN by about 35% [38]. Additionally, Dehghan et al. demonstrated that despite NEAP, the highest dietary PRAL category was associated with a 0.98 mmHg increase in SBP and 0.61 mmHg in DBP [39].
As body homeostasis is a balance of intricate mechanisms and varies from one individual to another, the impact of DAL could be modulated by multiple factors. Genetic predisposition, overall health status, lifestyle choices, and other complexities may substantially shape these outcomes. There are several proposed mechanisms through which metabolic acidosis might elevate blood pressure. The association between acid–base equilibrium and increased blood pressure could be due to the absorption impairment of blood pressure-lowering essential minerals (i.e. calcium and magnesium) induced by metabolic acidosis [40]. High DAL has been shown to increase calcium and magnesium urinary excretion while lowering intracellular potassium [40]. To compensate for the intracellular loss of potassium, through a flawed cycle, sodium is dragged into the cell which eventually triggers HTN [41, 42].
High DAL could trigger the renin-angiotensin-aldosterone system (RAAS), inducing the body to retain sodium and cause vasoconstriction, potentially contributing to the onset or worsening of HTN. This reaction is thought to be a way of compensating for acid-base disruptions. McCarty et al. proposed that high DAL could activate the renin-angiotensin hormone system through the glutaminase enzyme [43]. Moreover, Armin et al. in a randomized clinical trial design of a low dietary PRAL regimen on 80 type II diabetes patients demonstrated potential benefits for blood pressure regulation, indirectly indicating the involvement of the RAAS [44].
Endothelial dysfunction, oxidative stress, and inflammation are well-known common pathophysiologies of preeclampsia that can result from high DAL. Mazidi et al. indicated in a population of 4,864 participants aged 40–85 years, after adjustment for main clinical and anthropometrical confounders, high dietary PRAL could be associated with 31% higher odds of peripheral artery disease through endothelial dysfunction resulting from oxidative stress and inflammation [45]. Wu et al., in a cross-sectional setting of 3,042 breast cancer survivors, indicated the highest quartiles of DAL had a 30–33% increase in c-reactive protein (CRP), which is a marker of inflammation [46]. Varkaneh et al. designed a cross-sectional study of 185 type II diabetes mellitus patients to evaluate the association of high DAL with inflammatory biomarkers. Patients in the highest tertile had significantly higher tissue necrosis factor-α (TNF-α) levels [47]. On the other hand, Farhangi et al., in 454 patients undergoing coronary artery bypass surgery, found a null association for CRP while Jafari reported an inverse association between high DAL and TNF-α [48, 49]. In their study, Jafari et al. mentioned that they did not take into consideration the use of anti-inflammatory drugs or supplements, as well as the overall quality of the participants’ diets [48].
A surge in DAL can result in heightened ammonia production in the proximal tubule of the kidney and a corresponding increase in acid removal. A decrease in functioning nephrons essentially due to ammonia harm in the kidneys - leads to a greater demand for acid removal per nephron [50]. This need triggers higher rates of ammonia production, significant increases in intra-medullary ammonium levels, and boosts in hormones such as angiotensin II, aldosterone, and endothelin-1 which all play key roles in expediting acid excretion [50]. Moreover, metabolic acidosis resulting from high DAL could trigger inflammation and endothelial dysfunction which are key features associated with the onset of preeclampsia [51]. Additionally, another proposed pathophysiology of high DAL in the development of HDPs is via hyperuricemia. Esche et al. reported reduced urate transport through the proximal tubule in high quintiles of DAL leading to hyperuricemia [52]. Hyperuricemia and systemic metabolic acidosis boost serum cortisol levels, which induces vasoconstriction [53]. Moreover, hyperuricemia has been shown to induce local and systemic arterial stiffness, which plays a key role in the development of HTN [54]. The acid-base balance plays a crucial role in regulating the excretion of urinary citrate [55]. Metabolic acidosis induced by high DAL increases the reabsorption of citrate within the nephrons and subsequently reduces citrate excretion [52, 55]. This process might affect blood pressure in salt-sensitive individuals by influencing citrate levels. Additionally, metabolic acidosis may independently impact blood pressure through an elevated serum anion gap [56]. However, the exact underlying pathway for this effect remains unclear.
The strengths of our study lie in the casualty approach with consideration of potential confounders in a large, prospective, population-based design. Another strength of our analysis is that we utilized RRs to compare non-rare outcomes, such as preeclampsia, across different quartiles of DAL. However, limitations include the use of a somewhat imprecise FFQ for estimating DAL, the absence of information on kidney function, and direct blood/urine acidity measurement. Future research could explore urinary biomarkers, such as pH, nitrogen, and potassium, in addition to dietary assessments, to elucidate the potential influence of DAL on preeclampsia development during pregnancy.
Further investigations could prioritize mechanistic designs to evaluate urinary pH, urinary nitrogen, and urinary potassium levels as additional indicators of DAL, alongside dietary assessment. The inclusion of these biomarkers in research endeavors may offer enhanced evidence regarding the potential influence of DAL on the incidence of HTN during pregnancy. Further longitudinal cohort designs with larger sample sizes and a diverse population could provide better public clinical judgment.
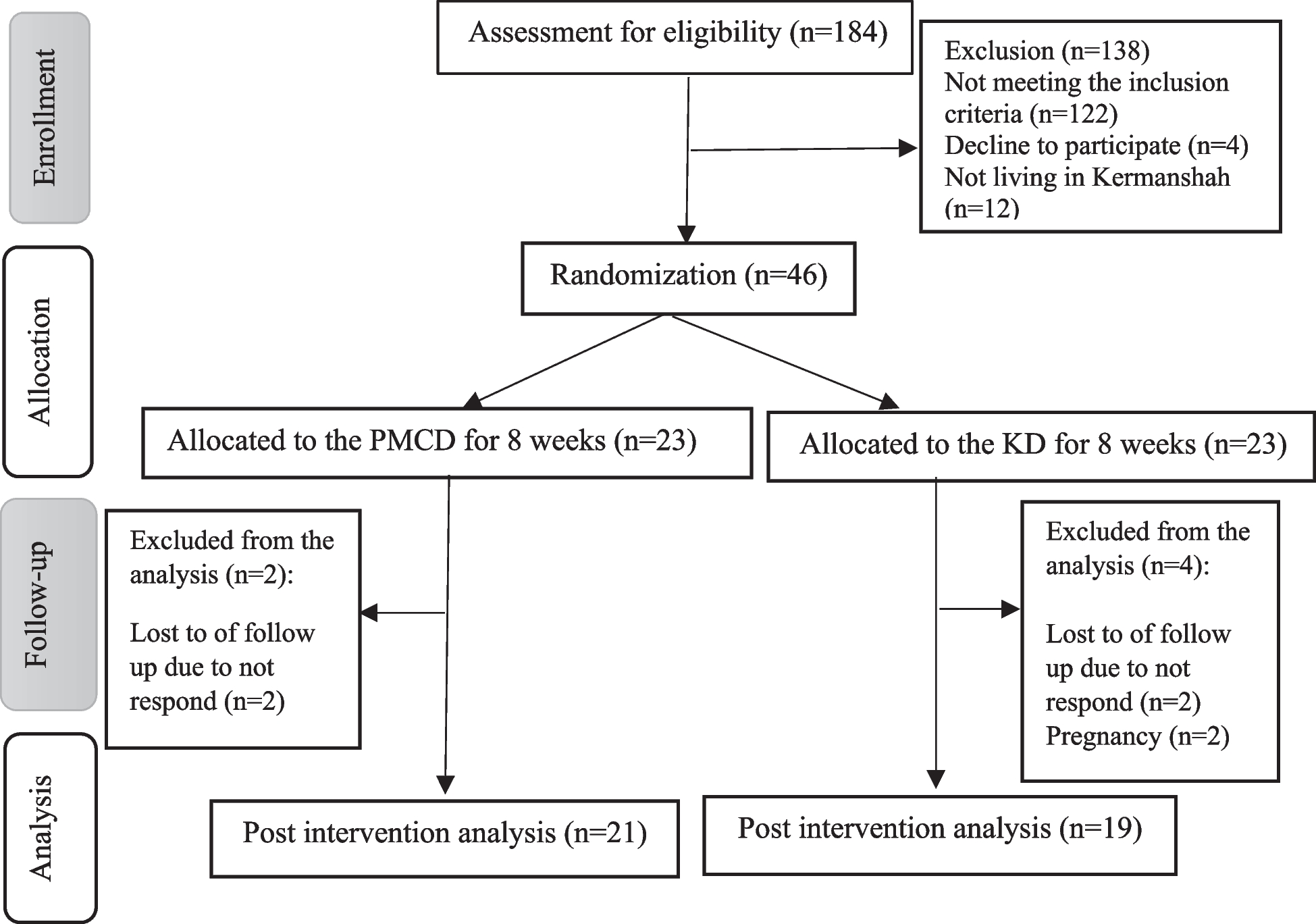
One notable limitation of our study is the relatively high rate of loss to follow-up and participant withdrawal. Unfortunately, we do not have comprehensive data regarding whether the women who withdrew or were lost to follow-up developed preeclampsia. Additionally, we lack detailed information on baseline characteristics for these non-completers, which precludes us from assessing potential differences between those who completed the study and those who did not. This missing data could introduce bias, as it is unclear whether the reasons for dropout are related to the study outcomes or if they might have systematically differed in ways that could impact the study’s findings. Future studies should aim to reduce loss to follow-up through enhanced participant retention strategies and ensure comprehensive data collection to allow for a more thorough analysis of the impact of attrition on study outcomes.




留言 (0)